Collapse of lung lobes and thier findings in x ray and ct With images and explaination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content and images needed. Here is the comprehensive, fully-illustrated answer.
Lobar Collapse of the Lung - Radiological Findings on CXR and CT
Source: Grainger & Allison's Diagnostic Radiology
Introduction
Collapse (atelectasis) refers to loss of volume within the lung. The terms are often used interchangeably. "Lobar collapse" specifically means complete loss of volume within an entire lobe.
Cardinal radiographic features of any lobar collapse:
- Increased opacity of the affected lobe (due to retained fluid + loss of aeration)
- Volume loss - demonstrated by direct and indirect signs
| Sign Type | Examples |
|---|---|
| Direct | Displaced interlobar fissures, displaced vessels/bronchi |
| Indirect (compensatory) | Hyperinflation of adjacent lobes, mediastinal shift, diaphragm elevation, hilar displacement, rib crowding |
Absence of air bronchograms within the collapsed lobe suggests a central obstructing lesion (tumor vs. pneumonia).
Mechanisms and Causes
| Category | Examples |
|---|---|
| Intrinsic endobronchial obstruction | Bronchogenic carcinoma (most common in smokers), mucus plugs, foreign body, carcinoid, metastases, granulomas (TB, sarcoid) |
| Extrinsic compression | Hilar/mediastinal lymphadenopathy, mediastinal masses, aortic aneurysm |
| Without obstruction | Passive collapse (pleural effusion, pneumothorax), post-radiation, rounded atelectasis |
In a middle-aged or elderly smoker, lobar collapse should always raise suspicion of bronchogenic carcinoma until proven otherwise.
Golden's S Sign (important for any lobe)
