Variable angle body plate orthopaedics 10 marks pg answer with flow chart and images
variable angle body plate orthopaedics PG exam answer uses design principles
variable angle locking plate design biomechanics advantages disadvantages orthopaedic surgery
https://www.siiora.com/blogs/understanding-the-variable-lock…
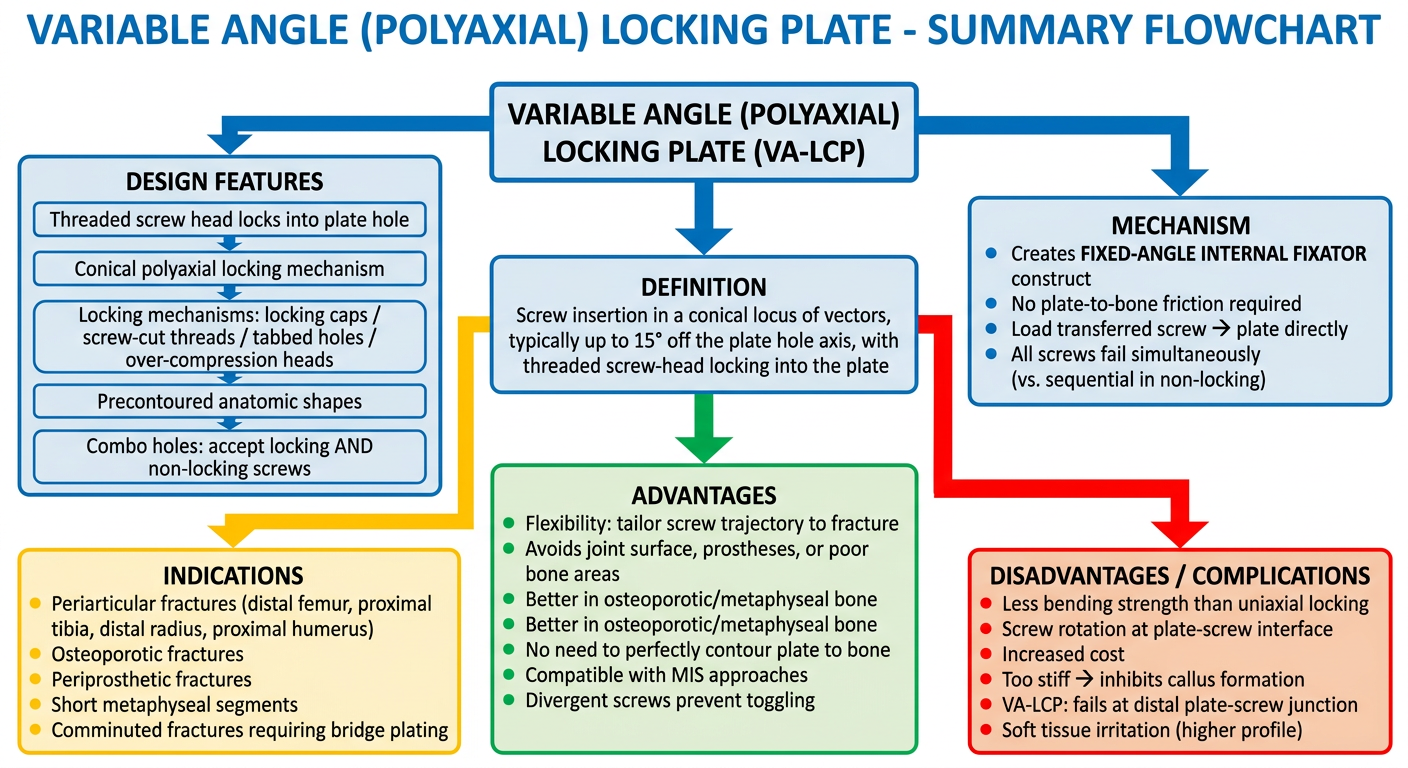
A detailed medical educational flowchart titled "Variable Angle (Polyaxial) Locking Plate - Summary Flowchart" for orthopaedic surgery PG exam. The flowchart should show the following hierarchy and flow in a clean, labeled diagram style with boxes and arrows: Top box: "VARIABLE ANGLE (POLYAXIAL) LOCKING PLATE (VA-LCP)" Branch 1 - Definition box: "Screw insertion in a conical locus of vectors, typically up to 15° off the plate hole axis, with threaded screw-head locking into the plate" Branch 2 - Design Features box with sub-boxes: - "Threaded screw head locks into plate hole" - "Conical polyaxial locking mechanism" - "Locking mechanisms: locking caps / screw-cut threads / tabbed holes / over-compression heads" - "Precontoured anatomic shapes" - "Combo holes: accept locking AND non-locking screws" Branch 3 - Mechanism box: - "Creates FIXED-ANGLE INTERNAL FIXATOR construct" - "No plate-to-bone friction required" - "Load transferred screw → plate directly" - "All screws fail simultaneously (vs. sequential in non-locking)" Branch 4 - Advantages box: - "Flexibility: tailor screw trajectory to fracture" - "Avoids joint surface, prostheses, or poor bone areas" - "Better in osteoporotic/metaphyseal bone" - "No need to perfectly contour plate to bone" - "Compatible with MIS approaches" - "Divergent screws prevent toggling" Branch 5 - Indications box: - "Periarticular fractures (distal femur, proximal tibia, distal radius, proximal humerus)" - "Osteoporotic