Cardiac patient posted for non cardiac surgery
Reading File
Finding Sources
Finding Sources
Searching PubMed
"non-cardiac surgery" AND "cardiac risk" AND "preoperative evaluation"
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the essential content needed. Let me compile a comprehensive, well-structured answer.
Cardiac Patient Posted for Non-Cardiac Surgery
The perioperative management of a cardiac patient undergoing non-cardiac surgery requires systematic stepwise assessment to minimize the risk of Major Adverse Cardiac Events (MACE). Myocardial infarction is the leading cause of both early and late postoperative deaths in this population.
Step 1 - Emergency vs. Elective Surgery
The very first decision:
- Emergency surgery: Proceed directly to the operating room with optimization of monitoring and medical therapy intraoperatively. No time for extensive risk stratification.
- Elective/urgent surgery: Proceed with full stepwise cardiac assessment below.
Step 2 - Identify Active Cardiac Conditions (Absolute Contraindications to Elective Surgery)
These must be evaluated and stabilized BEFORE proceeding:
| Condition | Action |
|---|---|
| Acute Coronary Syndrome (NSTEMI/STEMI) | Treat per ACS guidelines first |
| Decompensated Heart Failure | Stabilize medically |
| Significant arrhythmias (high-grade AV block, symptomatic bradycardia, uncontrolled SVT) | Rate/rhythm control |
| Severe symptomatic valvular disease (especially severe aortic stenosis) | Evaluate for intervention |
| Unstable/severe angina | Optimize medically |
Step 3 - Surgical Risk Stratification
Risk varies by the type of surgery:
| Risk Category | Examples | MACE Risk |
|---|---|---|
| Low | Endoscopic, superficial, cataract, breast | <1% |
| Intermediate | Intraabdominal, intrathoracic, orthopedic, prostate, head/neck | 1-5% |
| High | Vascular (aorta, peripheral), emergent major | >5% |
- Low-risk procedures: proceed without further cardiac testing.
- Intermediate/high risk: continue to Steps 4 and 5.
Step 4 - Estimate MACE Risk Using Risk Indices
Revised Cardiac Risk Index (RCRI) - Lee Index (1999)
The most widely used and validated tool (endorsed by ACC/AHA, ESC, ESA).
Assigns 1 point each for:
- High-risk surgery (intraperitoneal, intrathoracic, suprainguinal vascular)
- History of ischemic heart disease (prior MI, angina, positive stress test, pathological Q waves, nitrate use)
- History of congestive heart failure (PND, pulmonary edema, S3 gallop, LV failure on exam)
- History of cerebrovascular disease (TIA or stroke)
- Insulin-dependent diabetes mellitus
- Preoperative creatinine >2.0 mg/dL
RCRI Score and Predicted MACE Risk:
| Score | Risk of Major Cardiac Events |
|---|---|
| 0 | ~0.4% |
| 1 | ~0.9% |
| 2 | ~7% |
| ≥3 | ~11% |
Patients with RCRI ≥3 are at very high risk and may benefit from noninvasive stress testing or modification of management.
Other Risk Calculators
- ACS NSQIP MICA Calculator (online at riskcalculator.facs.org): uses age, functional status, ASA class, creatinine, and surgery type
- AUB-HAS2 Index: heart disease history, symptoms of heart disease (angina/dyspnea), age ≥75, anemia (Hb <12), vascular/emergency surgery
Step 5 - Functional Capacity Assessment
Expressed in Metabolic Equivalents (METs):
| Functional Capacity | Examples | METs |
|---|---|---|
| Poor | Cannot climb one flight / walk on level | <4 METs |
| Moderate-Good | Climb stairs, walk on level at 4 mph, carry 15-20 lb objects, golf, doubles tennis | ≥4 METs |
| Excellent | Strenuous sport, heavy physical labor | >10 METs |
- ≥4 METs: Generally proceed to surgery without further noninvasive testing.
- <4 METs or unknown: Consider pharmacological stress testing only if results would change management or perioperative care.
Step 6 - Preoperative Noninvasive Cardiac Testing
Indications are selective - NOT for all patients. Options include:
- Dobutamine stress echocardiography (DSE)
- Myocardial perfusion imaging with pharmacological stress (dipyridamole, adenosine, regadenoson) with Thallium-201 or Tc-99m
- Exercise ECG stress test (if patient can exercise and resting ECG is interpretable)
Evidence for widespread preoperative noninvasive testing in all patients undergoing major surgery is lacking. Test only when results would alter clinical management.
