Medial tibial defect in tka
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tibial defect" AND "total knee arthroplasty"
Reading File
Finding Sources
Finding Sources
Searching PubMed
"tibial bone defect" AND "knee arthroplasty"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive content from Campbell's Operative Orthopaedics (2026 edition) to provide a thorough answer. Let me compile this into a well-structured response.
Medial Tibial Defect in Total Knee Arthroplasty (TKA)
Medial tibial bone defects are the most common tibial defects encountered in TKA, arising almost always from chronic varus deformity with erosion of the medial tibial plateau. Managing them correctly is fundamental to achieving stable, well-aligned prosthetic fixation.
Etiology / Why the Medial Side?
Medial tibial bone loss occurs due to:
- Varus osteoarthritis (most common) - years of medial compartment overloading erode the medial tibial plateau
- Osteonecrosis of the medial plateau
- Previous proximal tibial osteotomy (HTO) - which can remove proximal tibial bone stock
- Trauma (post-tibial plateau fracture)
- Condylar hypoplasia
- Revision TKA - prior loosening, implant failure, or infection
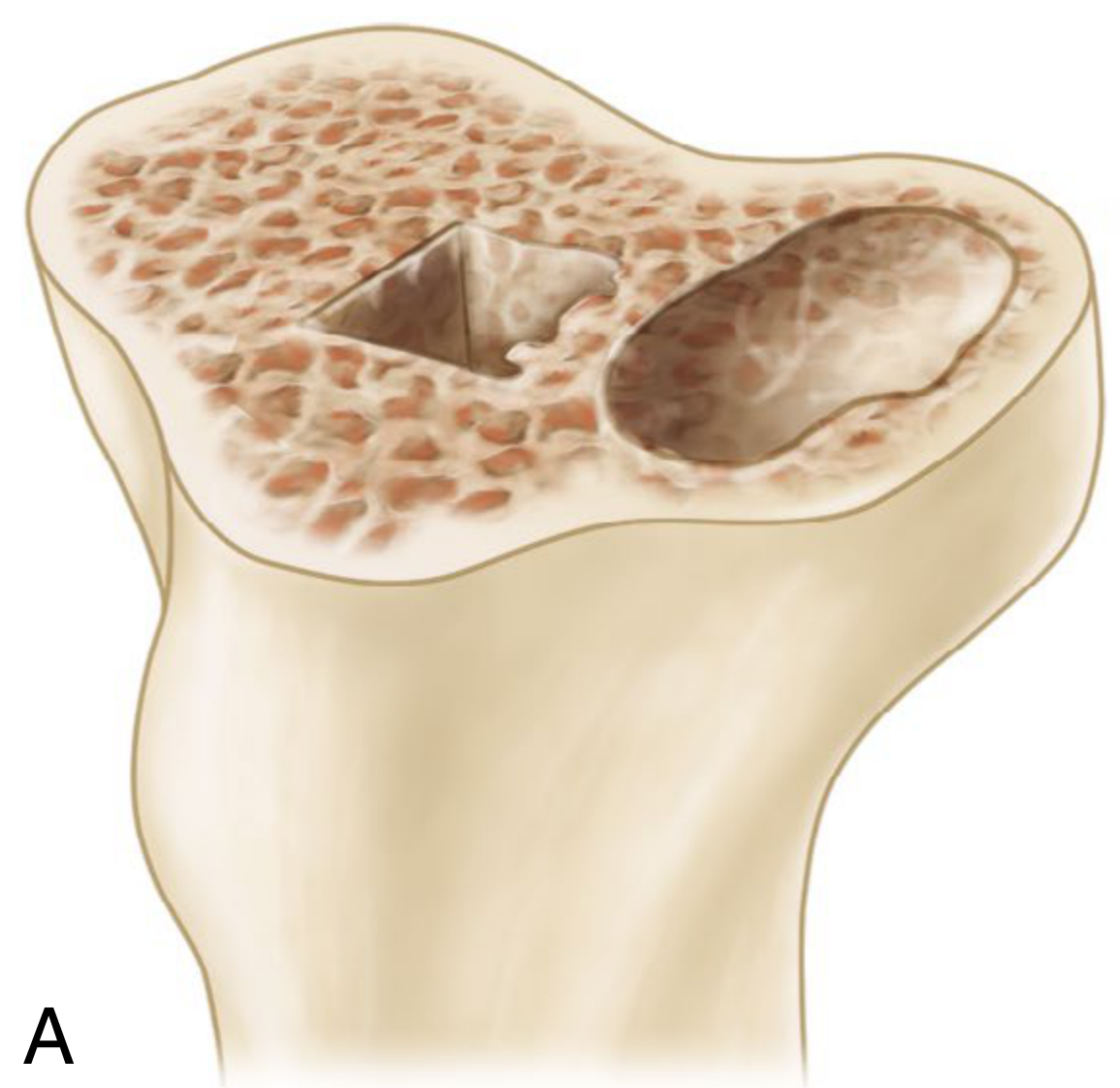
Classification of Tibial Bone Defects
Rand Classification (morphology-based)
| Type | Description |
|---|---|
| Type I | Focal metaphyseal defect with intact cortical rim (contained/cavitary) |
| Type II | Extensive metaphyseal defect with intact cortical rim |
| Type III | Combined metaphyseal and cortical defect (noncontained/segmental) |
AORI Classification (Anderson Orthopaedic Research Institute)
Tibial defects are graded T1, T2, T3:
- T1: Minor bone loss, tibial metaphysis intact - routine technique sufficient
- T2: Damaged metaphysis involving one (T2A) or both (T2B) condyles
- T3: Deficient tibial metaphysis, possibly requiring structural augmentation
The AORI system mirrors a parallel femoral classification (F1-F3).
