ECG
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive content. Now let me compile a thorough, well-organized response on all degrees of heart block.
AV Heart Blocks - ECG Guide
Source: Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine
What Is AV Block?
AV block is a disturbance of impulse conduction where the atrial impulse is conducted with delay or not at all to the ventricle when the AV junction is not physiologically refractory. The block site can be at the AV node, His bundle, or bundle branches. It must be distinguished from interference (normal refractoriness after a preceding impulse).
Classification by Degree
1st Degree AV Block
Definition: Every P wave conducts to the ventricle, but PR interval is prolonged > 200 ms (0.20 s).
ECG features:
- PR interval > 200 ms - can extend as long as 1000 ms in severe cases
- Regular rhythm - every P wave is followed by a QRS
- No dropped beats
Site of block:
- If QRS is narrow - delay is almost always in the AV node (prolonged A-H interval)
- If QRS shows BBB pattern - delay may be in AV node OR His-Purkinje system; requires His bundle electrogram to differentiate
Clinical note: Usually benign. Vagal tone (e.g., carotid massage) or rate acceleration can cause 1st degree to progress to 2nd degree Wenckebach.
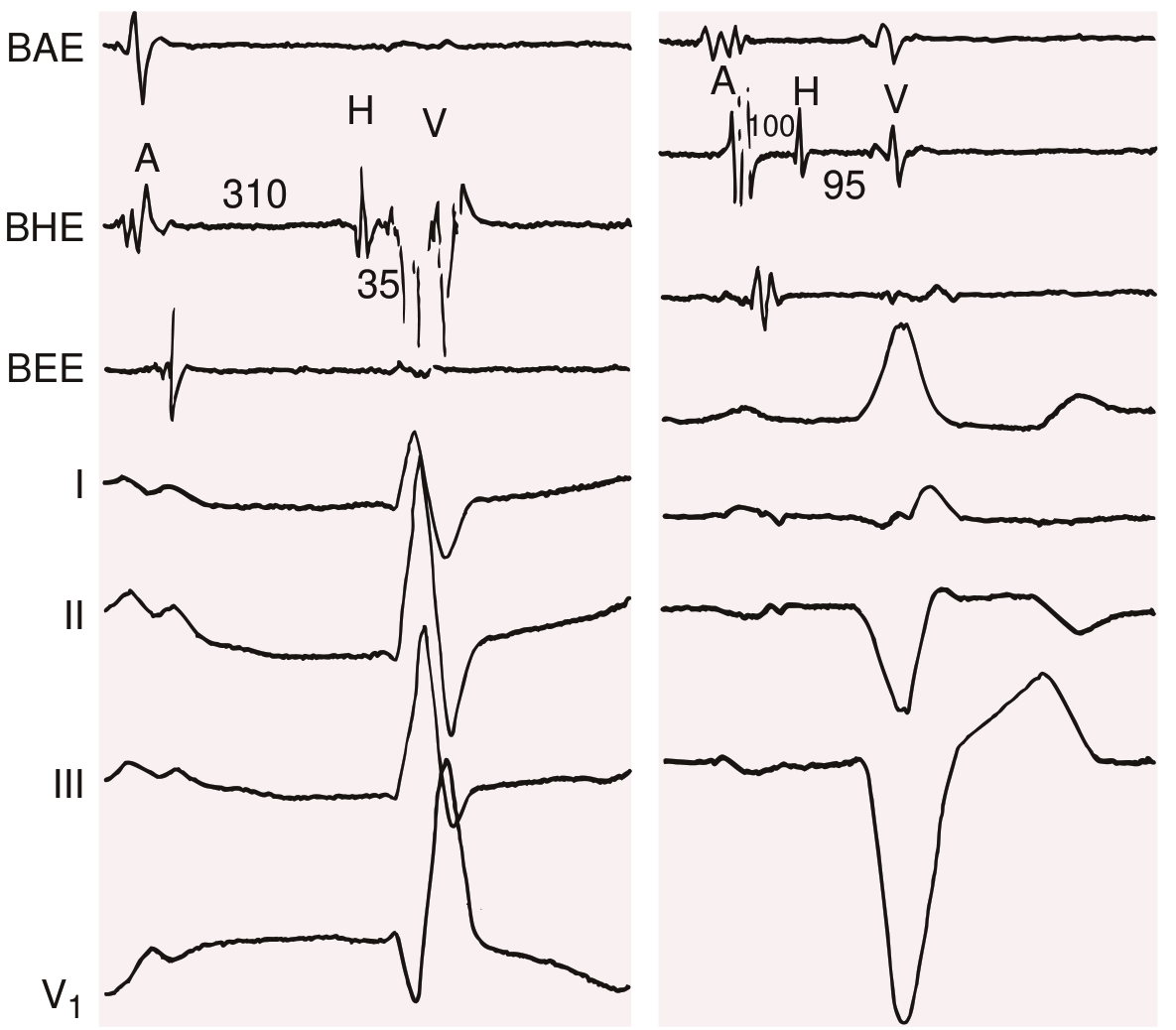
Fig 68.6 from Braunwald's: Left panel - RBBB with AV nodal delay (A-H 310 ms). Right panel - LBBB with His-Purkinje delay (H-V 95 ms)
2nd Degree AV Block
Some (not all) P waves fail to conduct to the ventricle. Two subtypes:
Mobitz Type I (Wenckebach) - 2nd Degree
ECG features:
- PR interval progressively lengthens from beat to beat
- The RR interval shortens progressively (because each PR increment is smaller than the last)
- A P wave is eventually dropped (not followed by QRS)
- The pause after the dropped beat is less than twice the shortest PP interval
- After the dropped beat, the cycle resets and PR shortens again
Ladder diagram - 4:3 Wenckebach cycle:
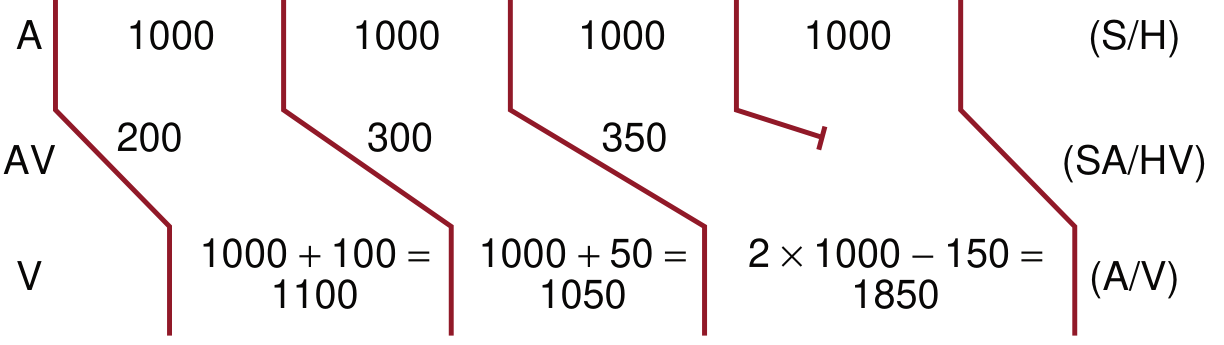
P-P = 1000 ms, PR goes 200 → 300 → 350 ms → blocked. Note: RR shortens (1100 → 1050) then long pause (1850 ms)
Memory aid for Wenckebach (PRWP mnemonic):
- PR gets longer, longer, longer...
- RR gets shorter, shorter, shorter...
- Will drop a beat
- Pause, then repeats
Site: Usually the AV node. Benign in most settings (especially inferior MI or athletes).
