
What is use for?
Based on the ingredient label, this is a male health / sexual wellness supplement tablet. Here's what each ingredient tells us about its purpose:
Primary Uses
1. Male Sexual Health & Libido
- L-Arginine (550 mg) — An amino acid that boosts nitric oxide production, improving blood flow and supporting erectile function.
- Maca Root (40 mg) — A Peruvian herb traditionally used to enhance libido, sexual desire, and energy.
- Tribulus Terrestris / Gokhru (30 mg) — A plant extract commonly used to support testosterone levels and male sexual performance.
- Korean Ginseng (20 mg) — An adaptogen known for improving stamina, reducing fatigue, and enhancing sexual function.
2. Testosterone & Reproductive Support
- Zinc (4 mg — 23.53% RDA) — Essential mineral for testosterone synthesis and sperm health.
- Selenium (25 mcg — 62.50% RDA) — Supports sperm motility and male fertility.
Summary
This tablet is designed to:
- Boost libido and sexual desire
- Support erectile function (via improved blood flow)
- Enhance male fertility (sperm quality/motility)
- Improve energy and stamina
It is a common formulation found in products marketed as men's performance or vitality supplements (similar to brands like Vigore, Manforce, or generic herbal men's health tablets sold in India/South Asia).
⚠️ These are dietary supplements, not medications. They are not FDA/drug-authority approved treatments for any medical condition. Consult a doctor for clinical concerns.
What is the best treatment for pre mature ejaculation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
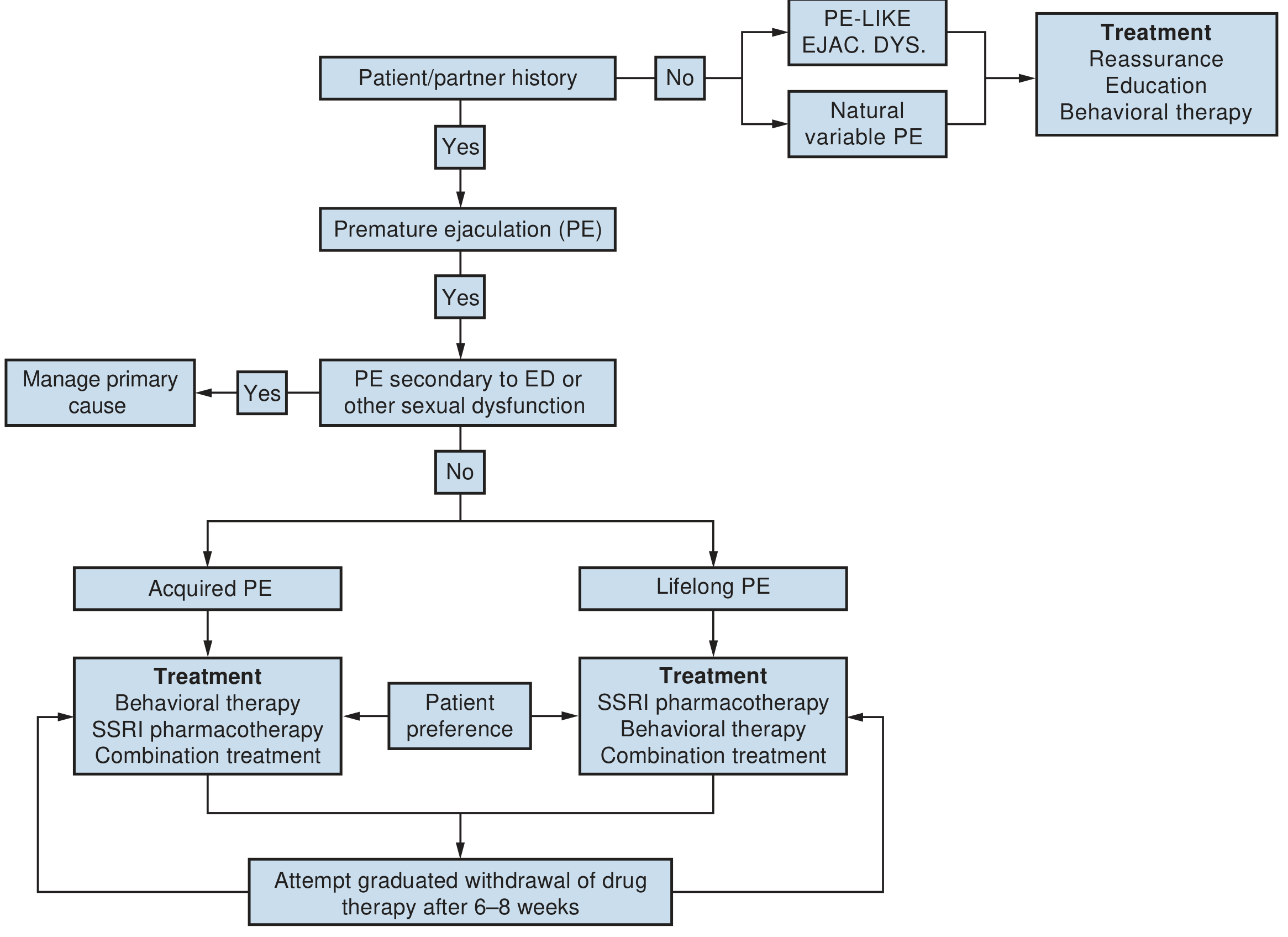
Here is a comprehensive, evidence-based overview of premature ejaculation (PE) treatment, sourced from Campbell-Walsh-Wein Urology and Textbook of Family Medicine 9e.
