Im posted as duty doctor in gastroenterology dpt multi speciality hospital. So teach me about pancreatitis and its management in casuality or hospital level along with specific treatments
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute pancreatitis" AND management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the complete clinical teaching guide.
Pancreatitis: A Complete Clinical Guide for the Duty Doctor in Gastroenterology
Sources: Schwartz's Principles of Surgery (11e), Rosen's Emergency Medicine, Sabiston Textbook of Surgery, Current Surgical Therapy (14e), Goldman-Cecil Medicine, Maingot's Abdominal Operations, ACG 2024 Guidelines [PMID: 38857482], IAP/APA Revised Guidelines 2025 [PMID: 40651900]
1. PATHOPHYSIOLOGY - KNOW YOUR ENEMY
The key event in acute pancreatitis (AP) is inappropriate intracellular activation of trypsinogen to trypsin within acinar cells.
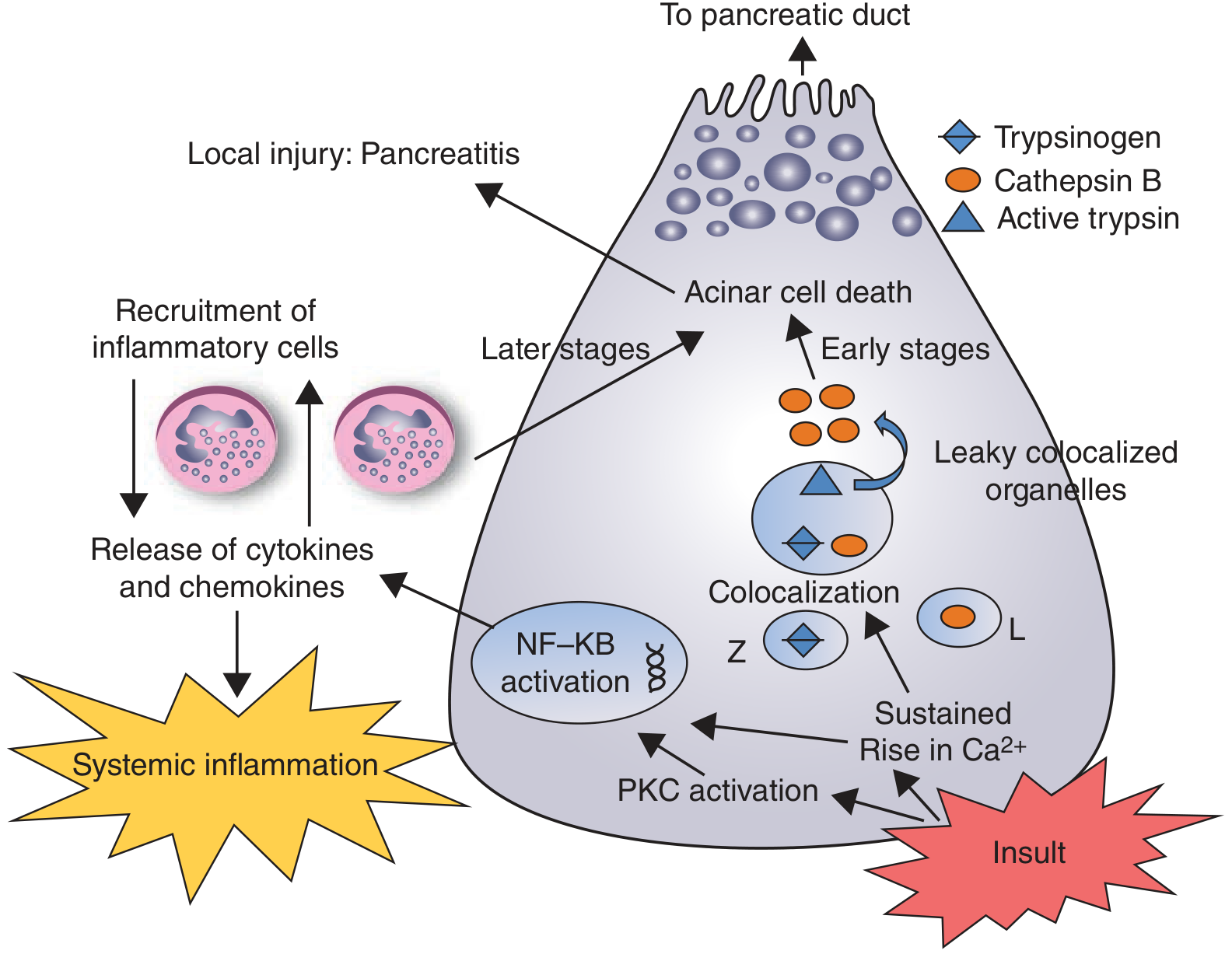
The cascade:
- Inciting event (gallstone obstruction, alcohol, drugs, etc.) causes cellular injury
- Lysosomal (cathepsin B) and zymogen (trypsinogen) contents colocalize within the acinar cell
- Trypsinogen is activated to trypsin - which then activates all other digestive enzymes (autodigestion)
- Sustained rise in cytosolic Ca²+ activates NF-kB - triggering cytokine/chemokine release
- Macrophage and neutrophil recruitment magnifies local damage
- SIRS, organ failure, sepsis, and shock follow in severe cases
- Bacteremia via translocation of gut organisms completes the picture in infected necrosis
- Schwartz's Principles of Surgery, 11e
2. ETIOLOGY (I GET SMASHED - Classic Mnemonic)
| Cause | Notes |
|---|---|
| I - Idiopathic | ~15-25% of cases |
| G - Gallstones | Most common cause overall (40-70%) |
| E - Ethanol (Alcohol) | 2nd most common (30%) |
| T - Trauma | Blunt abdominal trauma |
| S - Steroids | Corticosteroids, azathioprine |
| M - Mumps / other viruses | Coxsackievirus, CMV |
| A - Autoimmune | IgG4-related disease |
| S - Scorpion sting | Tityus trinitatis |
