I now have comprehensive content from Cummings Otolaryngology across all the topics. Let me synthesize a thorough, well-structured answer covering all 18 topics.
Rhinology — Comprehensive Clinical Review
Based primarily on Cummings Otolaryngology Head and Neck Surgery (9780323612173) and K.J. Lee's Essential Otolaryngology (9781260122237)
1. Acute Rhinitis — Clinical Picture & Treatment
Clinic (Clinical Features)
Acute rhinitis (common cold / acute viral rhinitis) follows a predictable course:
- Prodrome (1–3 days): dryness, itching and burning of nasal mucosa, sneezing, mild malaise, low-grade fever
- Catarrhal stage (days 2–4): profuse watery rhinorrhoea, nasal obstruction (bilateral), lacrimation, post-nasal drip, hyposmia/anosmia
- Mucopurulent stage (days 5–7): secretions thicken, become mucopurulent (secondary bacterial colonisation); associated facial pressure, headache
- Resolution usually within 7–10 days
Rhinoscopy: hyperaemic, swollen inferior turbinates, watery then mucopurulent secretion in the nasal floor.
Aetiology: Rhinovirus (>50%), coronavirus, RSV, parainfluenza, adenovirus.
Treatment
| Category | Agent |
|---|
| Topical decongestants | Oxymetazoline 0.05%, xylometazoline — max 3–5 days (avoid rhinitis medicamentosa) |
| Oral decongestants | Pseudoephedrine, phenylephrine |
| Saline irrigation | Isotonic or hypertonic nasal rinses — reduces congestion, clears secretions |
| Analgesics/antipyretics | Paracetamol, NSAIDs for fever/myalgia |
| Antihistamines | 1st-generation (chlorphenamine) reduce rhinorrhoea in viral rhinitis |
| Antibiotics | NOT indicated for uncomplicated viral rhinitis; reserved for proven bacterial superinfection |
| Antiviral | Intranasal ipratropium bromide reduces rhinorrhoea |
2. Chronic Atrophic Rhinitis — Clinic & Treatment
Definition: Progressive atrophy of the nasal mucosa, submucosa, glands, and turbinate bone, leading to paradoxical nasal obstruction despite a wide nasal cavity.
Primary (Ozaena): Caused by Klebsiella ozaenae, Staphylococcus spp., Proteus mirabilis, E. coli
Secondary: Post-surgical over-resection, granulomatous disease (TB, sarcoid, GPA), post-radiation
Clinical Features
- Foul-smelling thick crusts (ozaena) — fetid odour often noticed by others, not the patient (anosmia)
- Paradoxical nasal obstruction — wide nasal cavity yet patient feels blocked
- Anosmia / severe hyposmia
- Epistaxis from crust removal
- Persistent dryness and burning
- Rhinoscopy: atrophic, pale mucosa, greenish-yellow crusts adherent to turbinates, turbinate atrophy (especially inferior), wide nasal vault
Treatment
- Nasal irrigation with saline + glucose-glycerine solution (keeps mucosa moist)
- Topical antibiotics (mupirocin, rifampicin drops, 25% glucose in glycerine) to reduce bacterial load
- Systemic antibiotics for active Klebsiella: cotrimoxazole, ciprofloxacin
- Oestrogen drops (stilboestrol) — stimulate mucous secretion
- Surgical: Narrowing of nasal cavity by submucosal implants (Teflon, cartilage) to restore normal airflow dynamics; Young's operation (surgical closure of nostrils — rarely done today)
- Vitamin A (systemic/topical) — promotes mucosal regeneration
- Humidification of inspired air
3. Chronic Hypertrophic Rhinitis — Clinic & Treatment
Definition: Irreversible hypertrophy of the inferior (and sometimes middle) turbinates, usually resulting from chronic inflammation, repeated acute rhinitis, allergic rhinitis, or prolonged decongestant abuse.