Treatment of Premature Ejaculation
Step 1 — Classify the Type of PE
Treatment depends on which type of PE is present:
| Type | Description |
|---|---|
| Lifelong (primary) | Present since first sexual encounters; neurobiologic basis |
| Acquired (secondary) | Develops later in life; often linked to ED or other medical causes |
| Natural variable | Occasional early ejaculation — a normal variation, not a disorder |
| PE-like / Subjective | Normal IELT but patient perceives it as premature; psychological/cultural cause |
If PE is secondary to erectile dysfunction (ED), treat the ED first — PE often resolves.
Treatment Algorithm
1. Behavioral / Psychosexual Therapy
These are first-line options, especially for acquired PE:
- Stop-Start technique (Semans): Sexual stimulation is stopped just before ejaculation, then resumed once the urge passes. Repeated to build control.
- Squeeze technique (Masters & Johnson): Partner squeezes the glans at the point of ejaculatory inevitability to suppress the ejaculatory reflex.
- Sensate focus exercises: Reduces performance anxiety and improves intimacy.
- Psychosexual counseling: Addresses underlying anxiety, relationship issues, or trauma.
Evidence base for behavioral therapy alone is modest, but it works well in combination with pharmacotherapy.
2. Pharmacotherapy (Most Effective for Lifelong PE)
A. SSRIs — First-Line Drug Treatment
SSRIs delay ejaculation by increasing serotonergic tone (delayed ejaculation is an established side effect exploited therapeutically).
| Drug | Dose | Regimen |
|---|---|---|
| Dapoxetine | 30–60 mg | On-demand (1–3 hrs before sex) — only SSRI designed for PE |
| Paroxetine | 10–40 mg | Daily OR on-demand |
| Sertraline | 25–200 mg | Daily OR on-demand |
| Fluoxetine | 20–40 mg | Daily |
| Clomipramine | 25–50 mg | Daily OR on-demand (TCA with serotonergic action) |
- Dapoxetine is the only drug specifically approved for PE in many countries (not FDA-approved in the US).
- Daily dosing generally more effective than on-demand.
- Graduated withdrawal after 6–8 weeks should be attempted.
B. Topical Anesthetics — On-Demand Option
Reduce penile sensitivity to delay ejaculation.
- Lidocaine/prilocaine cream or spray (e.g., EMLA cream, Fortacin spray)
- Applied 20–30 minutes before intercourse
- Wash off before penetration to avoid partner numbness
- Lower systemic side effects than oral drugs
C. PDE5 Inhibitors (if comorbid ED)
- Sildenafil, tadalafil — useful when PE coexists with erectile dysfunction
- Not effective for PE alone
3. Combination Treatment (Best Outcomes)
Combining SSRI pharmacotherapy + behavioral therapy gives superior results over either alone, and is recommended for both lifelong and acquired PE.
4. Reassurance & Education (For Variable/Subjective PE)
For men with normal IELT who perceive themselves as having PE:
- Education about normal ejaculatory latency
- Reassurance
- Behavioral therapy to improve perceived control
Key Points
- No drugs are FDA-approved specifically for PE in the US; SSRIs are used off-label.
- Lifelong PE responds best to SSRIs ± behavioral therapy.
- Acquired PE — always evaluate and treat underlying causes (ED, prostatitis, thyroid disease, anxiety).
- Psychological interventions alone have poor evidence but remain a valid option for willing patients.
— Campbell-Walsh-Wein Urology, pp. 2074–2084 | Textbook of Family Medicine 9e, p. Table 40-13
⚠️ This is educational information. Consult a urologist or sexual health physician for personalized treatment.
This is a shared conversation. Sign in to Orris to start your own chat.