Tell me everything I need to know about " Popliteal Fossa, Popliteal Artery and Popliteal vein" it's features and everything in concise heading way and simple words, easier for me to understand
Reading File
Finding Sources
Finding Sources
Searching Images
popliteal fossa anatomy contents
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive, well-structured answer. Here it is:
Popliteal Fossa, Popliteal Artery & Popliteal Vein
🔷 POPLITEAL FOSSA
What Is It?
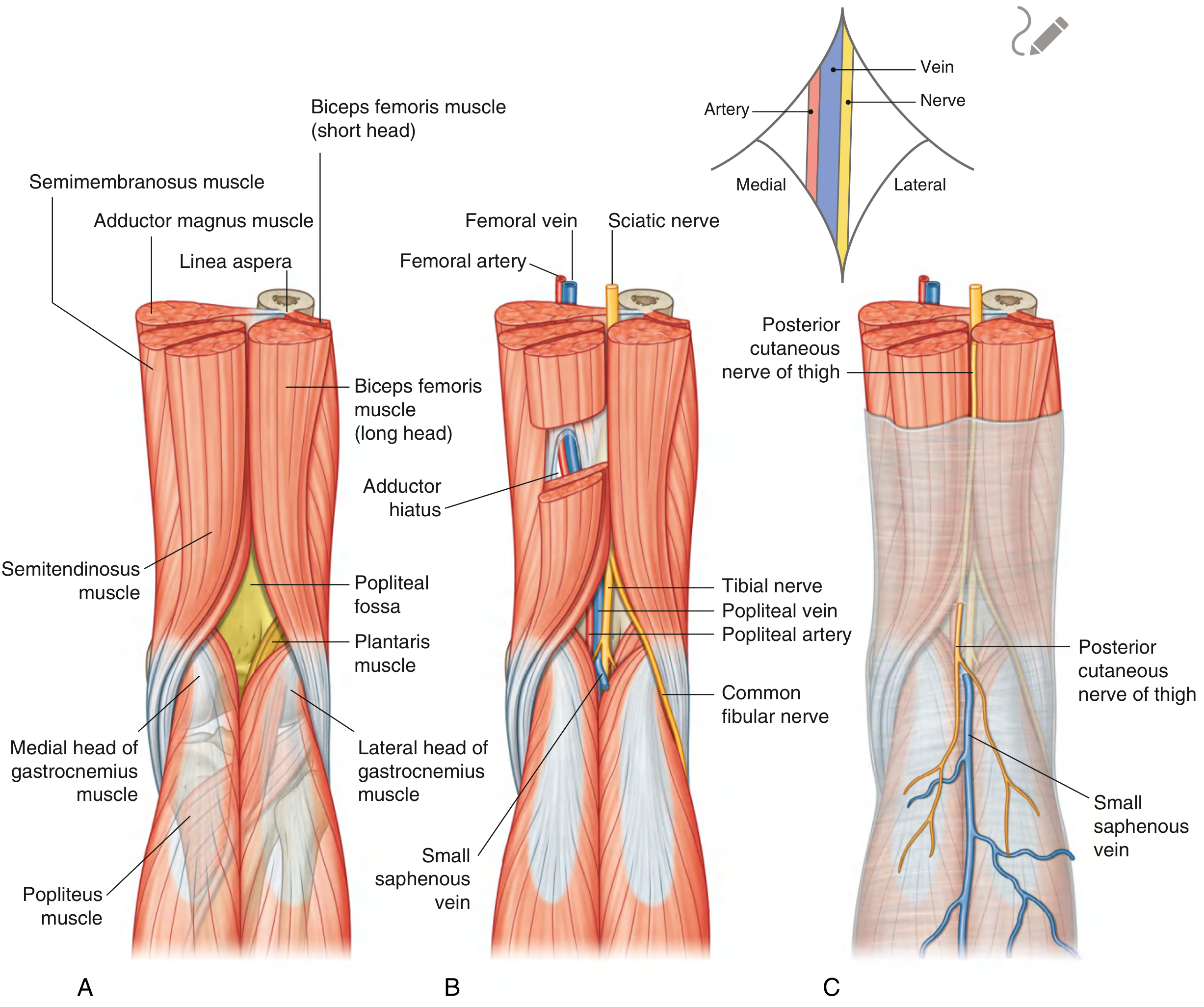
The popliteal fossa is a diamond-shaped hollow space located behind the knee joint. Think of it as the "back of the knee pit." It is the main passageway for structures traveling between the thigh and the leg.