When a central mass causes collapse, the fissure forms an S-shape - convex centrally (due to the mass) and concave peripherally (due to the collapse). Originally described in the RUL but can occur in any lobe.
1. Right Upper Lobe (RUL) Collapse
CXR Findings:
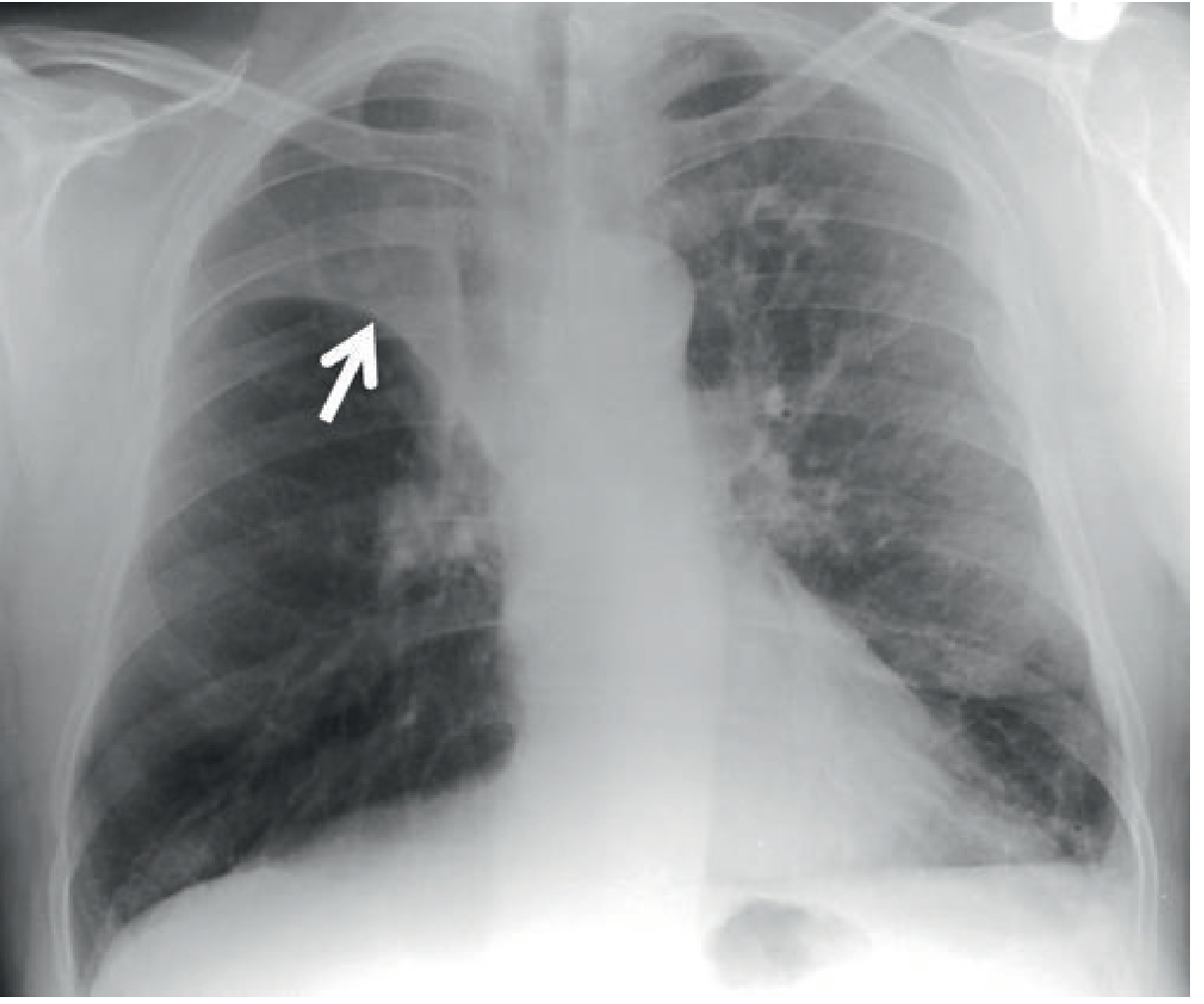
- PA view: Increased density at the right apex adjacent to the mediastinum; the horizontal fissure is elevated and has a concave inferior border (Fig. 7.17 below)
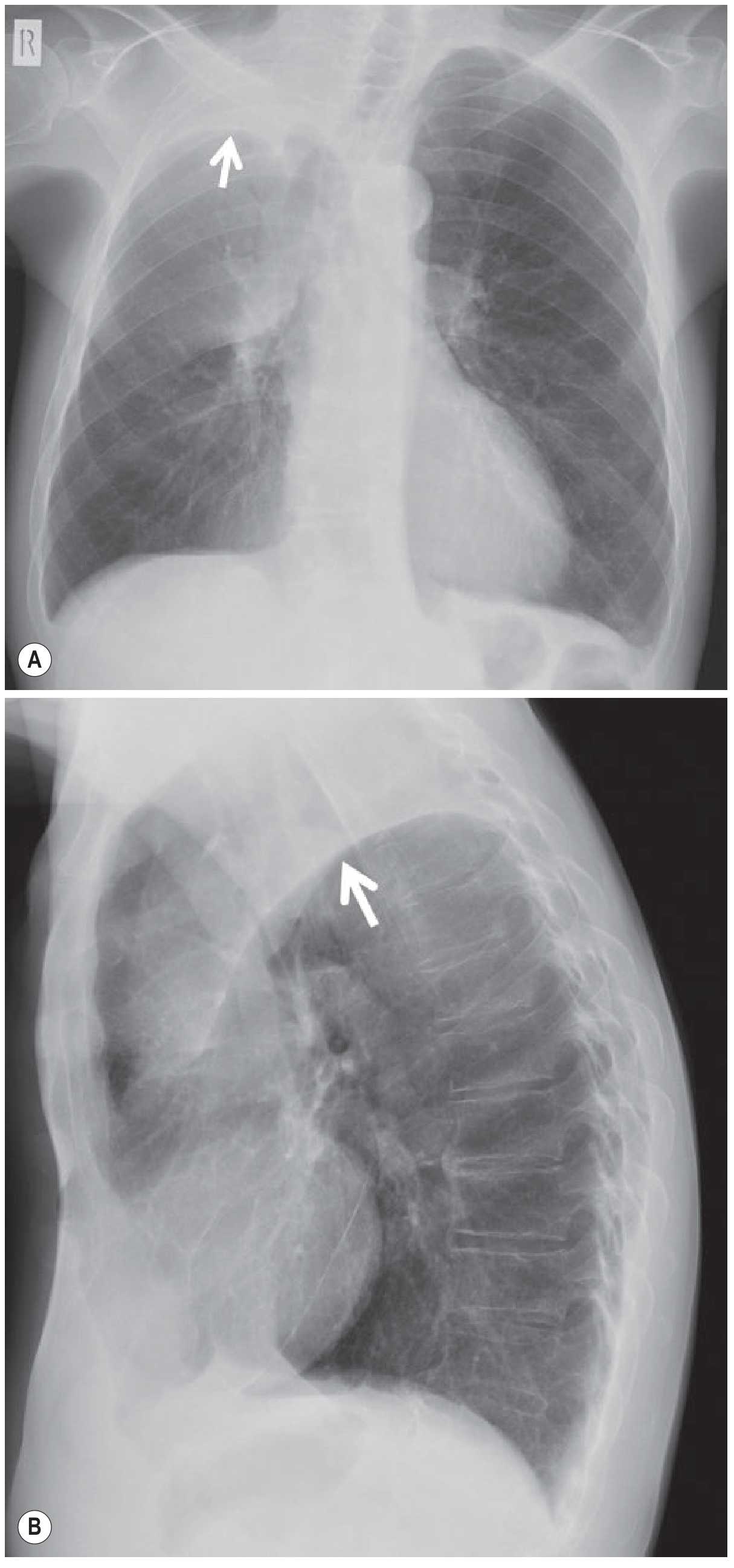
- In tight collapse: the lobe parallels the mediastinum, mimicking an apical pleural cap or mediastinal widening (Fig. 7.18/7.19)
- There is often a small convexity at the hilum where the apex attaches
- Compensatory hyperinflation of RML and RLL - right main bronchus/lower lobe artery course becomes more horizontal
- Lateral view: Both horizontal and oblique fissures displaced superiorly and medially - ill-defined wedge-shaped superior density
CT Findings:
