Perianal hematoma
Reading File
Finding Sources
Finding Sources
Searching the Web
perianal hematoma clinical features management treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content. Let me compile the full answer.
Perianal Hematoma (Thrombosed External Hemorrhoid)
Terminology note: The term "perianal hematoma" is often used interchangeably with "thrombosed external hemorrhoid," though strictly speaking a perianal hematoma is a blood collection within the perianal skin, while a thrombosed external hemorrhoid involves clot formation within the external hemorrhoidal venous plexus. Clinically the distinction is minor - both present and are managed identically. The "thrombosed external pile" label is a misnomer.
Anatomy
External hemorrhoids arise from the external hemorrhoidal venous plexus below the dentate (pectinate) line, covered by perianal skin (somatic innervation - hence painful). This is why thrombosis of external hemorrhoids causes severe pain, unlike thrombosis of internal hemorrhoids (above the dentate line, visceral innervation).
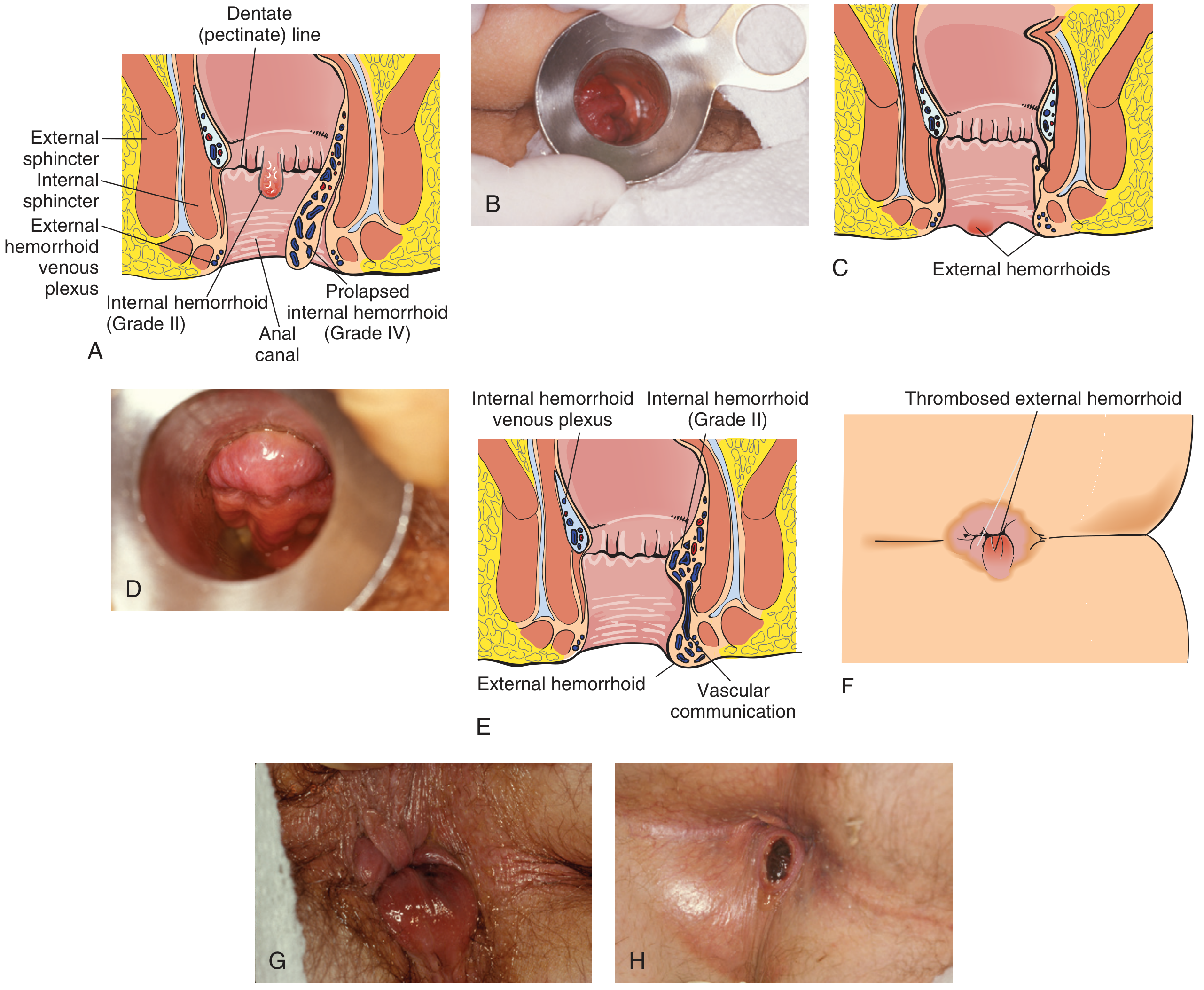
Pathophysiology
- Thrombosis occurs within the external hemorrhoidal plexus, forming a blood clot beneath the perianal skin
- Distention of the overlying perianal skin plus inflammation from the thrombotic process drives the pain
- Bleeding can occur if the overlying skin ulcerates and the liquefied, resolving hematoma extravasates
- After ~48-72 hours, the hematoma begins to liquefy and organise
Clinical Features
| Feature | Detail |
|---|---|
| Onset | Sudden, often after straining, heavy lifting, or prolonged sitting |
| Pain | Severe, constant perianal pain (unlike internal hemorrhoids) |
| Lump | Tense, tender, bluish-purple mass at the anal verge |
| Cannot be reduced | Cannot be pushed back inside (unlike prolapsed internal hemorrhoid) |