Clinical Features
- Persistent bilateral nasal obstruction (often worse on the dependent side)
- Mouth breathing; snoring; sleep-disordered breathing
- Mucopurulent or mucoid rhinorrhoea
- Hyposmia
- Headache and facial pressure
- Rhinoscopy: enlarged, firm, mulberry-shaped inferior turbinates (do NOT shrink adequately with decongestants — distinguishes from simple congestion); surface is bosselated/irregular, pale-pink to dusky-red; probe test — firm, no pitting
Treatment
Medical (first line):
- Intranasal corticosteroids (fluticasone, mometasone) — mainstay of long-term treatment
- Saline irrigations
- Treat underlying allergy or infection
Surgical (when medical therapy fails):
| Procedure | Notes |
|---|
| Inferior turbinate reduction (submucosal diathermy / radiofrequency) | Shrinks submucosal tissue, preserves mucosa |
| Laser turbinoplasty (CO₂, KTP) | Surface ablation |
| Microdebrider-assisted turbinoplasty | Precise submucosal removal |
| Partial/total inferior turbinectomy | More aggressive; risk of atrophic rhinitis if over-resected |
| Outfracture of turbinate | Combined with submucosal resection |
4. Allergic Rhinitis — Clinic & Treatment
Pathophysiology: IgE-mediated type I hypersensitivity. Allergen → sensitisation via TH2 cytokines (IL-4, IL-5, IL-13) → specific IgE on mast cells → re-exposure → degranulation → early phase (histamine, leukotrienes, prostaglandins) + late phase (eosinophilic infiltration).
Classification (ARIA):
- Intermittent (<4 days/week or <4 weeks/year) vs. Persistent
- Mild vs. Moderate-severe
Clinical Features
- Classic tetrad: paroxysmal sneezing, watery rhinorrhoea, bilateral nasal obstruction, nasal/ocular pruritus
- Itchy, watery eyes (allergic conjunctivitis); palatal pruritus
- "Allergic salute" — upward rubbing of nose; transverse nasal crease
- Allergic shiners (periorbital venous congestion)
- Rhinoscopy: pale/bluish, oedematous turbinates; thin watery secretion; mucosa has a "wet" appearance
- Nasal smear: eosinophilia
Investigations: Skin prick test; specific serum IgE (RAST/ImmunoCAP); nasal provocation test; total IgE
Treatment
| Step | Treatment |
|---|
| Allergen avoidance | House dust mite covers, HEPA filters, avoidance of triggers |
| Intranasal corticosteroids | First-line: fluticasone, mometasone, budesonide — most effective |
| Oral antihistamines | 2nd-generation (cetirizine, loratadine, fexofenadine) — especially for sneezing/itching/rhinorrhoea |
| Intranasal antihistamines | Azelastine — rapid onset |
| Leukotriene receptor antagonists | Montelukast — especially if concomitant asthma |
| Intranasal decongestants | Short-term only |
| Allergen immunotherapy (AIT) | Subcutaneous or sublingual — disease-modifying; indicated for moderate-severe persistent AR when medications insufficient |
| Omalizumab (anti-IgE) | For severe allergic rhinitis + asthma |
| Nasal saline irrigation | Adjunct |
5. Clinical Symptoms of Deviated Nasal Septum (DNS)
The nasal septum is composed of the quadrilateral (septal) cartilage anteriorly, the perpendicular plate of the ethmoid (posterosuperiorly), and the vomer (posteroinferiorly).
