Detailed approach and treatment of spondylolysthesis from grade 1 to 5 in meryerding scale
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have everything needed for a thorough, well-cited response.
Spondylolisthesis: Approach and Treatment by Meyerding Grade
The Meyerding Grading Scale
Meyerding grading quantifies the degree of anterior vertebral slip relative to the width of the subjacent vertebral body (typically S1):
| Grade | Slip Percentage | Description |
|---|---|---|
| I | 0–25% | Low-grade |
| II | 25–50% | Low-grade |
| III | 50–75% | High-grade |
| IV | >75% | High-grade |
| V | >100% | Spondyloptosis — complete anterior displacement |
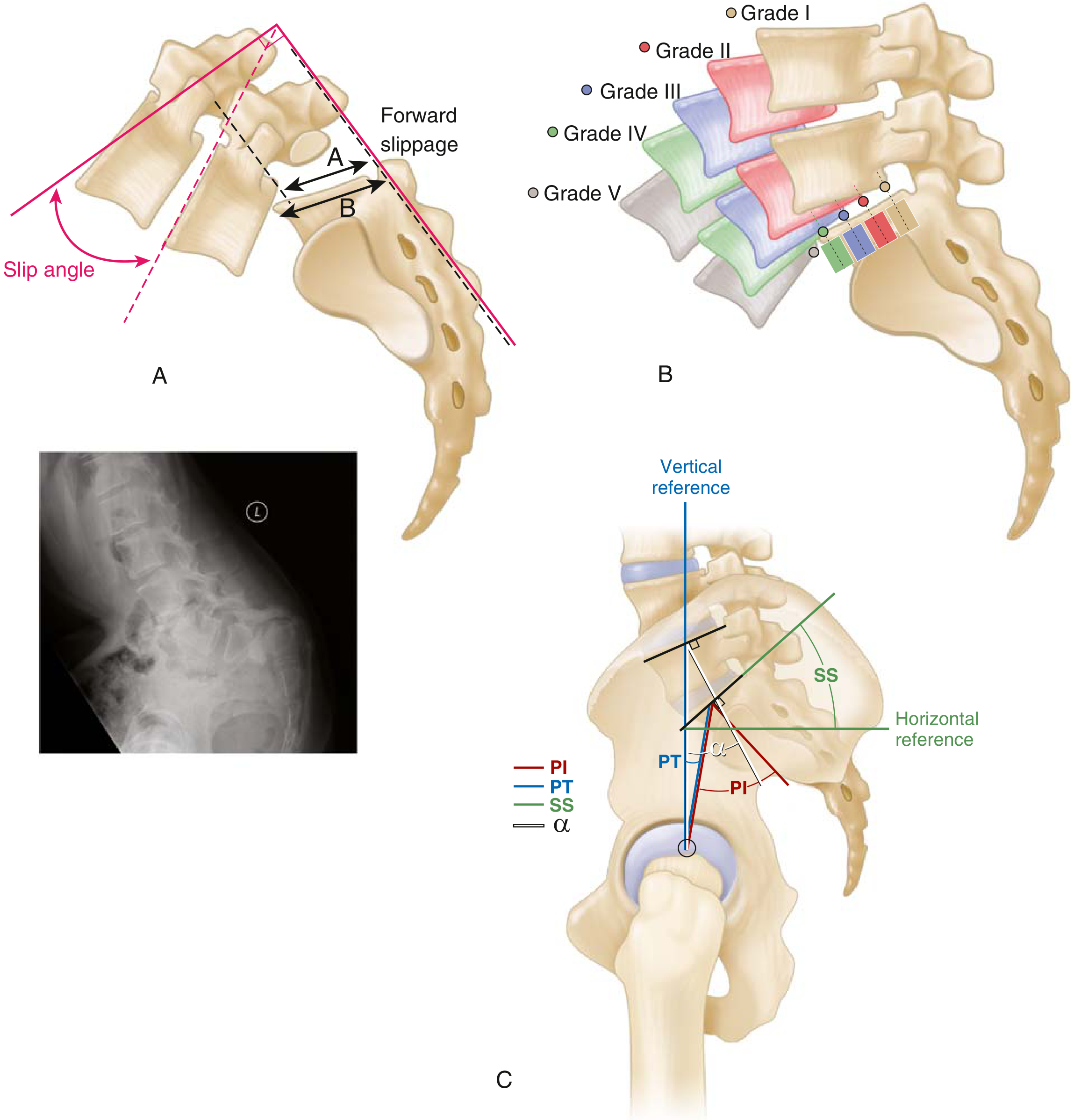
FIG. 8.21 — Meyerding grades I to V. The sacral body is divided into four segments; Grade V = spondyloptosis. Also shown: slip angle, pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS). — Miller's Review of Orthopaedics 9e
Additional Measurements Used Alongside Meyerding Grading
- Slip angle (normally <0°, indicating lordosis at L5–S1): measures lumbosacral kyphosis; >10° is a risk factor for progression
- Sacral inclination (normally >30°)
- Pelvic incidence (PI) (normally ~50°; elevated to 70–80° in spondylolisthesis patients): does NOT predict progression but predicts sagittal alignment demands
Wiltse-Newman Classification (Etiologic Types)
| Type | Age | Pathology |
|---|---|---|
| I — Dysplastic | Child | Congenital dysplasia of S1 superior facet |
| II — Isthmic* | 5–50 yr | Fracture/elongation of pars interarticularis (L5–S1) |
| III — Degenerative | >40 yr | Facet arthrosis → subluxation (L4–L5) |
| IV — Traumatic | Any | Acute fracture other than pars |
| V — Pathologic | Any | Incompetence of bony elements |
| VI — Postsurgical | Adult | Excessive resection of neural arch/facets |
Most common type — Miller's Review of Orthopaedics 9e
General Surgical Indications (Any Grade)
- Progression of slip (especially in skeletally immature patients)
- Neurologic deficit or persistent severe radiculopathy/weakness despite conservative care
- Intractable pain unresponsive to ≥3–6 months of nonoperative treatment
- High-grade slip (≥Grade III) in a growing child → prophylactic fusion recommended
Risk factors for progression: young age at presentation, female sex, slip angle >10°, high-grade slip, dysplastic type
Grade-by-Grade Approach
Grades I & II (Low-Grade: 0–50%)
Nonoperative Treatment (First-Line)
- Activity modification: restriction from high-risk sports (gymnastics, football linemen, weightlifting)
- Grade I asymptomatic: may return to contact sports once symptom-free
- Grade II asymptomatic: restricted from extension-dominant activities (gymnastics, football)
- Exercise: flexion-based core strengthening, hamstring stretching
- NSAIDs for pain control
- Bracing: considered for acute pars stress reactions, especially in adolescents
- Serial radiographic surveillance in skeletally immature patients to detect progression
Operative Treatment (When Conservative Fails)
- Reserved for intractable pain, progressive slippage, or neurologic compromise
- Procedure of choice: L5–S1 posterolateral in situ fusion (for isthmic/pediatric)
- The Wiltse paraspinal muscle-splitting approach to the lumbar transverse processes and sacral alae is widely used
- L5 radiculopathy is uncommon in children with low-grade slips; decompression is rarely needed
- Pars repair (Buck lag screw or Bradford tension band wiring + bone graft) is an option in young patients with <10% slip and a pars defect at L4 or above (spares L5–S1 motion segment)