| Bleeding | May occur if skin overlying the hematoma ulcerates |
Differential diagnoses to exclude:
- Prolapsed/strangulated internal hemorrhoid (larger, more circumferential, covers the entire anus)
- Perianal abscess (fluctuant, fever, systemic signs)
- Anal melanoma - can mimic a thrombosed external hemorrhoid, but up to 25% are amelanotic; these metastasize early with 5-year survival of only 15-20%
Management
Conservative (if > 72 hours or mild symptoms)
Most thrombosed external hemorrhoids resolve within 48-72 hours on their own. Conservative treatment is appropriate if the patient presents late or has mild discomfort:
- Warm sitz baths 2-3 times daily
- Stool softeners (psyllium, docusate sodium/calcium) - to minimise straining and prevent aggravation
- Topical anesthetic ointments (e.g., lidocaine)
- Witch hazel-impregnated pads
- Oral analgesics (NSAIDs)
Conservative measures do resolve symptoms, but clinical improvement must be attributed with caution - most resolve spontaneously regardless.
Surgical (within 48-72 hours of onset, severe pain)
If the patient presents within 48-72 hours with severe pain, surgical evacuation or excision is indicated and offers:
- Immediate symptom relief
- Lower recurrence rate
- Longer remission intervals vs. conservative therapy
Excision is preferred over simple incision and drainage - excising the thrombus with overlying skin (leaving a wide-open wound) has a lower recurrence rate than I&D alone, because simple drainage allows the wound to seal over and the clot to reaccumulate.
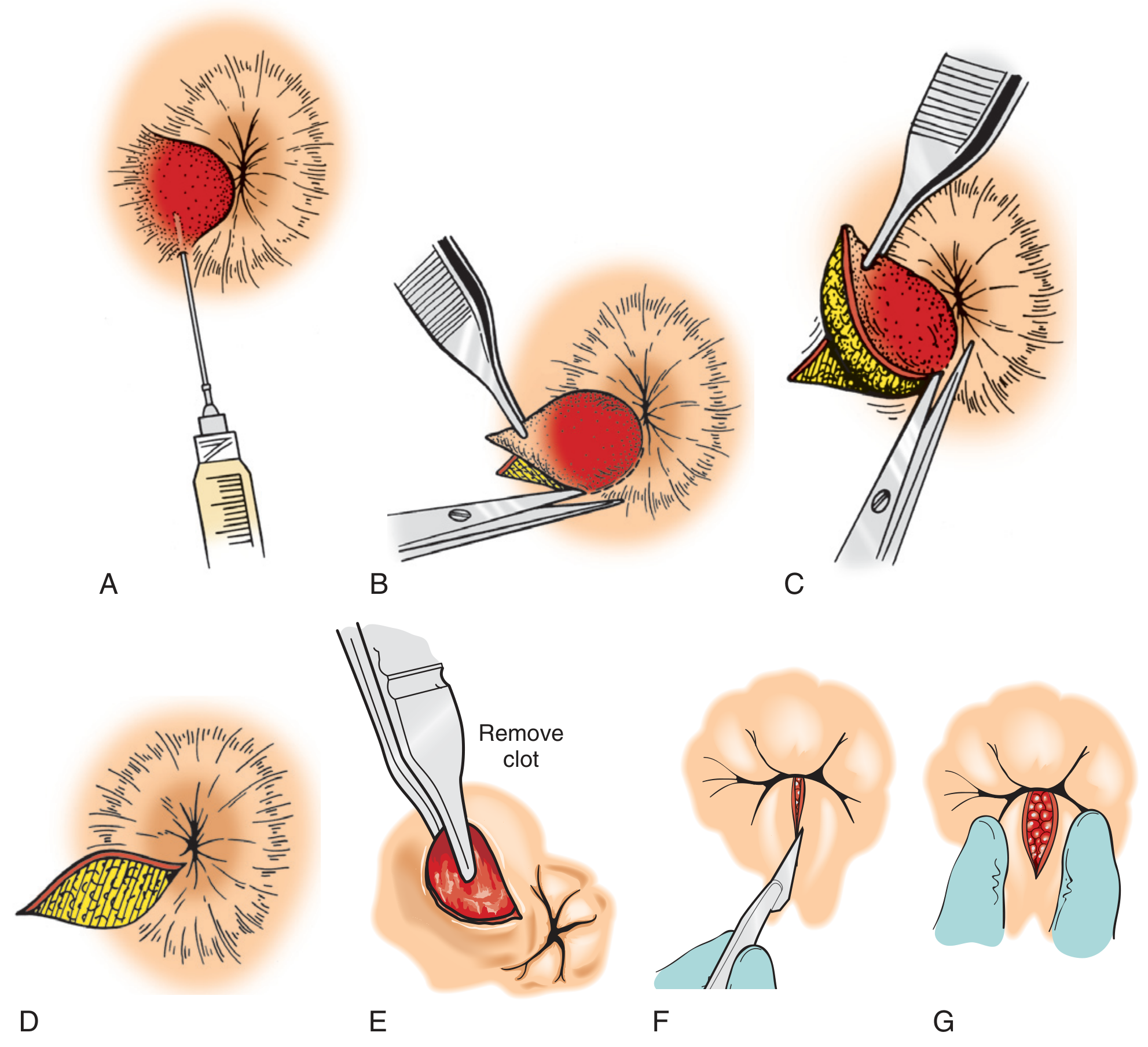
Technique (office procedure under local anaesthesia):
- Position: left lateral decubitus; perform digital and anoscopic exam
- Wipe the area with antiseptic