| H - Hyperlipidemia / Hypercalcemia | TG > 1000 mg/dL is classic |
| E - ERCP | Post-ERCP pancreatitis |
| D - Drugs | Thiazides, furosemide, valproate, didanosine, metronidazole |
3. DIAGNOSIS IN CASUALTY
Diagnostic Criteria (2 of 3 required)
- Characteristic abdominal pain - severe, steady, epigastric/periumbilical, radiates to the back, worse supine, better leaning forward
- Serum lipase or amylase > 3x upper limit of normal - lipase is preferred (more sensitive and specific; stays elevated longer)
- Characteristic findings on cross-sectional imaging (CT/MRI)
Amylase >3x ULN is threshold - levels may be normal in alcoholic pancreatitis or hypertriglyceridemia. Always order lipase.
Investigations to Order at Casualty Triage
Immediate (first hour):
- Serum lipase (preferred) + amylase
- CBC, CRP (baseline - CRP >150 mg/dL at 48h predicts severe disease)
- BMP: BUN, creatinine, electrolytes, glucose, calcium
- LFTs (ALT >3x ULN = biliary etiology with ~95% PPV)
- Serum triglycerides
- ABG if any respiratory distress
Imaging:
- Abdominal ultrasound - mandatory in ALL patients to look for gallstones/biliary dilation (sensitivity 95% for gallstones). Pancreas itself is often not well visualized due to bowel gas.
- CT scan (contrast-enhanced, portal venous phase) - NOT routine at presentation. Indications:
- Diagnostic uncertainty
- Failure to improve after 48-72h conservative management
- Clinical deterioration / suspected complications
- CTSI scoring for severity
4. SEVERITY ASSESSMENT
2012 Revised Atlanta Classification
| Grade | Definition |
|---|---|
| Mild | No organ failure, no local/systemic complications. Mortality <1% |
| Moderately Severe | Transient organ failure (<48h) OR local/systemic complications |
| Severe | Persistent organ failure (>48h) - cardiovascular, respiratory, or renal. Mortality 20-40% |
| Critical | Persistent organ failure + infected necrosis. Mortality >50% |
Organ failure = modified Marshall score ≥2 for respiratory (PaO2/FiO2), cardiovascular (MAP), or renal (creatinine) systems.