Symptoms of DNS:
- Nasal obstruction — unilateral (ipsilateral to deviation) or bilateral; may alternate (worsens on the deviated side)
- Mouth breathing, snoring, sleep disturbance
- Hyposmia/anosmia (especially high septal deviations blocking olfactory cleft)
- Headaches — contact point headaches when deviated septum touches a turbinate (Sluder's neuralgia)
- Epistaxis — turbulent airflow dries mucosa over convexity of deviation, causing crusting and bleeding
- Recurrent rhinosinusitis — DNS can obstruct ostiomeatal complex drainage
- Referred otalgia (through vagal-trigeminal pathways)
- Cosmetic deformity (external nasal deviation)
Signs:
- External nasal deviation
- Anterior rhinoscopy: deviated, irregular septum; compensatory hypertrophy of the contralateral inferior turbinate
- High septal deviations, spurs, crests
6. Types, Causes & Diagnosis of Nasal Septal Deviation
Types (Mlynski classification / descriptive):
| Type | Description |
|---|
| C-shaped | Simple unilateral deviation — concavity on one side |
| S-shaped | Bilateral deviation — obstruction on both sides |
| Spur | Sharp ridge/shelf projecting laterally — may contact turbinate |
| Crest | Ridge along the floor at the junction with the maxillary crest |
| Dislocation | Caudal septum displaced off the nasal spine into one nasal vestibule |
| Combined | Multiple deformities |
Causes:
- Traumatic — most common: nasal fractures, birth trauma (forceps delivery), childhood nasal injury
- Developmental — unequal growth between septum and facial skeleton; unequal pull of septal cartilage vs. bony support
- Idiopathic — intrinsic warping of cartilage
Diagnosis:
- Anterior rhinoscopy (nasal speculum + headlight): visualise caudal and mid-septum; assess inferior turbinate size; decongest and re-examine
- Nasal endoscopy (0° and 30°): assess entire septum including posterior deviations and spurs not visible anteriorly; evaluate ostiomeatal complex
- CT scan of paranasal sinuses (coronal + axial): gold standard for surgical planning; shows degree of deviation, associated sinus disease, lamina papyracea relationships
- Acoustic rhinometry / rhinomanometry: objective airflow assessment
7. Modern Surgical Methods for Nasal Septal Deformity
Septoplasty is the gold-standard surgical correction:
Classic (Submucous Resection — Killian/Freer technique):
- Hemi-transfixion or Killian incision
- Bilateral mucoperichondrial flaps elevated
- Deviated cartilage/bone removed while preserving a 1–1.5 cm dorsal and caudal cartilage "L-strut"
- Bony deviations (vomer, perpendicular plate) removed with Takahashi forceps/osteotome
Endoscopic Septoplasty (Giles technique, 1994):
- Incision made just caudal to the deviation
- Mucoperichondrium elevated circumferentially around specific deviation/spur only
- Best for limited, localised deviations and spurs
- Advantage: can be combined with FESS in the same session
Extracorporeal Septoplasty:
- Entire septal cartilage removed, reshaped on a back table, then reimplanted
- Reserved for severely deformed cartilage; risk of saddle deformity if not meticulous
Spreader grafts / Caudal septal replacement grafts:
- For weakened or retracted caudal septum after primary surgery
- Costal cartilage or remnant septal cartilage used
Septorhinoplasty:
- Combined septoplasty + external rhinoplasty for correction of both internal and external deformity
Laser-assisted septoplasty: Limited role; CO₂ or KTP for minor irregularities
Key surgical principles (Cummings):
"Most standard procedures nowadays recognize mucosal preservation as a primary goal and make use of a submucosal approach to the cartilaginous and bony abnormalities." — Cummings Otolaryngology
8. Treatment of Acute & Chronic Rhinitis (Summary)
| Type | Medical | Surgical |
|---|
| Acute viral | Topical decongestants (≤5 days), saline, analgesics, antihistamines | Not indicated |
| Acute bacterial | Amoxicillin-clavulanate, fluoroquinolone (if complicated) | Not indicated |
| Chronic hypertrophic | INCS, antihistamines, allergen avoidance | Turbinate reduction (RF, microdebrider, partial turbinectomy) |
| Chronic atrophic | Saline/glucose irrigation, topical antibiotics, Vit A, oestrogen drops | Cavity narrowing (submucosal implants) |
| Allergic | INCS, antihistamines, leukotriene antagonists, AIT, omalizumab | Turbinate reduction if refractory |
9. Rhinoscopic Picture: Abscess & Haematoma of the Nasal Septum
Septal Haematoma
- Collection of blood between the septal cartilage and its perichondrium, usually following nasal trauma
- Appearance on anterior rhinoscopy: Smooth, rounded, fluctuant bluish-red swelling of both sides of the septum (bilateral); obliterates the nasal airway; soft to palpation (fluctuant); does NOT transilluminate clearly; midline bulge narrows both nasal passages