fractures" - "Periprosthetic fractures" - "Short metaphyseal segments" - "Comminuted fractures requiring bridge plating" Branch 6 - Disadvantages / Complications box (red/orange): - "Less bending strength than uniaxial locking" - "Screw rotation at plate-screw interface" - "Increased cost" - "Too stiff → inhibits callus formation" - "VA-LCP: fails at distal plate-screw junction" - "Soft tissue irritation (higher profile)" All boxes should be clearly labeled, connected with arrows, color-coded (blue for design, green for advantages, red for disadvantages, yellow for indications). Professional medical diagram style, white background.
Variable Angle (Polyaxial) Locking Plate - 10 Marks PG Answer
1. Definition
- Rockwood and Green's Fractures in Adults, 10th ed. 2025
2. Historical Context and Evolution
- Non-locking plates - relied on plate-to-bone friction (dependent on bone quality)
- Uniaxial locking plates (LISS, LCP) - screw head threads into plate at a fixed single angle; angular stability; act as internal fixators independent of bone quality
- Variable angle locking plates (VA-LCP) - introduced to free the surgeon from fixed screw trajectories while retaining locking stability

3. Design Features
Screw-Plate Interface Mechanisms (varies by manufacturer):
| Mechanism Type | Description |
|---|---|
| Locking caps | Cap locks screw into plate at variable angle |
| Over-compression screw heads | Screw head compresses into polyaxial socket |
| Screws cutting threads into plate | Self-threading into the plate hole at the inserted angle |
| Tabbed screw holes | Tabs deform to lock screw at the angle of insertion |
Key structural elements:
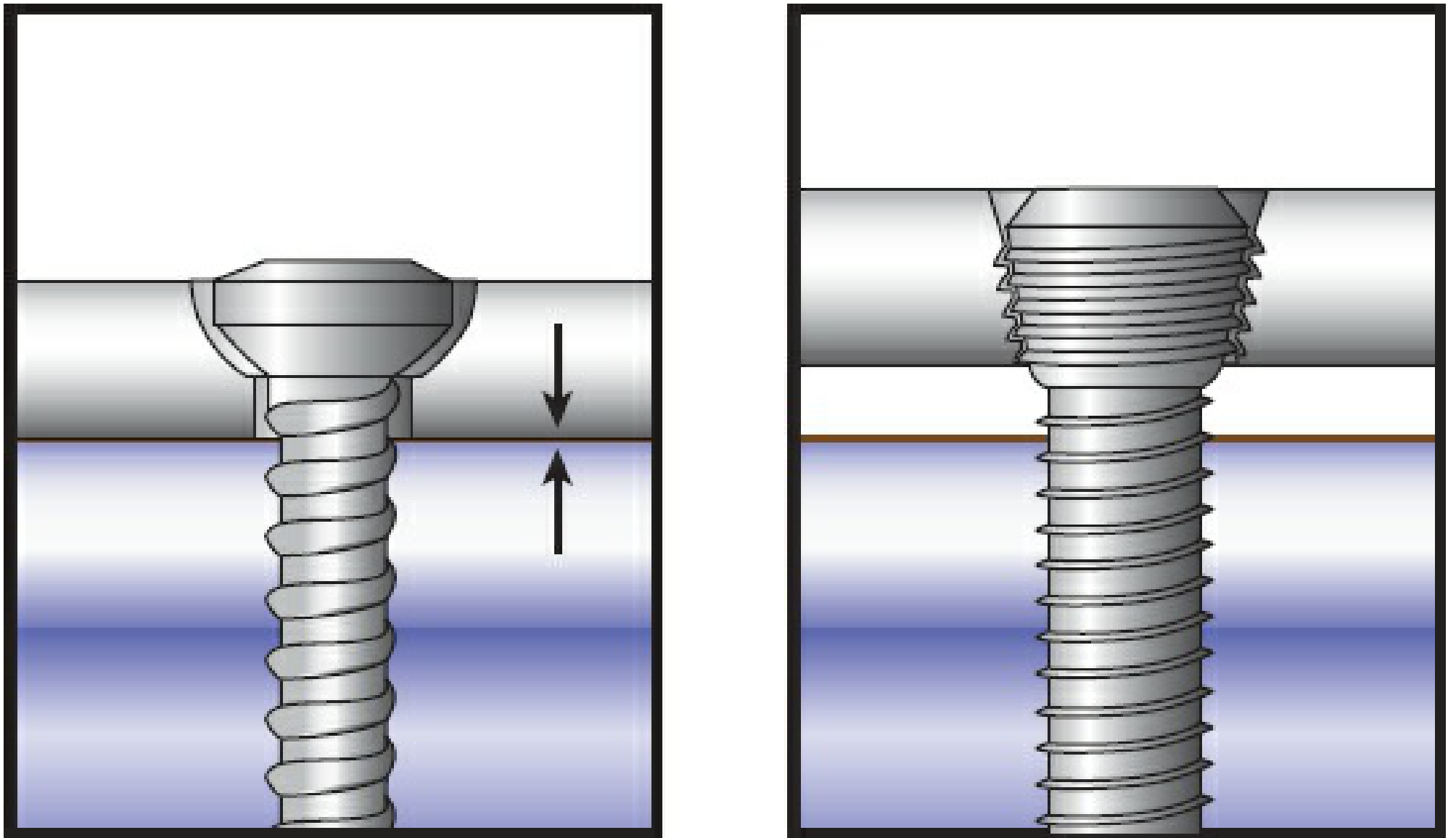
- Threaded screw head engages matching threads in the plate hole
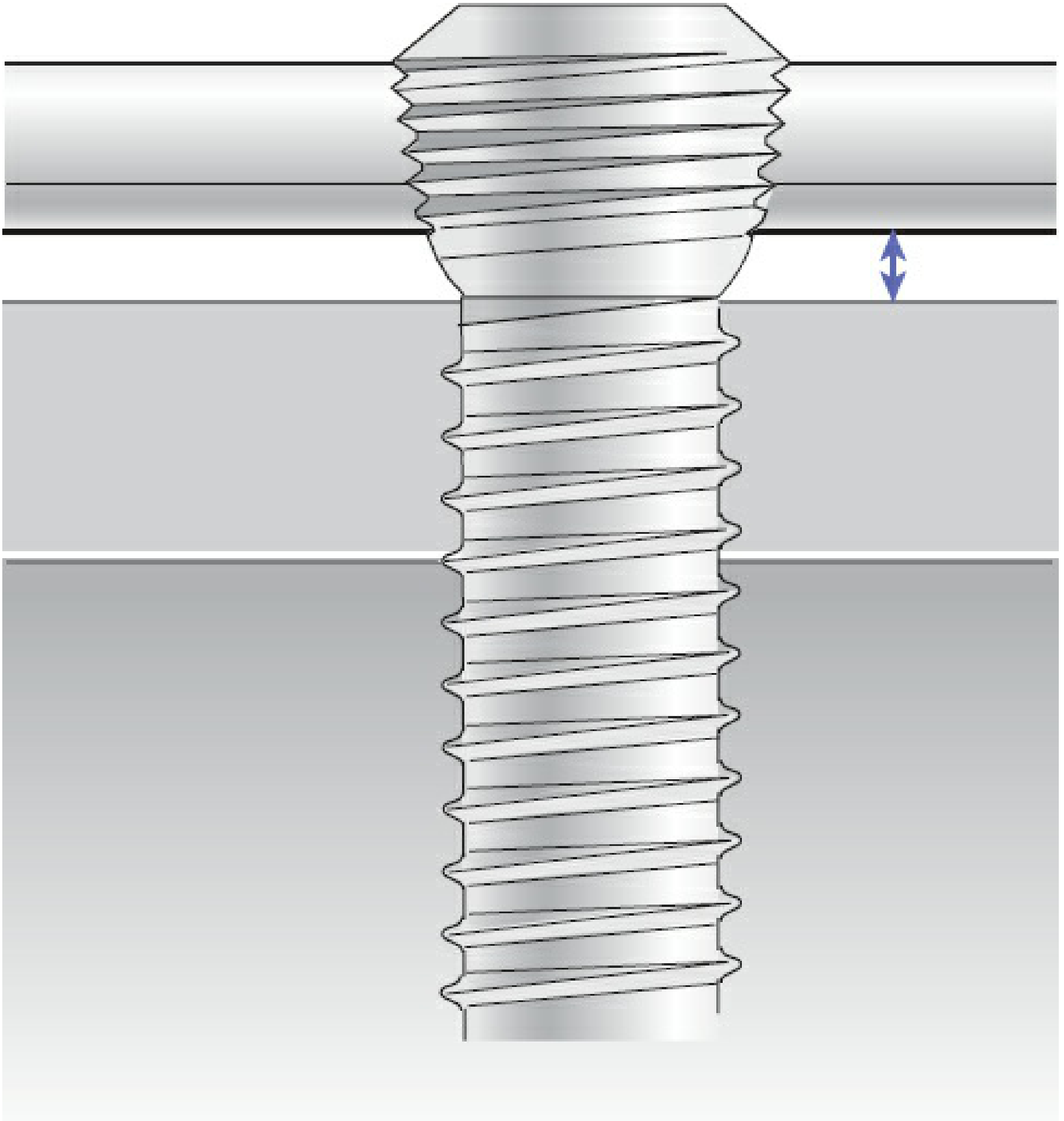