- Inject 2% lidocaine with epinephrine as a field block (avoid over-infiltrating, which tents up tissue excessively)
- Using a no. 15 scalpel blade, excise the thrombosed hemorrhoid with a small elliptical wedge of overlying skin
- Spread the incision to expose the base and remove all thrombi (multiple clots are common)
- Leave wound open or close with fine absorbable suture; control bleeding with Monsel's solution or cautery
- Apply antibiotic ointment mixed with 5% lidocaine ointment
After 72 hours - do NOT evacuate. The hematoma has begun to liquefy, and surgical intervention at this stage is associated with a high rate of bleeding. Continue conservative therapy.
Complications of the Procedure
- Pain (expected)
- Bleeding
- Infection / perianal abscess (< 1%)
- Chronic fissure
Post-Resolution: Skin Tags
After the clot resolves, the overlying skin may become redundant, leaving a perianal skin tag. These are generally asymptomatic but can cause hygiene difficulties and pruritus ani. Treatment is conservative; surgical excision only for persistent hygiene problems or significant patient distress.
Key Clinical Pearls
- Excision beats simple I&D - removes the clot chamber, preventing reaccumulation (Textbook of Family Medicine 9e; Greenspon et al., 2004, SOR: B)
- 72-hour window is critical - surgery before this point gives immediate relief; after this, conservative management is safer
- Don't confuse with internal hemorrhoid prolapse - external hemorrhoids cannot be reduced; prolapsed internal hemorrhoids can (sometimes)
- Melanoma mimicry - always consider anal melanoma in atypical or non-resolving "thrombosed hemorrhoids"
Sources: Yamada's Textbook of Gastroenterology 7e; Pfenninger and Fowler's Procedures for Primary Care 3e; Textbook of Family Medicine 9e; Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.