Shape & Boundaries
The diamond has 4 corners (borders), made by muscles:
| Border | Muscle |
|---|---|
| Upper-medial | Semitendinosus + Semimembranosus |
| Upper-lateral | Biceps femoris |
| Lower-medial | Medial head of gastrocnemius |
| Lower-lateral | Plantaris + Lateral head of gastrocnemius |
Floor (Bottom of the pit)
- Upper part → back of the femur (popliteal surface) + joint capsule of the knee
- Lower part → popliteus muscle
Roof (Lid of the pit)
- Covered by deep fascia (a tough sheet of connective tissue)
- This fascia is continuous with:
- Fascia lata (thigh fascia) above
- Deep fascia of the leg below
- Two structures pierce the roof:
- Small saphenous vein (drains into the popliteal vein here)
- Posterior cutaneous nerve of the thigh (supplies skin on back of leg)
Contents (What's Inside?)
The fossa contains 3 main neurovascular structures — arranged from superficial to deep:
MOST SUPERFICIAL ──► Tibial nerve + Common fibular nerve
│
Popliteal vein
│
DEEPEST ────────► Popliteal artery
Memory tip: From back to front = Nerve → Vein → Artery (NVA)
Also present:
- Popliteal lymph nodes — drain the knee joint and the back of the leg
- Fat — fills the space and pads the structures
- Small saphenous vein — in the superficial fascia of the roof
Nerves Inside the Fossa
1. Tibial Nerve
- Larger branch of the sciatic nerve
- Runs vertically down through the fossa
- Exits deep to the plantaris muscle → enters the posterior compartment of the leg
- Gives branches to the gastrocnemius, soleus, and plantaris muscles
2. Common Fibular (Peroneal) Nerve
- Smaller branch of the sciatic nerve
- Follows the biceps femoris tendon laterally
- Wraps around the neck of the fibula → enters the lateral compartment of the leg
- More at risk of injury (lies superficially near the fibular head)
🔴 POPLITEAL ARTERY
What Is It?
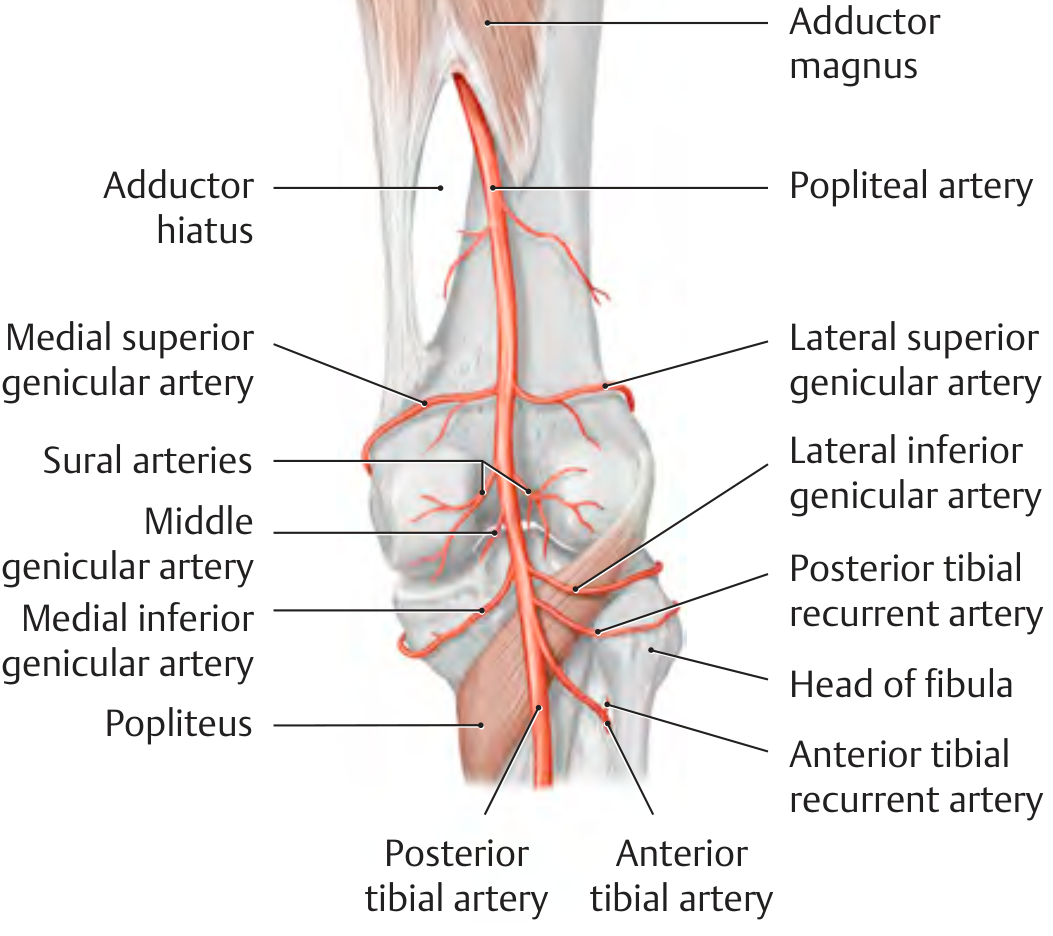
The popliteal artery is the direct continuation of the femoral artery. It begins when the femoral artery passes through a gap in the adductor magnus muscle called the adductor hiatus.