- Symptoms: bilateral nasal obstruction, pain, saddle deformity risk if untreated
- Urgent treatment: Incision and drainage (I&D) under LA; through-and-through quilting sutures or nasal packing to prevent re-accumulation; antibiotics to prevent secondary infection
Septal Abscess
- Secondary infection of a septal haematoma (most common) or spontaneous — S. aureus, H. influenzae, streptococci
- Appearance: Bilateral fluctuant swelling (identical to haematoma but now with systemic signs); erythema of overlying skin; extremely tender on palpation; fever and leucocytosis
- Distinguishing from haematoma: Pus on aspiration; fever, leukocytosis, warmth/tenderness of skin
- Dangers if untreated: Cartilage necrosis → saddle-nose deformity; spread to cavernous sinus → cavernous sinus thrombosis; meningitis; orbital cellulitis; brain abscess
- Treatment: Urgent I&D under GA; copious irrigation; systemic IV antibiotics (flucloxacillin + cephalosporin); cartilage reconstruction deferred if needed
10. Maxillary Sinusitis — Clinic, Diagnosis & Treatment
Acute Maxillary Sinusitis:
Clinical features:
- Pain/pressure over the cheek (infraorbital region); radiates to upper teeth
- Purulent unilateral nasal discharge (ipsilateral inferior meatus)
- Nasal obstruction; fever (38–39°C)
- Cheek tenderness on palpation; percussion of upper molar teeth painful
- Headache worse on bending forward or lying down
- Hyposmia
Anterior rhinoscopy: Purulent discharge in middle meatus; swollen middle turbinate
Diagnosis:
- Clinical diagnosis primarily
- Plain X-ray (Water's view): Opacification, mucosal thickening >6 mm, air-fluid level in antrum
- CT sinuses: Gold standard; shows opacification, ostiomeatal complex obstruction
- Diagnostic nasal endoscopy: pus from middle meatus
- Maxillary sinus puncture (antral lavage) — pus confirms diagnosis
Treatment (Acute):
- Amoxicillin-clavulanate 875/125 mg BD for 10–14 days; or doxycycline / respiratory fluoroquinolone
- Intranasal decongestants (oxymetazoline)
- Nasal saline irrigation
- Analgesia; steam inhalation
- Topical/oral corticosteroids to reduce oedema
Chronic Maxillary Sinusitis:
- Symptoms >12 weeks despite treatment
- Persistent purulent nasal discharge, hyposmia, facial fullness, post-nasal drip, cough
- CT: opacification, mucosal thickening, polyps, sclerosis of sinus walls
- Treatment: Prolonged antibiotics (macrolide: azithromycin 250 mg/day for 3 months for anti-inflammatory effect); nasal corticosteroids; FESS (Functional Endoscopic Sinus Surgery) — middle meatal antrostomy is first-line surgical approach; Caldwell-Luc for failed FESS or specific pathology
11. Frontitis (Frontal Sinusitis) — Clinic, Diagnosis & Treatment
Acute:
Clinical features:
- Severe frontal headache — localised to the forehead above the eye; worse in the morning (sinus fills overnight), relieved on standing; exacerbated by bending forward
- Tenderness on palpation/percussion of the floor of the frontal sinus (superomedial orbital rim)
- Fever, nasal obstruction, purulent discharge from middle meatus
- Periorbital oedema (Pott's puffy tumour if osteomyelitis develops)
Diagnosis:
- CT sinuses: opacification of frontal sinus, erosion of sinus floor in complications
- Endoscopy: pus from frontal recess
Treatment (Acute):
- IV antibiotics (amoxicillin-clavulanate or cefuroxime) if severe
- Nasal decongestants, corticosteroids to open frontal recess
- Frontal sinus trephination if medical treatment fails (see §16)
- FESS: Draf I/II/III procedures (frontal recess surgery → frontal sinusotomy)
Complications: Osteomyelitis of frontal bone (Pott's puffy tumour), orbital abscess, meningitis, frontal lobe abscess, superior sagittal sinus thrombosis
12. Ethmoiditis — Clinic, Diagnosis & Treatment
Acute:
Clinical features:
- Deep-seated pain between and behind the eyes ("inner canthal pain")
- Tenderness at medial canthus on palpation
- Periorbital oedema and erythema (most common orbital complication because the lamina papyracea is paper-thin)
- Purulent nasal discharge; nasal obstruction
- Fever; especially prominent in children
Diagnosis:
- CT sinuses: opacification of ethmoid air cells; erosion of lamina papyracea in complications
- Endoscopy: pus from middle/superior meatus
Treatment:
- Antibiotics (amoxicillin-clavulanate); IV if orbital complication suspected
- Nasal decongestants, saline irrigation
- Urgent orbital/ethmoid decompression if periorbital or orbital abscess develops (endoscopic ethmoidectomy or external ethmoidectomy)
- FESS: anterior + posterior ethmoidectomy for chronic ethmoiditis
13. Hemisinusitis — Clinic, Diagnosis & Treatment
Definition: Simultaneous inflammation of all ipsilateral paranasal sinuses (maxillary + ethmoid + frontal + sphenoid on one side).