Ranson's Criteria (11 parameters)
At Admission:
| Parameter | Biliary | Alcoholic |
|---|---|---|
| Age | >70 years | >55 years |
| WBC | >18,000 | >16,000 |
| Blood glucose | >220 mg/dL | >200 mg/dL |
| LDH | >400 IU/L | >350 IU/L |
| AST | >250 IU/L | >250 IU/L |
At 48 hours:
| Parameter | Both |
|---|---|
| Hematocrit fall | >10% |
| BUN rise | >2 mg/dL |
| Calcium | <8 mg/dL |
| PaO2 | <60 mmHg |
| Base deficit | >5 mEq/L |
| Fluid sequestration | >6 L |
Score interpretation: ≥3 = severe pancreatitis. Sensitivity ~70%, specificity ~80%. Mainly useful to rule OUT severity (NPV 90%). Cannot be fully calculated until 48h.
BISAP Score (Bedside Index for Severity in Acute Pancreatitis)
Score 1 point each: BUN >25 mg/dL | Impaired mental status | SIRS criteria ≥2 | Age >60 | Pleural effusion
Score ≥3 = high risk for organ failure and death. Calculable at admission - more ED-friendly.
SIRS Criteria (Recommended for Real-Time Monitoring)
Currently recommended at presentation AND 48h post-admission. Persistent SIRS is the strongest predictor of severe disease.
- Temperature <36°C or >38°C
- HR >90 bpm
- RR >20 or PaCO2 <32 mmHg
- WBC <4000 or >12,000 or >10% bands
5. EMERGENCY MANAGEMENT - THE FIRST 24 HOURS
5A. Fluid Resuscitation (The Most Critical Intervention)
"The most important treatment intervention for acute pancreatitis is early, intravenous fluid resuscitation to prevent systemic complications." - Harrison's Principles of Internal Medicine (22e)
Choice of fluid:
- Lactated Ringer's (LR) is the preferred fluid over normal saline. LR is more physiologic and has demonstrated anti-inflammatory properties (prevents acidosis, reduces SIRS). Supported by RCT evidence.
- Avoid normal saline as primary resuscitation fluid (hyperchloremic acidosis risk).
Rate:
- Goal-directed: 250-500 mL/hour initially in first few hours
- Monitor response with: urine output (goal >0.5-1 mL/kg/hour), HR normalization, BUN trend
- Avoid over-resuscitation - can worsen abdominal compartment syndrome, respiratory failure. Proponents of aggressive therapy (5-10 mL/kg/hr) must be balanced against these risks.
- Reassess every 4-6 hours and taper rate as patient improves.
Monitoring response:
- Hourly urine output
- BUN (rising BUN = inadequate resuscitation)
- Hematocrit (should decrease with adequate fluids if hemoconcentrated)
5B. Pain Management
Pain is the cardinal symptom - adequate analgesia is mandatory.
- Route: IV, at least initially, due to unpredictable absorption and vomiting
- Agents: No single agent is definitively superior. Options:
- NSAIDs (ketorolac 30 mg IV) - good first-line, anti-inflammatory effect
- Opioids when NSAIDs insufficient - hydromorphone or fentanyl preferred. No evidence that morphine is harmful despite theoretical concern about sphincter of Oddi spasm.
- Patient-controlled analgesia (PCA) - appropriate for severe/prolonged cases
- Opioids may promote ileus - use at lowest effective dose.
5C. NPO and Nasogastric Tube
- Make patient NPO initially to minimize exocrine stimulation
- NGT only if patient has intractable vomiting or ileus causing distension - not routine
5D. Antiemetics
- Metoclopramide, ondansetron, or promethazine for nausea/vomiting
5E. Monitoring Setup
- IV access x2, continuous pulse oximetry, cardiac monitoring if hemodynamically unstable
- Strict input-output chart
- Blood glucose monitoring every 4-6h (risk of hyperglycemia)
- Serial abdominal exams
6. HOSPITAL MANAGEMENT
6A. Ward vs. ICU Decision
Admit to ICU/HDU if any of the following:
- Persistent organ failure (Severe Atlanta)
- BISAP ≥3 or Ranson ≥3
- SIRS criteria met at presentation or 48h
- Hemodynamic instability requiring vasopressors
- Respiratory failure (SpO2 <95% on room air)
- Necrotizing pancreatitis on CT
6B. Nutrition - Critical and Often Mismanaged
The old paradigm of "resting the pancreas" with prolonged NPO and TPN is obsolete.