Step 7 - Perioperative Medical Interventions (the algorithm)
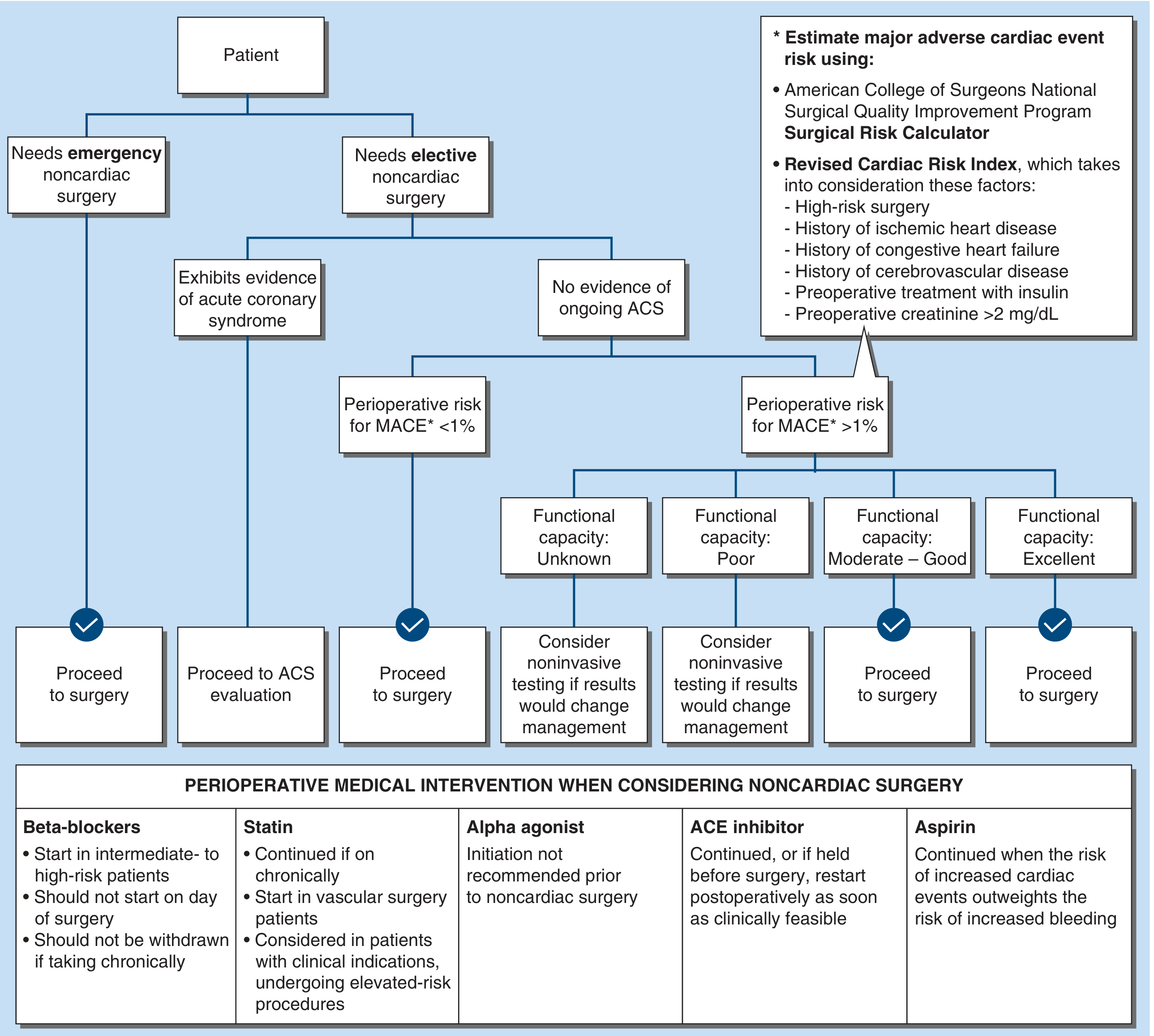
Beta-blockers
- Continue if already on chronic beta-blocker therapy - do NOT withdraw perioperatively (withdrawal increases risk of ischemia/arrhythmia)
- Do NOT initiate on the day of surgery
- Consider initiating in intermediate- to high-risk patients (ideally days to weeks before surgery to assess tolerability), particularly those with ≥3 RCRI risk factors or intermediate/high-risk ischemia on stress testing
- Titrate to heart rate 60-80 bpm
Statins
- Continue if patient is already on a statin - associated with reduced perioperative cardiac complications
- Initiate in patients undergoing vascular surgery (regardless of clinical risk)
- Consider initiation in intermediate-/high-risk non-vascular procedures, though recent trial evidence (LOAD trial: atorvastatin 80 mg loading) showed no benefit in statin-naive patients
ACE Inhibitors / ARBs
- Continue if used for heart failure or hypertension management
- If held before surgery, restart as soon as clinically feasible postoperatively
Antiplatelet Therapy (Coronary Stents)
This is a critical consideration:
| Stent Type | Minimum DAPT Duration Before Elective Surgery |
|---|---|
| Bare Metal Stent (BMS) | 30 days |
| Drug-Eluting Stent (DES) - for stable IHD | 6 months |
| DES - post-ACS | 12 months |
- If P2Y12 inhibitor must be stopped: continue aspirin perioperatively, restart P2Y12 inhibitor ASAP postoperatively
- Timing of stopping before surgery: Clopidogrel - 5 days; Prasugrel - 7 days; Ticagrelor - 3-5 days
- Multidisciplinary decision-making (cardiologist + surgeon + anesthesiologist) is required
Alpha-2 Agonists (Clonidine)
- NOT recommended - POISE-2 trial showed clonidine increased nonfatal cardiac arrest and clinically important hypotension
Calcium Channel Blockers
- Insufficient evidence to recommend as prophylactic cardiac protection
SGLT-2 Inhibitors
- Generally hold perioperatively (risk of euglycemic DKA)
Step 8 - Coronary Revascularization Before Non-Cardiac Surgery
The CARP trial established that prophylactic coronary revascularization (CABG or PCI) before non-cardiac surgery in high-risk patients with peripheral vascular disease and significant CAD did NOT reduce overall mortality or perioperative MI, and caused significant delays and increased limb morbidity. Therefore:
- Routine preoperative revascularization is NOT recommended
- Revascularization should be considered only if it would be indicated independently of the upcoming surgery (e.g., left main disease, severe 3-vessel disease with poor LV function, ACS)
Special Considerations
Patients with Heart Failure
- Optimize volume status preoperatively
- Avoid fluid overload intraoperatively
- Monitor with invasive hemodynamic monitoring in severe cases
- BNP/NT-proBNP can guide risk stratification
Patients with Valvular Heart Disease