- Conical hole geometry permits ±15° off-axis angulation in any direction
- Combination holes - many designs accept BOTH locking and non-locking screws in the same hole
- Anatomically precontoured shapes for periarticular sites (distal femur, proximal tibia, distal radius, proximal humerus, clavicle)
- Larger core diameter of locking screws with finer thread pitch - designed for bending strength over stripping torque
4. Biomechanical Principles
- Stability = friction force between plate and bone
- Load exceeding friction → screw toggles and loosens sequentially
- Entirely dependent on bone quality/density
- Threaded screw head locks into plate → fixed-angle device
- No plate-to-bone contact required
- Load transfers directly: bone → screw → plate (compressive stresses at screw-bone interface)
- All screws fail simultaneously (not sequentially)
- Angular stability distributes stress more uniformly across all screw-bone interfaces
- Same locking principle, but screw can be inserted off-axis (up to 15°)
- As off-axis angle increases, locking interface resistance DECREASES nearly linearly
- Bending stability reduced to 63% and 31% with 5° and 10° axis deviation respectively
- Maximum stability achieved when screw is inserted perpendicular (on-axis) to plate
5. Flowchart
6. Indications
| Clinical Scenario | Rationale |
|---|---|
| Periarticular fractures (distal femur, proximal tibia, distal radius, proximal humerus) | Short metaphyseal segment; poor bone quality near joint |
| Osteoporotic fractures | Screw locking independent of bone density; no pull-out risk |
| Periprosthetic fractures | VA screws can redirect to avoid prosthesis |
| Comminuted fractures (bridge plating) | Screw trajectories tailored to available bone fragments |
| Plate-bone mismatch | Locked screw does not drag bone to plate, preserving reduction |