Clinical Features:
- Combination of symptoms referable to all ipsilateral sinuses: facial pain/pressure on the affected side, unilateral nasal obstruction and purulent discharge, headache
- Pain may involve cheek, forehead, retro-orbital and vertex regions simultaneously (ipsilateral)
- Hyposmia (unilateral)
- Fever and systemic malaise
Diagnosis:
- CT sinuses: opacification of all paranasal sinuses on one side
- Endoscopy: pus from middle meatus (and sphenoethmoidal recess)
- Consider dental source (odontogenic) for ipsilateral maxillary/pan-ipsilateral disease
Treatment:
- Broad-spectrum antibiotics (amoxicillin-clavulanate or fluoroquinolone); IV if severe
- Nasal saline + decongestant + corticosteroid
- FESS on affected side: addresses all sinus ostia — maxillary antrostomy, anterior/posterior ethmoidectomy, frontal sinusotomy, sphenoidotomy
- Treat any dental source
14. Pansinusitis — Clinic, Diagnosis & Treatment
Definition: Bilateral simultaneous involvement of all paranasal sinuses (maxillary, ethmoid, frontal, sphenoid — bilaterally).
Clinical Features:
- Severe, generalised facial pain and pressure (bifrontal headache, bilateral cheek pain, retro-orbital pain)
- Bilateral dense nasal obstruction and profuse mucopurulent bilateral rhinorrhoea
- Post-nasal drip → chronic cough, pharyngitis
- High fever, systemic toxicity, malaise
- Complete anosmia
- Hyposmia, visual symptoms (if sphenoid involved — cavernous sinus proximity)
Diagnosis:
- CT sinuses: bilateral opacification of all sinus groups — gold standard
- Endoscopy: bilateral mucopurulent discharge from multiple drainage pathways
- Blood cultures if febrile; CRP/ESR elevated
- Rule out immunodeficiency (HIV, IgA deficiency), cystic fibrosis, primary ciliary dyskinesia
Treatment:
- Hospitalisation often required
- IV antibiotics (cefuroxime, amoxicillin-clavulanate; add metronidazole if anaerobic concern)
- Systemic corticosteroids (reduce polyp/oedema bulk)
- Nasal saline irrigation
- Bilateral FESS when acute phase controlled: bilateral middle meatal antrostomy + bilateral ethmoidectomy + frontal sinusotomy ± sphenoidotomy
- Long-term: maintenance INCS + macrolide therapy for chronic disease
15. Maxillotomy (Caldwell-Luc / Antrostomy) — Indications & Technique
Indications
(Cummings Otolaryngology)
- Complicated acute or chronic rhinosinusitis that has failed FESS
- Maxillary sinus foreign bodies
- Benign sinus tumours (e.g., inverted papilloma — combined with FESS)
- Trauma with displaced fractures of the maxillary sinus posterior/anterior wall
- Orbital decompression (combined approach)
- Odontogenic cysts of maxillary sinus
- Samter's triad (aspirin-exacerbated respiratory disease) with gross polyp disease
- Canine fossa trephination: adjunct in AFRS (allergic fungal rhinosinusitis) for clearing debris