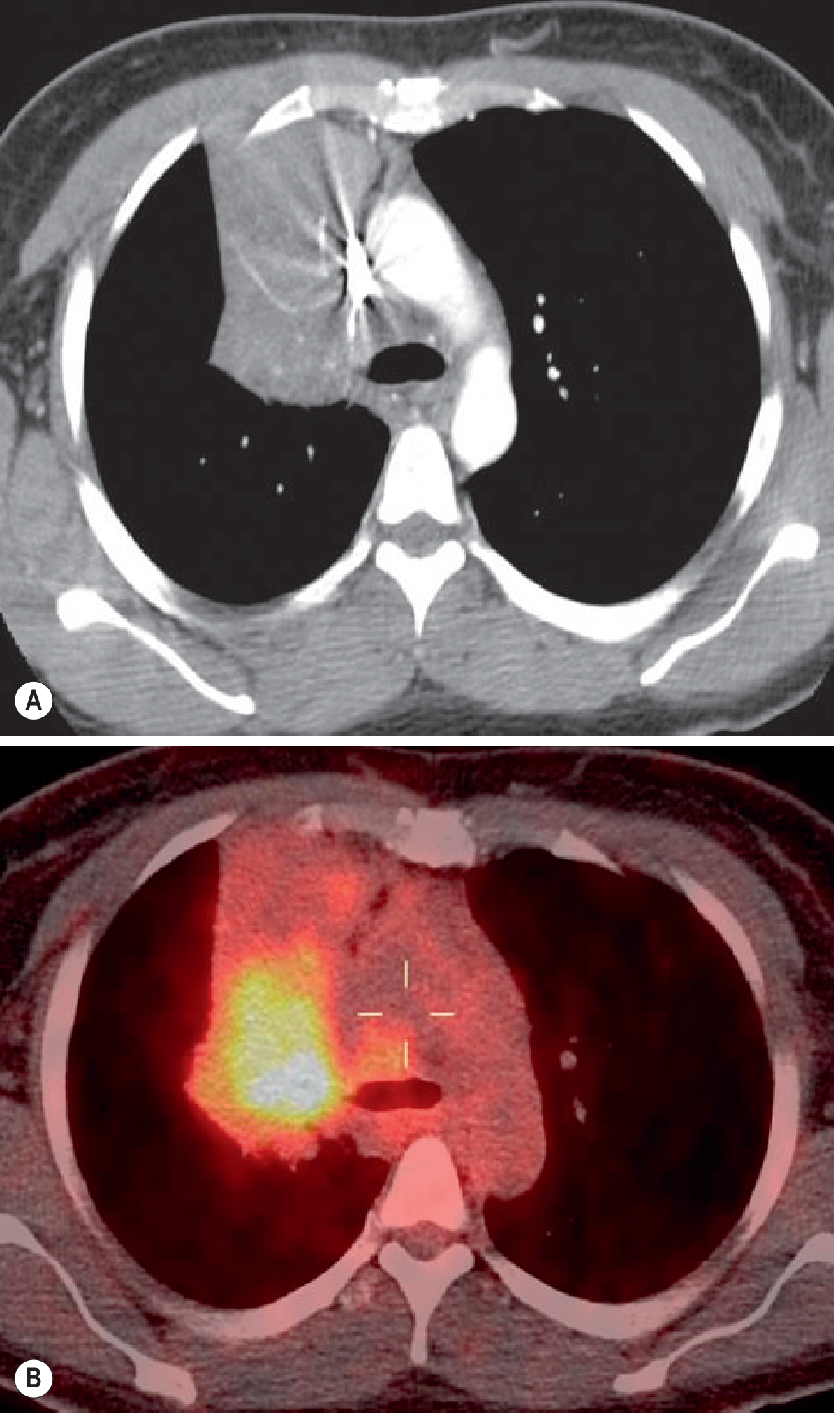
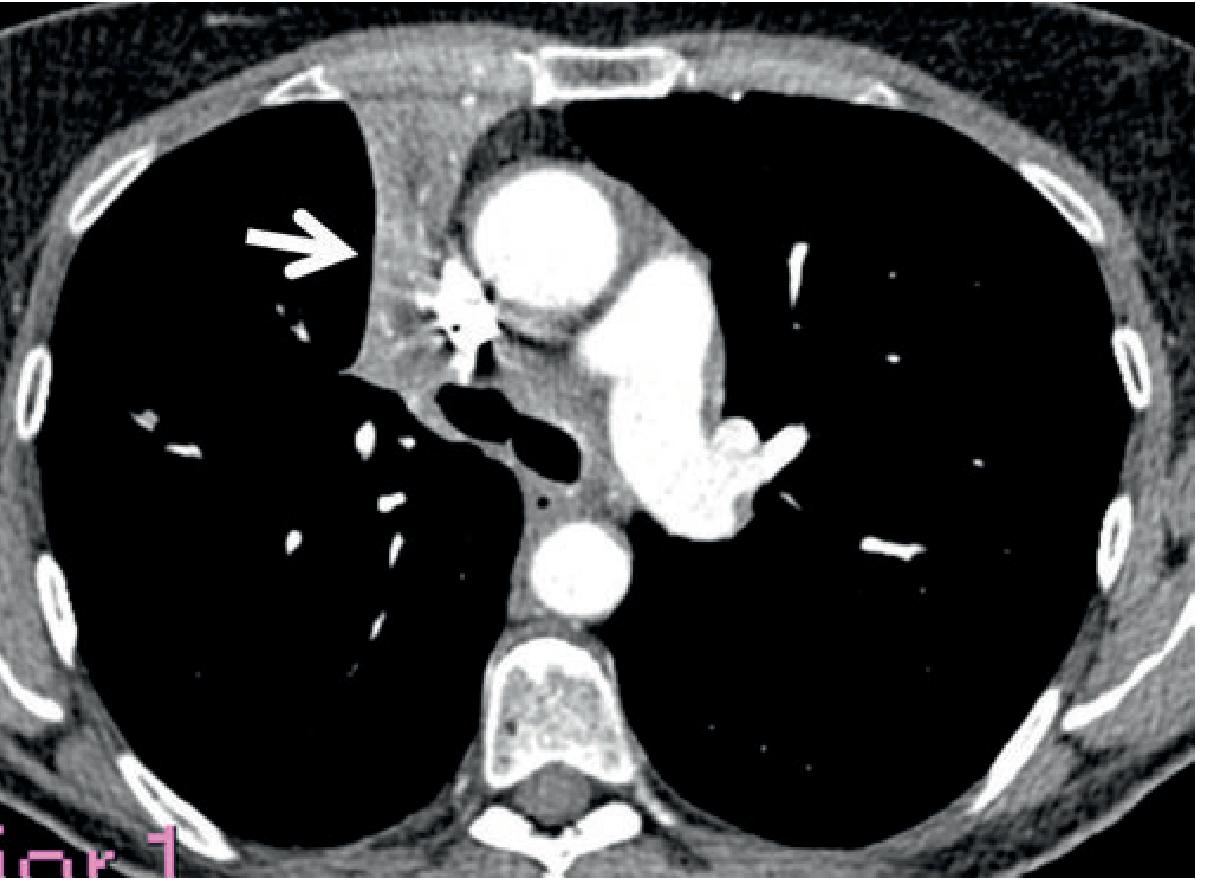
- Roughly triangular density with the base anteriorly against the chest wall and apex at the hilum
- A focal bulge of the lateral border indicates an underlying mass
- Compensatory hyperinflation well-appreciated, including left upper lobe overexpansion crossing the midline
Typical RUL collapse - CXR (note concave inferior border of elevated horizontal fissure, arrow):
RUL collapse mimicking apical cap on frontal (A) and lateral (B) showing superior fissure displacement:
CT of tight RUL collapse - triangular wedge anteriorly (arrow), with PET-CT fused image:
CT axial showing RUL collapse (arrow) - triangular soft-tissue density adjacent to right mediastinum:
2. Left Upper Lobe (LUL) Collapse
The LUL behaves differently from the RUL because the left lung rarely has a horizontal fissure.