- Severe aortic stenosis: highest risk for perioperative cardiac events; consider valve replacement/TAVR before elective non-cardiac surgery if symptomatic
- Mitral stenosis: control heart rate, avoid tachycardia
- Regurgitant lesions: generally better tolerated
Patients with Arrhythmias / Pacemakers / ICD
- Ensure pacemaker is functioning
- For ICDs: discuss with electrophysiology team about intraoperative electromagnetic interference (electrocautery); consider reprogramming to asynchronous mode or deactivating tachycardia therapies during surgery
- Patients with implanted cardiac devices should have device interrogated within 6-12 months of major surgery
Patients with Pulmonary Hypertension
- High perioperative risk; requires specialist consultation
- Avoid hypoxia, hypercarbia, acidosis, and pain (all increase pulmonary vascular resistance)
Preoperative Investigations in Cardiac Patients
| Investigation | Indication |
|---|---|
| ECG | All cardiac patients preoperatively |
| Echocardiography | Known/suspected valvular disease, HF, new symptoms |
| Stress testing | Poor/unknown functional capacity + MACE risk >1% if results change management |
| BNP/NT-proBNP | Risk stratification in suspected/known HF |
| CBC | Expected major blood loss, symptoms of anemia, cardiac/pulmonary disease |
| Creatinine/electrolytes | Renal disease, diuretics, ACE inhibitor use |
| Coagulation | Anticoagulant use, liver disease |
| Glucose/HbA1c | Diabetes (cardiac risk factor) |
| CXR | Suspected pulmonary edema, known cardiac disease with new symptoms |
Intraoperative Considerations
- Monitoring: standard + invasive arterial line for high-risk patients; consider central venous access, TEE, pulmonary artery catheter in select cases
- Maintain hemodynamic stability: avoid hypotension (systolic BP <100 mmHg), tachycardia (HR >80), and prolonged hypoxemia
- Temperature regulation: hypothermia increases cardiac stress
- Regional anesthesia: may be preferable in selected patients (reduces sympathetic response, avoids general anesthesia-related myocardial depression)
- Continue beta-blockers intraoperatively
Postoperative Considerations
- ECG in the immediate postoperative period and at 24-48 hours in high-risk patients
- Troponin monitoring: rising troponin post-operatively (Myocardial Injury after Non-cardiac Surgery - MINS) is associated with worse outcomes
- Early mobilization to reduce DVT/PE risk
- Restart cardiac medications as soon as feasible
- Adequate pain control (reduces sympathetic activation)
Sources:
- Harrison's Principles of Internal Medicine 22E, Chapter 492 (Preoperative Evaluation and Perioperative Medicine)
- Goldman-Cecil Medicine, Chapter 399 (Cardiovascular Risk in Noncardiac Surgery)
- Sabiston Textbook of Surgery, Chapter 4 (Preoperative Assessment)
- Schwartz's Principles of Surgery 11E, Chapter 23 (Peripheral Arterial Disease)
- 2022 ESC Guidelines on Cardiovascular Assessment and Management for Noncardiac Surgery
This is a shared conversation. Sign in to Orris to start your own chat.