Mobitz Type II - 2nd Degree
ECG features:
- PR interval is constant (no progressive lengthening)
- A P wave is suddenly not conducted without warning
- The pause containing the dropped beat is exactly twice the PP interval
- QRS is often wide (BBB pattern), reflecting infranodal disease
Key distinction from Type I:
| Feature | Mobitz I (Wenckebach) | Mobitz II |
|---|---|---|
| PR before dropped beat | Progressively longer | Constant |
| QRS width | Usually narrow | Usually wide |
| Site of block | AV node | His bundle / bundle branches |
| Clinical risk | Lower | Higher - prone to complete block |
| Response to atropine | Usually responds | Unpredictable / poor |
| Pacing needed? | Rarely (unless symptomatic) | Yes - permanent pacing often needed |
Site: Infranodal - His bundle or bundle branches. Clinically more serious because it can progress unpredictably to complete (3rd degree) block.
High-Grade (Advanced) AV Block
When 2 or more consecutive P waves are blocked (e.g., 3:1 or 4:1 block). This is an intermediate category between 2nd and 3rd degree. The conducted beats may have a constant PR, and the ventricular rate can be very slow.
3rd Degree (Complete) AV Block
Definition: No atrial impulses conduct to the ventricle. Atria and ventricles are completely dissociated.
ECG features (from Tintinalli's Emergency Medicine):
| Feature | Finding |
|---|---|
| P wave - QRS association | None - completely dissociated |
| Atrial rate vs. ventricular rate | Atrial rate greater than ventricular rate |
| Ventricular rhythm | Regular (escape rhythm is regular) |
| QRS morphology | Usually widened (junctional escape = narrow; ventricular escape = wide) |
Escape rhythms:
- AV nodal / junctional escape: Rate 40-60 bpm, narrow QRS - block is at or above His bundle
- Ventricular escape: Rate 20-40 bpm, wide QRS - block is infranodal (bundle branch level); less reliable, hemodynamically worse
AV dissociation vs Complete Heart Block:
- Complete heart block is one cause of AV dissociation, but they are not synonymous
- In AV dissociation from enhanced automaticity, the ventricular rate may be faster than the atrial rate (isorhythmic dissociation); in complete heart block, the atrial rate is always faster
Common Causes Summary
| Block Type | Common Causes |
|---|---|
| 1st degree | Vagal tone, athletes, inferior MI, digoxin, beta-blockers, calcium channel blockers, myocarditis |
| 2nd degree Mobitz I | Inferior MI (RCA lesion), increased vagal tone, drug effects (digoxin, opioids), myocarditis |
| 2nd degree Mobitz II | Anterior MI, degenerative conduction system disease (Lev's/Lenegre's disease), cardiomyopathy, surgical trauma |
| 3rd degree (complete) | Inferior MI (often temporary), anterior MI (often permanent), Lyme carditis, congenital, degenerative, surgical |
Management Overview
| Block | Management |
|---|---|
| 1st degree | Usually no treatment; monitor; address reversible causes |
| 2nd degree Mobitz I | Often no treatment if asymptomatic; atropine if symptomatic; pacing rarely needed |
| 2nd degree Mobitz II | Permanent pacemaker in most cases; transcutaneous pacing if unstable |
| 3rd degree (complete) | Immediate pacing if symptomatic; atropine for nodal blocks; transcutaneous pacing while arranging transvenous; permanent pacemaker eventually |
Key clinical point: Infranodal blocks (Mobitz II, complete block with wide QRS escape) are unlikely to respond to atropine or vagolytic agents. Pacing is the definitive treatment. - Tintinalli's Emergency Medicine
Quick ECG Recognition Trick
| What you see | Likely block |
|---|---|
| Every P has a QRS, PR > 200 ms | 1st degree |
| PR getting longer → dropped beat → reset | 2nd degree Mobitz I (Wenckebach) |
| Constant PR → sudden dropped beat, wide QRS | 2nd degree Mobitz II |
| P waves and QRS completely unrelated, regular slow escape | 3rd degree (complete) |
This is a shared conversation. Sign in to Orris to start your own chat.