Current evidence-based approach:
| Severity | Approach |
|---|---|
| Mild AP | Allow oral intake ad libitum when tolerated (no need to wait for amylase normalization). Soft/low-fat diet as tolerated. |
| Moderate-Severe AP | If oral intake not tolerated in 24-48h, start nasogastric or nasojejunal feeding |
| Severe AP | Early enteral nutrition (within 24-72h) via nasoenteric tube - nasogastric is as effective as nasojejunal in most patients |
| Parenteral nutrition (TPN) | Only if enteral route is absolutely not achievable - higher cost, higher infection risk, no superior outcomes |
- Standard polymeric formulas are adequate - no evidence for elemental or immune-enhancing formulas over standard
- Enteral nutrition maintains gut barrier integrity, reduces bacterial translocation, and attenuates inflammatory response
6C. Antibiotics
Prophylactic antibiotics: NOT recommended
Multiple high-quality RCTs have shown no benefit from prophylactic antibiotics in acute pancreatitis, even in necrotizing disease. Prophylaxis leads to selection of resistant organisms and fungal infections.
When TO use antibiotics:
- Documented infected pancreatic necrosis (positive culture from CT-guided FNA or interventional drain, or gas in necrosis on CT)
- Ascending cholangitis (Charcot's triad: fever + jaundice + RUQ pain)
- Other confirmed extra-pancreatic infections (UTI, pneumonia, bacteremia)
Antibiotic choice for infected necrosis:
- Carbapenems (meropenem, imipenem) - good pancreatic penetration, covers gram-negative enteric organisms which are most common (E. coli, Klebsiella, Enterococcus)
- Alternatives: ciprofloxacin + metronidazole, or piperacillin-tazobactam
6D. Special Considerations by Etiology
Gallstone pancreatitis:
- All patients should have cholecystectomy before discharge (or within 2-4 weeks of mild AP) to prevent recurrence (~50% recurrence without it)
