70 year old male, with diabetes and HTN with past history of left pontine infarct with erectile dysfunction. What are the drugs which can cause this and what is the pharmacological management for such a patient
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
erectile dysfunction diabetes hypertension pharmacological management
Reading File
Reading File
Finding Sources
Finding Sources
Searching PubMed
"erectile dysfunction"[MeSH Terms] AND "phosphodiesterase 5 inhibitors"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have everything needed for a comprehensive, well-structured answer.
Erectile Dysfunction in a 70-Year-Old Male with Diabetes, HTN, and Past Left Pontine Infarct
Understanding the Clinical Context
This patient has multiple overlapping contributors to erectile dysfunction (ED):
- Age — prevalence of ED rises sharply with age: ~17% at 60–69 years, ~39% at ≥70 years
- Diabetes mellitus — peripheral autonomic neuropathy, endothelial dysfunction, and microangiopathy all impair the neurovascular axis of erection
- Hypertension — vascular disease is a primary driver; "what is bad for the heart is bad for the penis"
- Left pontine infarct — central neurogenic ED; the pons (medial pontine formation/nucleus paragigantocellularis) relays erectile signals from the MPOA/PVN down to sacral parasympathetic outflow. A pontine lesion disrupts this descending pathway, impairing psychogenic and reflexogenic erections
Part 1: Drugs That Can Cause or Worsen ED
Medications are implicated in up to 25% of ED cases. In this patient — on antihypertensives, potentially antidiabetics, and possibly cardiac drugs — a careful medication review is essential.
Antihypertensives
| Drug Class | Effect on Erectile Function | Mechanism |
|---|---|---|
| β-Blockers (atenolol, metoprolol, bisoprolol, propranolol) | Major contributor | Reduced cardiac output, CNS depression of libido, peripheral vasoconstriction, blockade of β2-mediated penile vasodilation |
| Thiazide diuretics (hydrochlorothiazide, chlorthalidone) | Major contributor | Reduced penile arterial flow due to volume/pressure effects; smooth muscle relaxation impairment |
| Central α₂-agonists (clonidine, methyldopa) | Significant | Antagonize hypothalamic α₂-adrenoceptors; clonidine also has peripheral effects reducing corporal smooth muscle relaxation |
| Verapamil (calcium channel blocker) | Moderate | Linked to ejaculatory complaints; reduced bulbocavernosus muscle force |
| Spironolactone | Significant | Antiandrogen effect via progesterone/androgen receptor binding → loss of libido, gynecomastia, ED |
| ACE inhibitors | Neutral to beneficial | No adverse effect; may improve erectile function via RAS pathway |
| ARBs (losartan, valsartan) | Beneficial | Reverse penile vascular structural changes; losartan improved sexual function at 3 months; valsartan was superior to carvedilol in a crossover trial |
| α₁-blockers (doxazosin) | Neutral to beneficial | Increase cavernosal smooth muscle relaxation |
Cardiac Drugs
| Drug | Effect | Mechanism |
|---|---|---|
| Digoxin | ED | Inhibits Na⁺/K⁺-ATPase in corporal smooth muscle; also antiandrogen effect by raising SHBG |
| Amiodarone | ED | Structural similarity to thyroid hormone; induces hypothyroidism/hypogonadism |
Psychotropics / Antidepressants
| Drug | Effect | Mechanism |
|---|---|---|
| SSRIs (sertraline, fluoxetine, paroxetine) | Significant | Serotonin-mediated suppression of dopaminergic pro-erectile pathways; delayed ejaculation and ED |
| TCAs | Significant | Anticholinergic effects impair parasympathetically mediated erection |
| MAOIs | Significant | Central serotonin excess |
| Alprazolam, diazepam | Moderate | CNS depression |
Hormonal / Endocrine Agents
| Drug | Effect |
|---|---|
| 5α-reductase inhibitors (finasteride, dutasteride) | ED, reduced libido via decreased DHT |
| Antiandrogens (flutamide, cyproterone) | Direct androgen receptor blockade |
| GnRH agonists (leuprolide, goserelin) | Castrate testosterone levels |
| Corticosteroids | Suppress HPG axis |
| Ketoconazole | Inhibits testosterone synthesis |
Other Agents
| Drug | Effect |
|---|---|
| H₂ blockers (cimetidine, ranitidine) | Antiandrogen (cimetidine blocks androgen receptors) |
| Opioids (methadone, morphine) | Hypogonadotropic hypogonadism |
| Alcohol (chronic) | Gonadotoxic, hepatotoxic → low testosterone |
| GLP-1 agonists (dulaglutide) | Protective — associated with reduced incidence of ED in diabetic men |
Part 2: Pharmacological Management in This Specific Patient
Step 0 — Optimize Medications First
- Switch β-blocker + thiazide (if used) to an ARB ± calcium channel blocker if BP control allows — ARBs actively improve erectile function
- Avoid or minimize spironolactone, clonidine, digoxin if alternatives exist
- Review SSRIs — if antidepressant needed, bupropion is preferred (least impact on sexual function)
Step 1 — Lifestyle Modifications
- Glycaemic control (HbA1c optimization) — directly reduces endothelial dysfunction
- Weight loss — improves sexual function in obese patients
- Smoking cessation, alcohol moderation
- GLP-1 agonist (e.g., dulaglutide) if on antidiabetic therapy — has shown protective association with ED
Step 2 — First-Line: PDE-5 Inhibitors
Mechanism: Nitric oxide (NO) → ↑ cGMP in cavernosal smooth muscle → relaxation and engorgement. PDE-5 inhibitors prevent cGMP breakdown, sustaining erection.