CXR Findings:
- Volume loss is predominantly anterior and medial (not superior like the right)
- PA view: "Veil-like" hazy increased density over the entire left hemithorax - greatest at the hilum, fading out laterally/superiorly/inferiorly without a sharp inferior border
- Loss of silhouette of left heart border, aortic arch, and left mediastinum
- In less severe collapse: left heart border and aortic knuckle are obscured
- In severe collapse: the aortic knuckle may paradoxically become visible again - the apical segment of the LLL hyperexpands superiorly and outlines the arch
- Luftsichel sign: "air crescent" of hyperexpanded lung between the aortic arch and the medial collapse border
- Left main bronchus reoriented with more horizontal course; angulation with LLL bronchus
- Lateral view: Entire oblique fissure displaced anteriorly and medially, parallel to the chest wall
CT Findings:
- Triangular soft-tissue density with apex at origin of upper lobe bronchus and base against the anterior chest wall adjacent to the left mediastinal border
- Lingular segment seen as density closely opposed to the left heart border
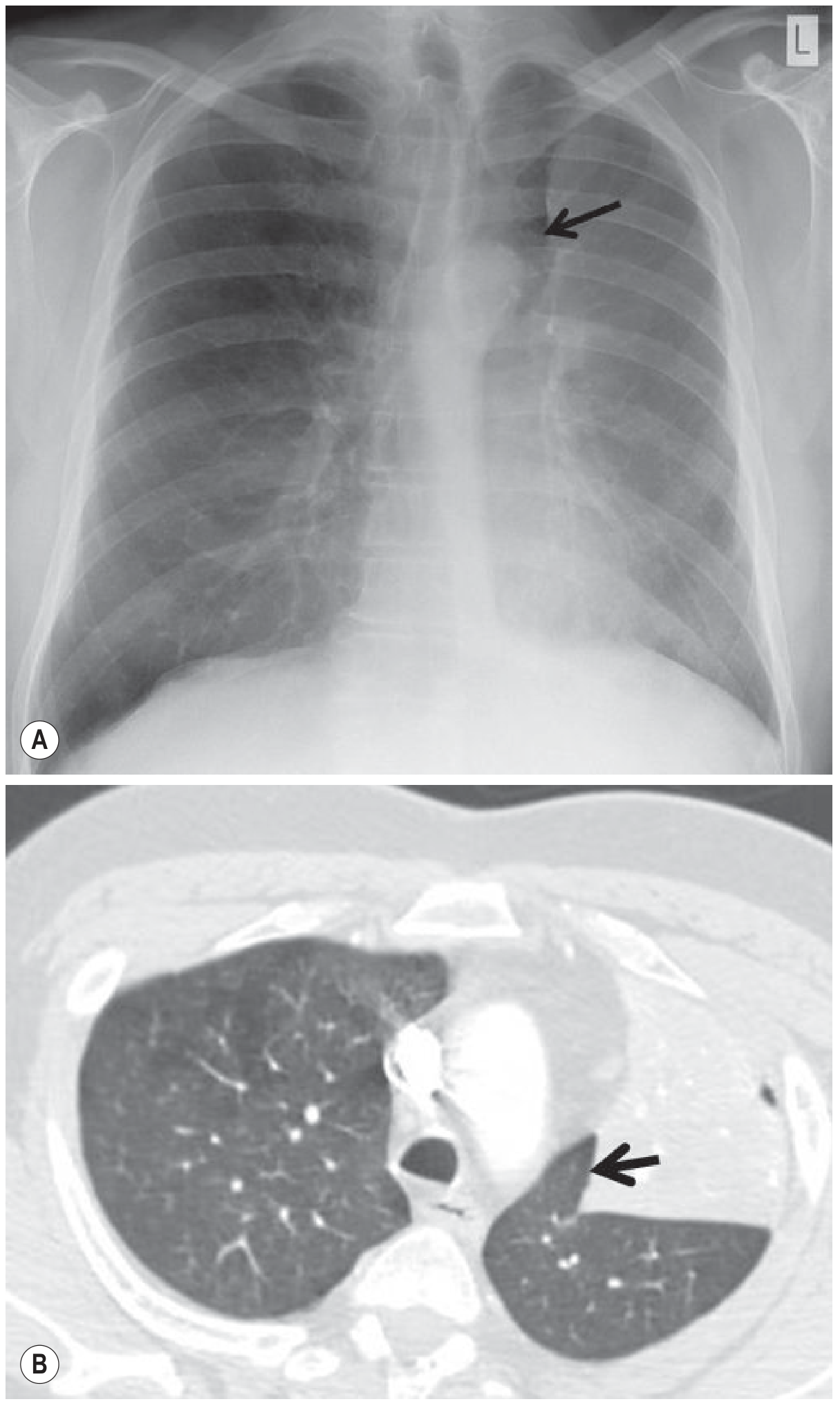