- Do NOT perform cholecystectomy during acute attack
ERCP indications in AP:
- Emergency ERCP (within 24h): Acute cholangitis concurrent with AP
- Urgent ERCP (within 48-72h): Persistent biliary obstruction without cholangitis (jaundice, rising bilirubin)
- NOT indicated in uncomplicated gallstone pancreatitis - the offending stone usually passes spontaneously
Hypertriglyceridemia-induced AP (TG >1000 mg/dL):
- Insulin infusion (lowers TG rapidly)
- Heparin (activates lipoprotein lipase)
- Plasmapheresis in refractory severe cases
- Long-term: fibrate therapy, dietary restriction
7. COMPLICATIONS AND THEIR MANAGEMENT
Local Complications (Atlanta 2012 Classification)
| Timing | No Infection | Infected |
|---|---|---|
| Acute (<4 wks, no defined wall) | Acute Pancreatic Fluid Collection (APFC) | Infected APFC |
| Acute with necrosis | Acute Necrotic Collection (ANC) | Infected ANC |
| Chronic (>4 wks, defined wall) | Pseudocyst | Infected Pseudocyst |
| Chronic with necrosis | Walled-Off Necrosis (WON) | Infected WON |
Management of Necrotizing Pancreatitis
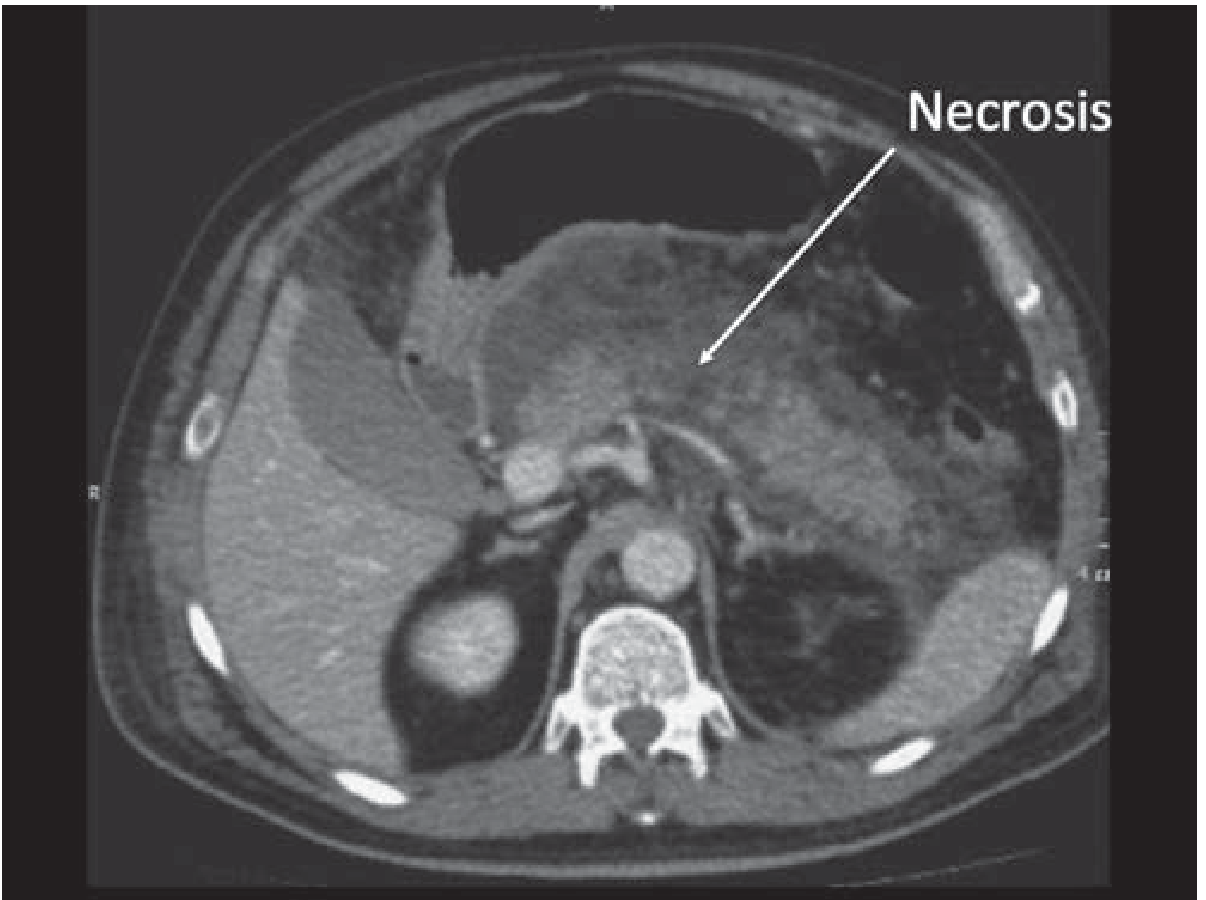
- Sterile necrosis: Managed conservatively - no intervention, no prophylactic antibiotics. The majority resolve.
- Infected necrosis: Diagnosed by CT showing gas in necrosis, or positive culture from drain/FNA. Requires drainage + antibiotics.
Step-up approach for infected necrosis (current standard):
- Antibiotics (carbapenems)
- Delay intervention to allow walling-off (ideally ≥4 weeks from onset)
- Percutaneous catheter drainage (PCD) as first-line - resolves ~1/3 to half of cases without further intervention
- Minimally invasive drainage if PCD fails:
- Video-assisted retroperitoneal debridement (VARD)
- Endoscopic ultrasound-guided transmural drainage/necrosectomy
- Open surgical necrosectomy - last resort, highest morbidity. Reserved for failure of all minimally invasive approaches.