| Drug | Dose | Onset | Duration | Notes |
|---|---|---|---|---|
| Sildenafil (Viagra) | 25–50 mg on-demand (↑ to 100 mg) | 30–60 min | 4–6 h | Take on empty stomach; starting dose 25 mg in elderly |
| Vardenafil (Levitra) | 5–20 mg on-demand | 30–60 min | 4–6 h | Similar to sildenafil |
| Tadalafil (Cialis) | 10–20 mg on-demand or 2.5–5 mg daily | 30 min | Up to 36 h | Preferred in elderly — daily dosing option avoids "on-demand" pressure; also treats BPH |
| Avanafil | 50–200 mg on-demand | 15–30 min | 6 h | Most selective PDE-5 |
Efficacy: ~60% overall; lower in diabetic/neurogenic ED (~40–50%) but still clinically meaningful. PDE-5 inhibitors are effective in neurogenic ED (including post-stroke).
Critical safety consideration for this patient:
- ABSOLUTE CONTRAINDICATION: Do NOT combine with nitrates (accumulation of cGMP → profound hypotension)
- Caution with α-blockers — risk of orthostatic hypotension; use lowest dose, separated by 4 hours
- Pontine infarct — no direct contraindication; central neurogenic ED may show attenuated response but PDE-5 inhibitors remain first-line
Step 3 — Second-Line Options (if PDE-5 inhibitors fail or are inadequate)
a) Intracavernosal injection (ICI) — most effective second-line therapy
- Alprostadil (prostaglandin E₁): 2.5–60 mcg injected directly into corpus cavernosum with 27–30 gauge needle
- Alternatively: trimix (papaverine + phentolamine + alprostadil)
- Onset: 5–10 min; erection lasts 30–60 min
- Side effects: pain, fibrosis, priapism
b) Intraurethral alprostadil (MUSE)
- 125–1000 mcg suppository into urethra
- Less invasive than ICI; efficacy 30–66%
c) Vacuum erection device (VED)
- Mechanical; no drug interactions; safe in cardiovascular disease
- Creates negative pressure to draw blood into corpus cavernosum
Step 4 — Hormonal Assessment
- Check morning serum testosterone
- If testosterone < 275 ng/dL + symptoms of hypogonadism → testosterone gel (or other formulation) — moderately effective; adding testosterone to a partial PDE-5 responder may provide synergistic benefit via upregulation of PDE-5 receptors
Step 5 — Third-Line: Penile Prosthesis
Surgical implantation of semi-rigid (malleable) or inflatable penile prosthesis for men refractory to all pharmacological options. High long-term patient satisfaction but reserved for those who prefer a permanent solution.