Technique
- Anaesthesia: General anaesthesia preferred; infiltrate gingivobuccal sulcus with 1% lidocaine + 1:100,000 adrenaline; topical vasoconstrictor (oxymetazoline/cocaine pledgets) in nasal cavity
- Incision: In the gingivobuccal sulcus, above the canine fossa, leaving an adequate gingival cuff for closure; extend from lateral incisor to first molar; in children, place incision above secondary dentition (check with plain X-ray)
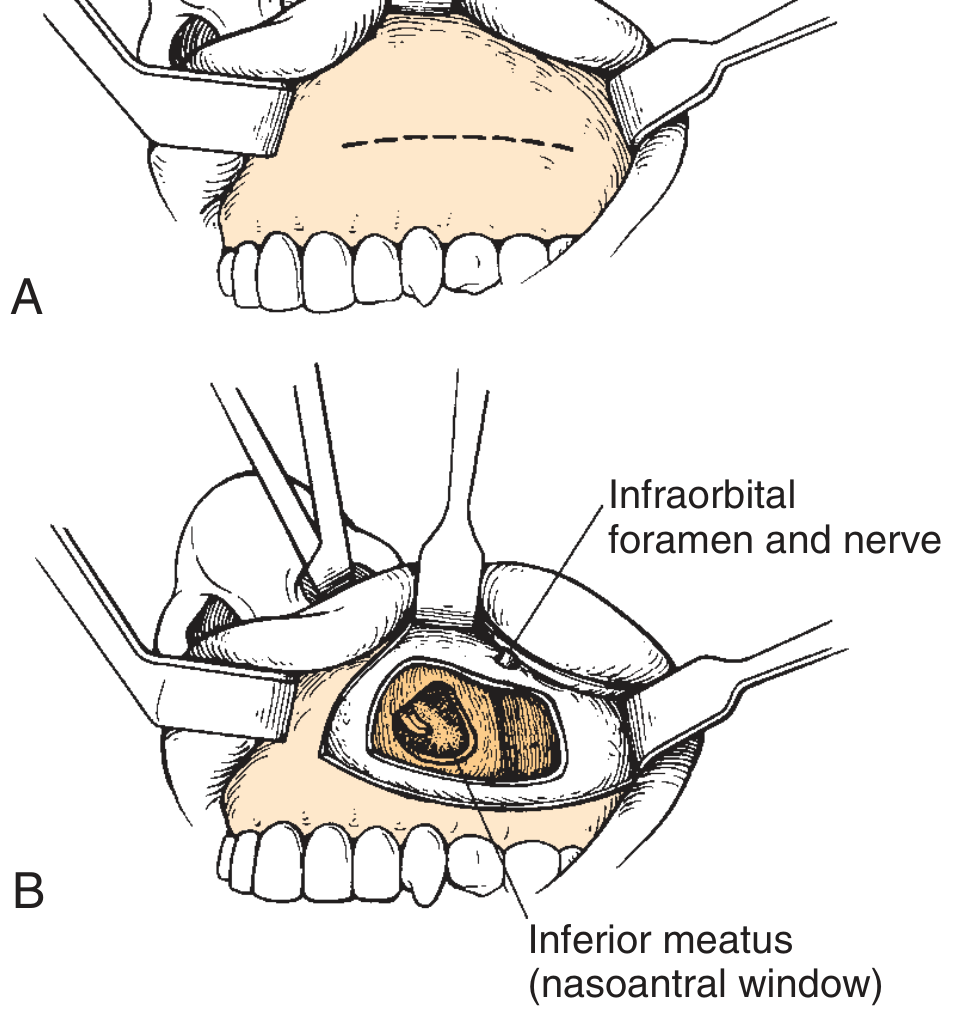
- Dissection: Incise through periosteum; elevate periosteal flap superiorly; identify and protect the infraorbital nerve
- Bony window: Use 4-mm osteotome or drill to create a window into the anterior wall of the maxillary antrum (thin bone); enlarge with Kerrison punch forceps; avoid infraorbital nerve and dental roots
- Intranasal antrostomy: Pass curved hemostat under inferior turbinate into nasal cavity; create nasoantral window ≥1 cm posterior to anterior end of inferior turbinate (avoids nasolacrimal duct and ASAA nerve); partial inferior turbinate removal or stenting prevents closure
- Sinus inspection: Endoscopic visualisation both through antrostomy and canine fossa window
- Closure: Gingivobuccal incision closed with absorbable suture (Vicryl)
Fig. 44.29 — Caldwell-Luc procedure: (A) Gingivobuccal sulcus incision above canine fossa; (B) Osteotome/drill used to create antral window with nasoantral drainage. — Cummings Otolaryngology
16. Frontotomy — Indication & Technique
Indications
- Acute frontal sinusitis failing medical therapy (severe headache, high fever, risk of complications)
- Frontal sinus mucocele/pyocele
- Chronic frontal sinusitis refractory to FESS (Draf I/IIa/IIb/III)
- Frontal sinus fracture with brain herniation or nasofrontal duct obstruction
- Benign tumours of the frontal sinus
- Complication: Pott's puffy tumour (osteomyelitis with subperiosteal abscess)
Types of Surgical Approaches
1. Trephination (Minimal invasive / bedside)
- Small drill hole through the floor of the frontal sinus (superomedial orbital rim)
- Used for acute emergency drainage or sampling
- Can be used to lavage/irrigate sinus
2. Endoscopic Frontal Sinusotomy (Draf classification):
- Draf I: Removal of agger nasi cells; clearance of frontal recess — minimally invasive
- Draf IIa: Enlargement of frontal ostium from lamina papyracea to middle turbinate
- Draf IIb: Extension across midline to nasal septum on ipsilateral side
- Draf III (Modified Lothrop): Bilateral frontal sinusotomies with removal of the intersinus septum and superior nasal septum — creates a single common drainage pathway; used for recalcitrant disease, mucocele, neo-osteogenesis
3. External (Osteoplastic) Frontal Sinusotomy:
- Bicoronal or brow incision
- Frontal bone flap raised (template drawn from Caldwell X-ray)