Luftsichel sign - air crescent (arrow) between aortic arch and collapsed LUL on CXR; CT showing interposition of aerated lung:
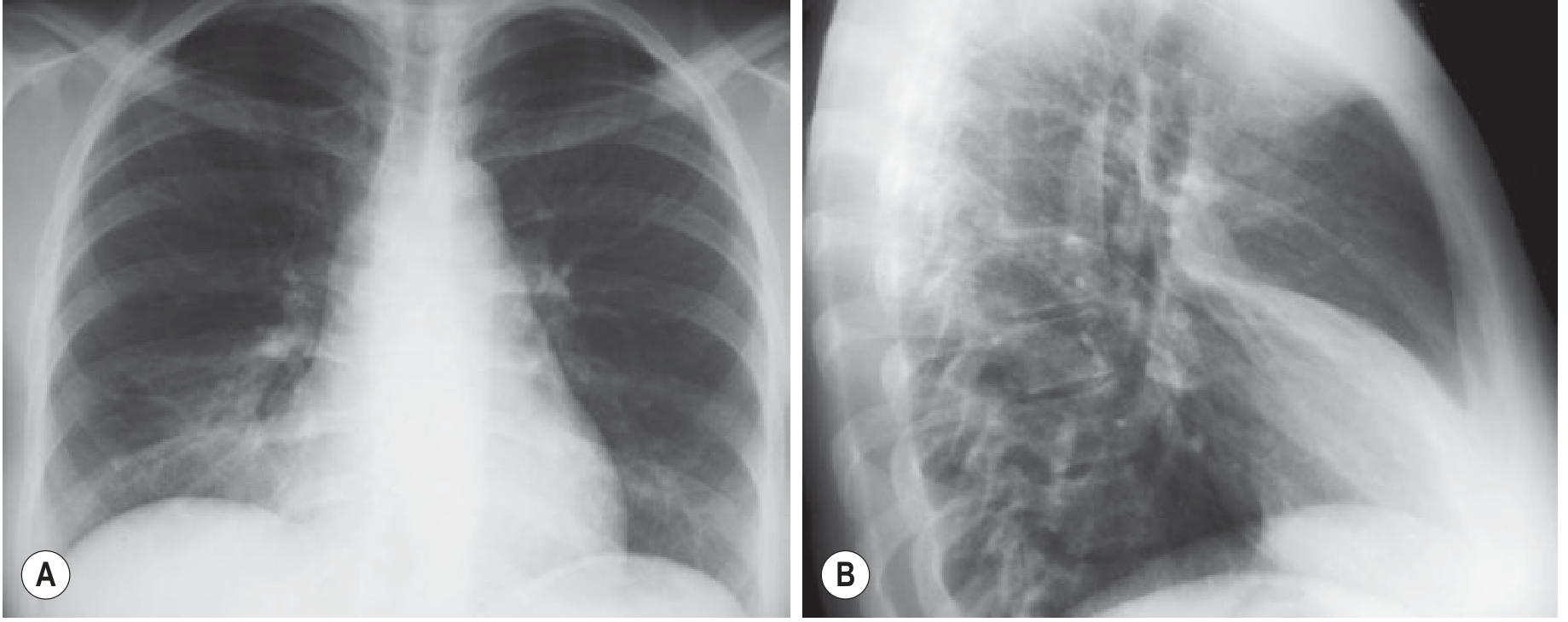
LUL collapse - PA and lateral views (veil-like opacity, anteriorly displaced oblique fissure on lateral):
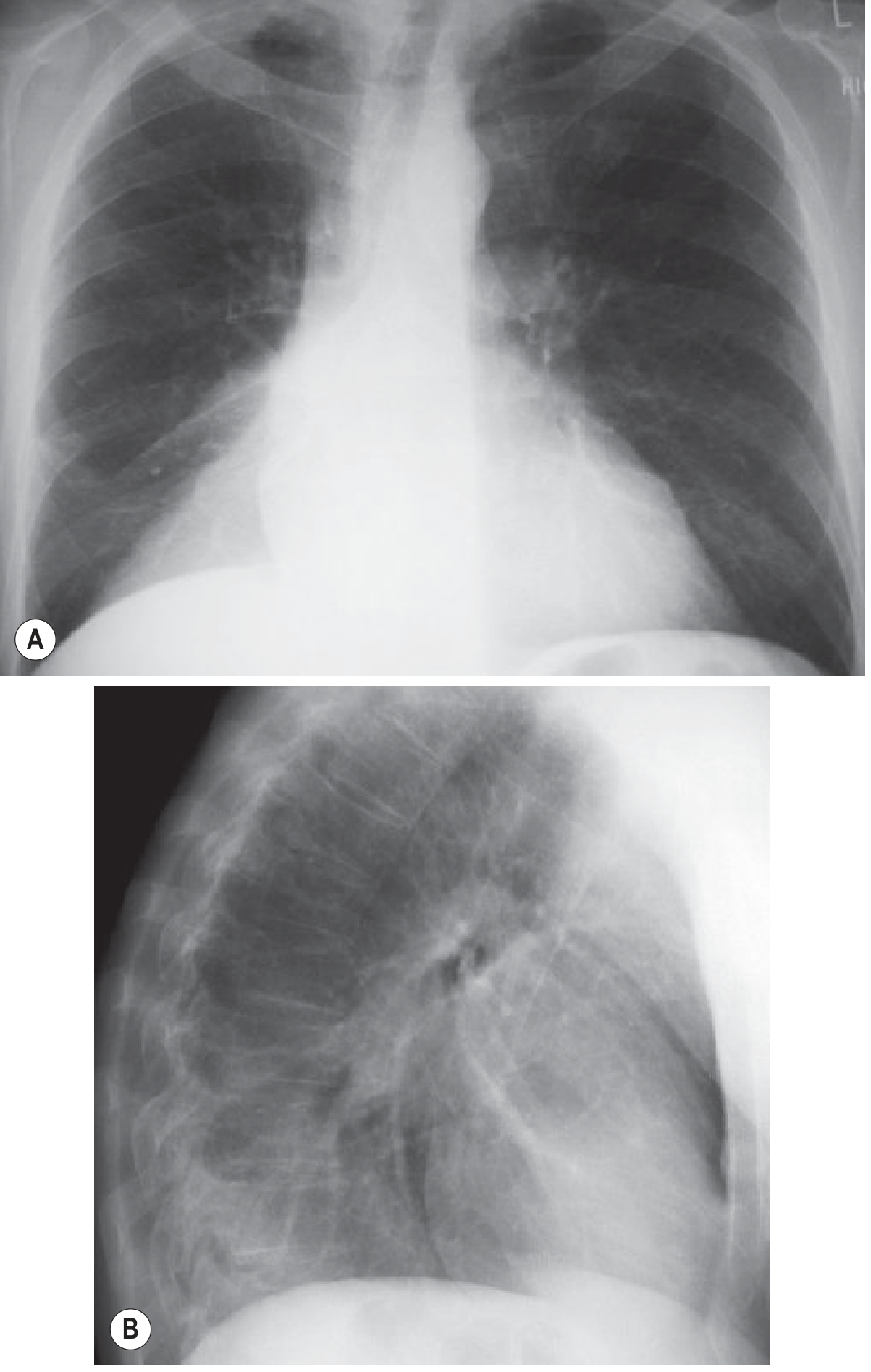
LUL collapse - veil-like opacity with loss of left heart border and aortic arch silhouette:
3. Right Middle Lobe (RML) Collapse
Signs on the frontal CXR can be extremely subtle and easy to miss.
CXR Findings:
- PA view:
- Loss of silhouette of the right heart border (variable degree) - the key sign
- If collapse is oriented parallel to the beam or patient is lordotic: triangular/sail-shaped density adjacent to the right heart border (Fig. 7.24, 7.26)
- If collapse lies obliquely, the only sign may be subtle loss of the right heart border silhouette
- Lateral view: Wedge-shaped density extending anteriorly from the hilum toward the sternum - this is the most reliable view (Fig. 7.24)
CT Findings:
- Narrow wedge of soft tissue anteriorly adjacent to the heart - best seen on coronal reformats
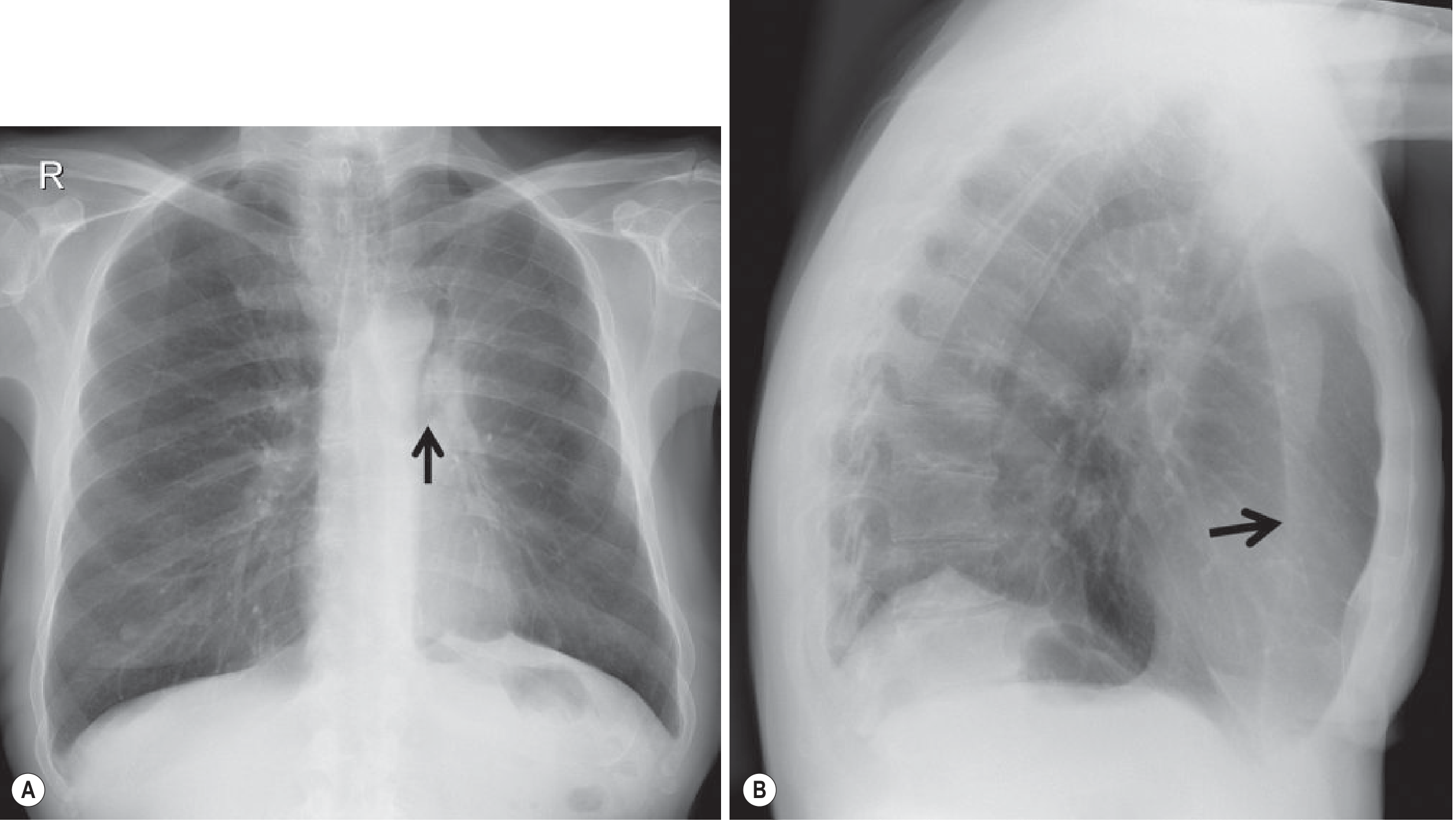
RML collapse - PA (loss of right heart border, arrow) and lateral (wedge-shaped anterior density from hilum, arrow):