| Clavicle fractures | Precontoured VA-LCP when plate not centred perfectly |
| Distal radius fractures | VA allows fragment-specific fixation up to 15° off-axis |
7. Advantages
- Surgical flexibility - surgeon selects screw trajectory based on fracture geometry, bone quality, and existing hardware; not dictated by fixed plate design
- Better fixation in challenging anatomy - screw can target denser bone regions, avoid joints or articular surfaces, and navigate around prior implants
- Osteoporotic bone - angular stability without relying on bone purchase; significantly reduces screw pull-out risk
- No perfect plate contouring required - locked screws do not drag bone to plate, preserving reduction
- MIS compatibility - precontoured plates allow submuscular insertion with minimal soft tissue stripping
- Divergent screw trajectories - multiple divergent screws resist toggling better than parallel screws in comminuted metaphyseal fractures
- Hybrid construct option - non-locking screws can be used first for compression and reduction, then locking screws for stability
8. Disadvantages and Complications
| Disadvantage | Mechanism |
|---|---|
| Reduced locking strength vs. uniaxial | Off-axis insertion reduces screw-plate thread engagement; VA mechanisms inherently less stable than fixed-angle |
| Screw rotation at plate-screw interface | Clinical failures reported where VA screws rotate under load; standard locking provides greater rotational resistance |
| Higher cost | More complex manufacturing vs. conventional plates |
| Construct over-stiffness | May create environment too rigid for callus formation in some fracture types |
| Specific failure pattern | VA-LCP plates for distal femur tend to fail at the distal plate-screw junction |
| Soft tissue irritation | Higher profile implants in subcutaneous locations (e.g., clavicle, distal radius) |