Practical morphologic distinction:
- Contained (cavitary) defects: intact cortical rim surrounds the defect - amenable to cement or impacted bone graft
- Noncontained (segmental/peripheral) defects: peripheral with no cortical rim - require structural augmentation
Treatment Options Based on Defect Size and Type
1. Cement Fill (Small Defects, <5 mm)
- Simplest option for small, contained defects
- Cement alone fills the void adequately
- No significant biomechanical compromise for minor defects
2. Screw-Augmented Cement (Larger Contained Defects)
- Cancellous or cortical screws placed into the defect bed, then PMMA fills around them
- Screws act as anchors and provide structural reinforcement
- In a series of 145 TKAs with medial tibial defects treated with screws + cement: only 2 medial collapses and 1 lateral collapse occurred (all in metal-backed components), with no revisions required
- 7-year follow-up in 25 knees showed no progression of tibial radiolucencies

3. Impacted Cancellous Bone Graft (Contained Defects)
- Suitable for cavitary contained defects
- Morsellized autograft or allograft packed into the defect
- Best results when the defect is contained and the graft can be compressed
4. Peripheral/Structural Bone Graft (Noncontained/Segmental Defects)
Windsor-Insall-Sculco Technique (Technique 8.10):
- Convert the irregular defect to a flat surface using a saw - minimal bone resection
- Attach autogenous bone from the distal femoral resection (or proximal tibia) to the flattened defect
- Secure with threaded Steinmann pins or cancellous screws
- Recut the upper tibial surface to a uniform flat plane
- Seal the graft-host junction with a small premixed cement batch before final cementing, to prevent cement extrusion into the graft-bone interface
- If graft apposition requires further bone removal, level the host surface with a burr for maximal graft-host contact
Key principles:
- Neutral alignment is essential - it directly affects graft survival and prosthesis loosening
- Intramedullary stem extensions on tibial (and often femoral) components are used routinely to protect peripheral bone grafts from stress
5. Modular Metal Wedges / Blocks
- Attached to the tibial tray to fill the defect geometrically
- Available in most modern TKA systems - allow intraoperative customization
- Reported: no tibial loosening in 22 knees observed at 3 years average
- Particularly useful for primary TKA with significant lateral or medial slope defects (e.g., post-HTO where the medial plateau is the more deficient side)
6. Porous Metal Cones and Sleeves (Severe/Revision Defects)
- Cones: press-fit into cavitary metaphyseal defects; implant is cemented into the cone to create a composite construct
- Sleeves: attached directly to the implant stem, forming a single-unit construct for contained defects
- Primarily used for revision cases with significant bone loss (AORI T2B/T3)
- Key advantage: cones can integrate biologically even if the overlying implant construct eventually fails
- Good reported results, though mostly in revision settings
Special Considerations
Post-HTO Cases
After a high tibial osteotomy, the tibial plateau is often oblique or maloriented. The medial side is usually more deficient. Metal block augmentation is commonly required, and offset stem placement may be needed due to residual deformity of the proximal fragment.
Alignment Restoration
Restoration of neutral mechanical alignment is the most critical principle in managing tibial defects. Malalignment substantially increases the risk of:
- Graft resorption
- Asymmetric loading and component subsidence
- Early loosening
Stem Extensions
- Used whenever condylar bone stock is tenuous
- Required with constrained condylar prostheses
- Protect grafts and augments by off-loading metaphyseal stress to the diaphysis
Summary Treatment Algorithm
| Defect Size/Type | Preferred Treatment |
|---|---|
| <5 mm, contained | Cement alone |
| 5-10 mm, contained | Impacted cancellous graft or screw-augmented cement |
| >10 mm, contained | Screw+cement or modular metal block/wedge |
| Noncontained/segmental (peripheral) | Structural autograft (Windsor technique) + stem; or metal block + stem |
| Massive (revision, AORI T3) | Porous metal cone/sleeve, structural allograft, or custom implant |
Sources:
- Campbell's Operative Orthopaedics, 15th Ed. 2026, Chapter 8 - Management of Bone Deficiency in TKA; Technique 8.10 (Windsor, Insall, Sculco); Revision TKA section
Recent literature note: A 2024 finite element study (PMID 38870990) found that stem extensions on the tibial component significantly reduce stress at the medial tibial bone-implant interface for medial defects, supporting the established practice of using stem extensions with augments or grafts. A 2025 case series (PMID 41438996) reported favorable short-term outcomes using robotic-assisted TKA with metal block augmentation for severe varus knees with tibial defects.
This is a shared conversation. Sign in to Orris to start your own chat.