"Middle lobe syndrome" refers to chronic RML collapse with bronchiectasis due to focal bronchostenosis (classically from tuberculosis).
4. Right and Left Lower Lobe (RLL/LLL) Collapse
The features are similar for both sides.
CXR Findings:
- PA view: Triangular density behind the heart - "sail sign" or "triangular shadow behind the cardiac silhouette" (Fig. 7.27)
- Loss of clarity of the medial hemidiaphragm (no longer outlined by aerated lung)
- If inferior pulmonary ligament is incomplete, the medial diaphragm contour may still be visible
- Lateral view:
- Posterior hemidiaphragm contour not visualized
- Spine sign: Vertebral column appears progressively denser inferiorly - this is the opposite of the normal pattern and is a reliable sign of lower lobe collapse
CT Findings:
- The collapsed lobe lies in the posteromedial portion of the chest
- Oblique fissure displaced posteriorly and medially
- Compensatory hyperinflation of the upper lobes well demonstrated
Summary Table
| Lobe | PA CXR Key Finding | Lateral Key Finding | CT Key Finding |
|---|---|---|---|
| RUL | Apical opacity, elevated horizontal fissure with concave inferior border | Both fissures displaced superiorly | Triangular anterior wedge, apex at hilum |
| LUL | Veil-like opacity entire hemithorax, loss of left heart/aortic silhouette, Luftsichel sign | Oblique fissure displaced anteriorly (parallel to chest wall) | Anterior triangular density adjacent to left mediastinum |
| RML | Loss of right heart border silhouette (subtle), sail-shaped density | Anterior wedge from hilum to sternum | Narrow anterior wedge adjacent to heart |
| RLL/LLL | Triangular density behind heart, loss of medial hemidiaphragm | Spine sign (denser inferiorly), posterior diaphragm not seen | Posteromedial opacity, posteriorly displaced oblique fissure |
CT - Special Advantages Over CXR
- Eliminates superimposition of overlying structures
- Multiplanar reconstructions (coronal, sagittal) clarify fissure displacement
- Identifies the cause of collapse (endobronchial mass, mucus plug, lymphadenopathy)
- Detects distal air bronchograms (often visible in neoplastic collapse on CT, unlike CXR prediction)
- Better characterization of compensatory changes
All images and content sourced from Grainger & Allison's Diagnostic Radiology, Chapter 7 (Lobar Collapse).
This is a shared conversation. Sign in to Orris to start your own chat.