- Sinus completely exenterated + obliterated with abdominal fat (osteoplastic flap with fat obliteration)
- Reserved for failed endoscopic surgery, malignancy, irreversibly diseased sinus
17. Rhinosinusogenic Orbital Complications — Clinical Symptoms, Diagnosis & Treatment
Orbital complications arise most commonly from acute ethmoiditis (children) and frontal sinusitis (adults), due to the paper-thin lamina papyracea.
Chandler Classification (1970)
| Stage | Diagnosis | Features |
|---|
| I | Preseptal (periorbital) oedema | Inflammatory oedema anterior to orbital septum; no proptosis; full EOM |
| II | Orbital (postseptal) cellulitis | Diffuse oedema of orbital fat; mild proptosis; no discrete abscess; EOM restricted but not absent |
| III | Subperiosteal abscess | Pus between periorbita and bony wall (usually medial); proptosis; restricted + painful EOM; globe displaced |
| IV | Orbital abscess | Pus within orbital fat; severe proptosis; complete ophthalmoplegia; chemosis; vision threatened |
| V | Cavernous sinus thrombosis | Bilateral signs, high fever, toxicity, meningism; septic emboli to contralateral orbit |
Clinical Symptoms:
- Periorbital/eyelid erythema, oedema, warmth
- Proptosis (exophthalmos) — lateral and inferior displacement with medial subperiosteal abscess
- Ophthalmoplegia — restricted or painful eye movement
- Chemosis (conjunctival oedema)
- Reduced visual acuity, afferent pupillary defect — surgical emergency
- Fever, severe headache, toxicity
- Bilateral eye signs + meningism → cavernous sinus thrombosis
Diagnosis:
- CT orbits + sinuses with IV contrast: Differentiates preseptal from postseptal; identifies subperiosteal/orbital abscess; evaluates sinus source
- MRI: Superior for soft tissue, intracranial extension, cavernous sinus
- Ophthalmology assessment: visual acuity, pupil, EOM, fundoscopy (venous congestion)
- Blood cultures, FBC, CRP
Treatment:
- Chandler I–II: IV antibiotics (cefuroxime + metronidazole; or co-amoxiclav); nasal decongestants; INCS; close monitoring q4–6h for vision
- Chandler III–IV (abscess): Urgent surgical drainage — endoscopic medial orbital wall decompression + ethmoidectomy is preferred (FESS); external approach (Lynch incision) if endoscopic drainage fails or lesion is lateral
- Chandler V: IV antibiotics, anticoagulation (heparin — controversial), neurosurgical consultation; aggressive surgical drainage of all infected sinuses
- Indications for emergency surgery: Decreasing visual acuity, worsening proptosis despite 24–48h IV antibiotics, large abscess on CT
18. Rhinosinusogenic Intracranial Complications — Clinical Symptoms, Diagnosis & Treatment
Intracranial complications arise from direct extension, retrograde thrombophlebitis of valveless diploic veins (Breschet's veins), or haematogenous spread from frontal, ethmoid, or sphenoid sinusitis.