- For adult isthmic Grade I/II: foraminal decompression + in situ posterolateral L5–S1 fusion ± instrumentation
Grades III, IV & V (High-Grade: >50% including Spondyloptosis)
Presentation
- More symptomatic with higher rate of progression
- L5 radiculopathy (exiting nerve root) — not S1 (distinguish from L5–S1 HNP)
- Cauda equina dysfunction (especially in dysplastic type where the neural arch is intact)
- Lumbosacral kyphosis, palpable step-off, hamstring tightness, altered gait ("pelvic waddle"), "heart-shaped" buttocks
Operative Treatment (Strongly Recommended)
- Prophylactic fusion is recommended in growing children with >50% slip (Grades III–V)
- Standard procedure: bilateral posterolateral fusion in situ, L4–S1 (with or without instrumentation)
- L4 must be included because L5 is too far anterior to achieve solid L5–S1 fusion at high grades
- Nerve root exploration/decompression: controversial; reserved for patients with clear-cut radicular pain or significant weakness
- Other described procedures:
- Posterior decompression + fibular interbody fusion + posterolateral fusion without reduction (Bohlman technique — excellent long-term results)
- L5 vertebrectomy (Gaines resection): for spondyloptosis (Grade V), involves removing L5 and fusing L4 to the sacrum
Reduction of the Listhesis — Controversial
- Carries a 20–30% incidence of L5 nerve root injury (most transient)
- Indications:
- Cosmetically unacceptable deformity
- Severe lumbosacral kyphosis (slip angle so severe that posterior fusion would be under tension without correction)
- In situ fusion at high-grade leaves such severe compensatory hyperlordosis above the fusion that long-term problems are common
- Close intraoperative and postoperative neurologic monitoring is mandatory
Degenerative Spondylolisthesis (Type III — Typically Grade I)
Epidemiology: More common in women >40 years, Black patients, and those with diabetes; most common at L4–L5
Presentation:
- Neurogenic claudication (central stenosis): leg heaviness/cramping, improved with flexion ("shopping cart sign")
- Nerve root compression (lateral recess stenosis): traversing L5 root compression between subluxated inferior facet of L4 and the posterosuperior body of L5
Treatment:
- Nonoperative: same as lumbar stenosis — activity modification, NSAIDs, physical therapy, epidural steroid injections
- Operative: decompression of nerve roots + posterolateral fusion with or without instrumentation
- SPORT Trial evidence: At 4-year follow-up, surgical patients had significantly better SF-36 Bodily Pain, Physical Function, and Oswestry Disability Index scores compared to nonoperative patients (both groups improved from baseline)
Summary Table
| Meyerding Grade | Slip | Primary Approach | Surgery |
|---|---|---|---|
| I | 0–25% | Conservative; RTP when asymptomatic | In situ L5–S1 PLF if failed/progressive |
| II | 25–50% | Conservative; restrict extension sports | In situ L5–S1 PLF; pars repair if <10% slip at L4+ |
| III | 50–75% | Surgical in growing child (prophylactic) | PLF L4–S1 ± decompression |
| IV | >75% | Surgical; stabilization essential | PLF L4–S1; reduction considered carefully |
| V (Spondyloptosis) | >100% | Surgical emergency if neurologic involvement | L5 vertebrectomy (Gaines) or PLF L4–S1 |
PLF = posterolateral fusion
Sources:
- Miller's Review of Orthopaedics 9th Edition, pp. 775–778
- SPORT Trial (Weinstein et al., 2009) — cited in Miller's
This is a shared conversation. Sign in to Orris to start your own chat.