Pseudocyst
- Fluid collection >4 weeks with defined wall, no necrosis
- Asymptomatic pseudocysts - observe, most resolve spontaneously
- Symptomatic (pain, early satiety, obstruction, infection) - endoscopic transmural drainage preferred (EUS-guided cystogastrostomy), or percutaneous drainage
Systemic Complications
| Complication | Management |
|---|---|
| ARDS / Respiratory failure | Supplemental O2, HFNC, intubation + mechanical ventilation if needed |
| AKI / Renal failure | Aggressive fluid resuscitation, avoid nephrotoxins, dialysis if needed |
| Hypocalcemia | IV calcium gluconate (symptomatic) or oral supplementation |
| Hyperglycemia | Insulin sliding scale; may indicate pancreatic endocrine damage |
| Abdominal compartment syndrome | Risk with massive fluid resuscitation; monitor bladder pressure; decompress if IAP >20 mmHg with organ dysfunction |
| GI hemorrhage | From pseudoaneurysm rupture - angioembolization first-line |
| Septic shock | ICU admission, vasopressors (norepinephrine), broad-spectrum antibiotics, source control |
8. CHRONIC PANCREATITIS - KEY POINTS FOR WARD CALLS
- Pain is chronic, progressive, postprandial, epigastric radiating to back
- Serum amylase/lipase may be normal in established chronic pancreatitis (burnt-out exocrine function)
- Look for: steatorrhea, weight loss, diabetes mellitus ("pancreatic diabetes")
- CT findings: pancreatic calcifications, ductal dilation, parenchymal atrophy
- Exocrine insufficiency: Treat with pancreatic enzyme replacement therapy (PERT) - lipase ≥40,000-50,000 IU per meal, with acid suppression (PPI)
- Pain management: Stepwise - paracetamol > NSAIDs > tramadol > opioids; adjuncts include pregabalin, celiac plexus block
- Endoscopic/surgical: ERCP for ductal stones/strictures; Puestow procedure (lateral pancreaticojejunostomy) for dilated duct with pain
9. QUICK REFERENCE - CASUALTY CHECKLIST
ACUTE PANCREATITIS - CASUALTY PROTOCOL
□ IV access x2 + bloods: lipase, amylase, CBC, CMP, LFTs, CRP, triglycerides, ABG
□ Abdominal USS (all patients - gallstones)
□ Start IV Lactated Ringer's 250-500 mL/hr, titrate to UO >0.5 mL/kg/hr
□ NPO + antiemetics
□ IV analgesia (ketorolac ± opioid)
□ Urinary catheter for strict I/O monitoring
□ Calculate BISAP score
□ If BISAP ≥3 or SIRS: Consider ICU/HDU transfer
□ CT with contrast ONLY IF: diagnostic uncertainty, clinical deterioration at 48-72h
□ NO prophylactic antibiotics
□ Reassess at 48h: SIRS status, BUN trend, fluid balance, organ function
□ Nutrition: Start oral/NG feeds as soon as tolerated; do NOT wait for amylase normalisation
□ If gallstone etiology: plan cholecystectomy before discharge
□ If cholangitis: URGENT ERCP within 24h
10. CURRENT GUIDELINES - 2024/2025 UPDATES
The ACG 2024 Clinical Practice Guidelines for Management of Acute Pancreatitis (PMID: 38857482) and IAP/APA Revised Guidelines 2025 (PMID: 40651900) confirm:
- LR preferred over NS for fluid resuscitation
- Enteral > parenteral nutrition - start early
- No prophylactic antibiotics in AP or necrotizing pancreatitis
- Step-up approach for infected necrosis with delayed (≥4 weeks) intervention
- Cholecystectomy during index admission or within 2-4 weeks for biliary pancreatitis
- ERCP only for cholangitis or persistent biliary obstruction
Key mortality numbers to keep in mind:
- Mild AP (interstitial edematous): <1% mortality
- Moderate AP: ~3-8%
- Severe AP (organ failure >48h): 20-40%
- Infected necrotizing pancreatitis: up to 30-50%
Early aggressive fluid resuscitation with LR, early enteral nutrition, judicious use of CT and ERCP, and prompt recognition of the step-up to ICU care are the pillars of good pancreatitis management. The pancreas does most of the healing itself - your job is to keep the patient alive and supported while it does.
This is a shared conversation. Sign in to Orris to start your own chat.