Types (Cummings Otolaryngology)
- Meningitis — most common intracranial complication
- Epidural abscess
- Subdural empyema — most dangerous (rapid spread in subdural space)
- Brain abscess (frontal lobe most common)
- Cavernous sinus thrombosis (from sphenoid/ethmoid sinusitis)
- Superior sagittal sinus thrombosis (from frontal sinusitis)
Clinical Symptoms
| Complication | Key Features |
|---|
| Meningitis | High fever, severe headache, neck stiffness (Kernig/Brudzinski positive), photophobia, altered consciousness |
| Epidural abscess | Persistent frontal headache; fever; relatively slow progression; "lucid interval" possible |
| Subdural empyema | Rapid onset; high fever, severe headache → focal neurological deficit → seizures → coma; neurosurgical emergency |
| Brain abscess | Headache, focal deficit (frontal: personality change, contralateral weakness), fever (low-grade), raised ICP signs (papilloedema, vomiting) |
| Cavernous sinus thrombosis | Bilateral eye involvement, severe headache, high fever, proptosis, chemosis, complete ophthalmoplegia, meningism; septic emboli |
| Superior sagittal sinus thrombosis | Bifrontal headache, bilateral limb weakness/seizures, raised ICP |
Diagnosis
- MRI brain + MRI venography — gold standard for all intracranial complications; identifies abscess, empyema, sinus thrombosis
- CT brain with IV contrast — initial investigation; ring-enhancing lesion (abscess); may miss early changes
- CT sinuses — identifies sinus source
- Lumbar puncture (meningitis): elevated WCC, protein; low glucose; culture & sensitivity (only if no raised ICP / no mass lesion on CT)
- Blood cultures, FBC, CRP, coagulation screen
Treatment
| Complication | Treatment |
|---|
| Meningitis | IV antibiotics: high-dose penicillin G + ceftriaxone ± metronidazole; dexamethasone; simultaneous FESS to drain offending sinus |
| Epidural abscess | IV antibiotics + urgent neurosurgical craniotomy + sinus drainage (FESS) |
| Subdural empyema | Emergency craniotomy (burr hole or craniotomy) + IV antibiotics + FESS |
| Brain abscess | IV antibiotics (ceftriaxone + metronidazole ± vancomycin); CT-guided stereotactic aspiration or craniotomy; FESS to drain sinus source |
| Cavernous sinus thrombosis | IV high-dose antibiotics; anticoagulation (heparin — evidence limited); bilateral sphenoid/ethmoid drainage; ophthalmology co-management |
| All complications | Multidisciplinary: ENT + Neurosurgery + Neurology + Infectious Disease; ICU monitoring |
Key principle: Surgical drainage of the intracranial complication and the causative sinus must be performed simultaneously or in rapid succession. Sinus drainage alone is insufficient.
References: Cummings Otolaryngology Head and Neck Surgery, 7th edition | K.J. Lee's Essential Otolaryngology, 11th edition