| Clinical effectiveness unproven | Comparative clinical superiority over standard locking plates remains unproven in literature |
- Rockwood and Green's, 2025, pp. 492-506
9. Specific Clinical Applications
Distal Femur (VA-LCP):
- Locking plates with polyaxial screw capabilities allow variable insertion angles to optimize screw placement in complex fracture patterns or with preexisting hardware
- VA-LCP plates specifically fail at the distal plate-screw junction (unlike LISS which fails at shaft fixation, or stainless steel which fails within working length)
- Polyaxial screws provided greatest resistance to rotation when inserted perpendicular to the plate - resistance decreased as off-axis angle increased
Distal Radius (VA-LCP 2.4):
- Screws can diverge up to 15° in any variable angle hole in the plate head
- Enables fragment-specific fixation of complex intra-articular fractures
- Allows buttressing of subchondral bone without mandatory far-cortex penetration
Proximal Humerus / Clavicle:
- Variable angle holes useful when the plate is not positioned perfectly central on the bone
- Clavicle VA-LCP: locking plate placed superiorly is biomechanically superior to conventional compression plate
10. Key Exam Points to Remember
- VA = Polyaxial = permits ±15° off-axis screw insertion
- More flexibility = less locking strength (inverse relationship)
- Screw perpendicular to plate = maximum strength
- Specific failure: VA-LCP distal femur fails at distal plate-screw junction
- Standard locking > VA locking for rotational resistance at screw-plate interface
- Acts as an internal fixator (not reliant on plate-bone friction)
- All screws fail simultaneously (vs. sequential in non-locking)
- Especially valuable in: osteoporotic bone, periarticular fractures, periprosthetic fractures