Treatment Algorithm
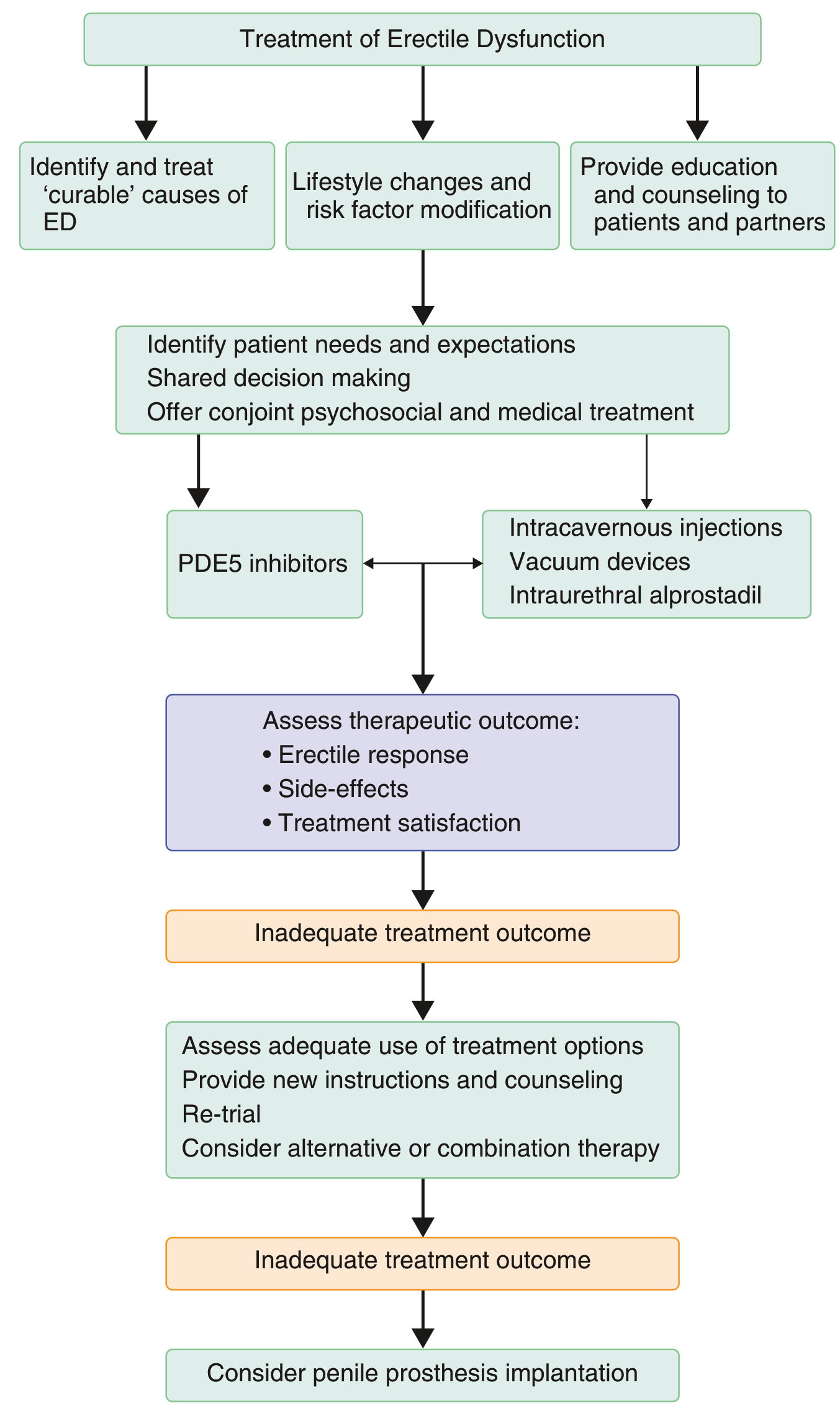
Summary: Practical Approach for This Patient
| Priority | Action |
|---|---|
| 1 | Review medications — switch to ARB-based antihypertension; stop/switch thiazide + β-blocker if possible |
| 2 | Optimize diabetes (HbA1c) and BP; consider GLP-1 agonist |
| 3 | Start tadalafil 5 mg daily (preferred in elderly with diabetes + neurogenic component) |
| 4 | If PDE-5 inhibitor inadequate after 6–8 attempts → ICI with alprostadil or trimix |
| 5 | Check testosterone; replace if deficient |
| 6 | Psychosexual counselling alongside medical treatment |
| 7 | Last resort: penile prosthesis |
Key sources: Goldman-Cecil Medicine 22E, pp. 2543–2544 | Textbook of Family Medicine 9e, pp. 1193–1194, 1261 | Campbell-Walsh-Wein Urology, pp. 1989–1993
This is a shared conversation. Sign in to Orris to start your own chat.