Course (Path)
- Enters the popliteal fossa from the upper medial side (under semimembranosus)
- Descends obliquely (diagonally) through the fossa
- Travels alongside the tibial nerve
- Exits at the lower end of the fossa by passing under the popliteus muscle
- Divides just below the popliteus into:
- Anterior tibial artery → goes to the front of the leg
- Posterior tibial artery → continues down the back of the leg
Position in the Fossa
- It is the DEEPEST of all the neurovascular structures
- Lies closest to the knee joint capsule and bone
- This makes it hard to palpate but a pulse can be felt with deep pressure near the midline behind the knee
Branches (Given Off in the Fossa)
| Branch | What it Supplies |
|---|---|
| Medial superior genicular artery | Superomedial knee |
| Lateral superior genicular artery | Superolateral knee |
| Middle genicular artery | Pierces joint capsule → supplies cruciate ligaments |
| Medial inferior genicular artery | Inferomedial knee |
| Lateral inferior genicular artery | Inferolateral knee |
| Sural arteries (paired) | Both heads of gastrocnemius muscle |
All genicular arteries (except middle) join together to form the articular rete of the knee — a vascular network that helps supply the knee even when the main artery is compressed during flexion.
Clinical Points — Popliteal Artery
Popliteal Artery Aneurysm
- Abnormal dilation of the artery — considered aneurysmal when diameter > 7 mm
- Most commonly associated with aneurysms elsewhere (femoral artery, aorta)
- Tends to thrombose (clot) rather than rupture
- Main danger: blood clots breaking off → distal embolization → limb ischemia → possible amputation
- Diagnosed with ultrasound + Doppler
- Must surgically repair due to high thromboembolic risk
Popliteal Artery Entrapment Syndrome (PAES)
- An abnormally positioned gastrocnemius muscle compresses the popliteal artery
- Causes leg pain during exercise, especially on plantar flexion
- Seen in young, active individuals
🔵 POPLITEAL VEIN
What Is It?
The popliteal vein is the main vein draining the leg at the knee level. It forms when the anterior and posterior tibial veins join together.
Course
- Formed at the lower end of the popliteal fossa by the joining of tibial veins
- Travels alongside the popliteal artery (superficial to it)
- The two travel together wrapped in a common fascial sheath
- Exits the fossa superiorly through the adductor hiatus
- Becomes the femoral vein once it passes through the hiatus
Position in the Fossa
- Lies between the tibial nerve (superficial) and the popliteal artery (deep)
- Superficial to the artery, deep to the nerve → middle position in the NVA arrangement
What Joins It?
- Small saphenous vein — enters through the roof of the fossa and drains into the popliteal vein
- This is an important clinical landmark in varicose vein surgery
Clinical Points — Popliteal Vein
Deep Vein Thrombosis (DVT)
- A blood clot in the popliteal vein is a common and serious condition
- Can break off and travel to the lungs → Pulmonary Embolism (PE)
- Risk factors: immobility, surgery, clotting disorders
- Diagnosed by compression ultrasound
- Treated with blood thinners (anticoagulants)
🔁 Quick Summary Table
| Feature | Popliteal Artery | Popliteal Vein |
|---|---|---|
| Origin | Continuation of femoral artery (at adductor hiatus) | Junction of anterior + posterior tibial veins |
| Termination | Divides into anterior & posterior tibial arteries | Becomes the femoral vein |
| Position in fossa | Deepest (next to bone) | Middle (between nerve & artery) |
| Palpable? | Yes, with deep pressure | No (not routinely) |
| Key branches/tributaries | 5 genicular arteries + sural arteries | Small saphenous vein |
| Key clinical issue | Aneurysm, PAES | DVT |
📌 Remember — The "NVA" Rule
From superficial to deep inside the popliteal fossa:
Nerve → Vein → Artery (most superficial) → → → (deepest)
This is clinically important — the artery being deepest protects it but makes direct access challenging.
Sources: Gray's Anatomy for Students, 4th Ed., p. 720–722 | THIEME Atlas of General Anatomy & Musculoskeletal System, p. 585–586
tell me about the clinical importance of popliteal fossa
Finding Sources
Finding Sources
Searching Images
popliteal fossa clinical Baker cyst aneurysm
Reading File
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive clinical material from multiple authoritative sources. Here is the full answer:
Clinical Importance of the Popliteal Fossa
The popliteal fossa is packed with vital neurovascular structures — which makes it an area of great clinical, surgical, and traumatic significance. Problems here can affect blood supply, nerve function, and venous drainage of the entire lower leg and foot.
1. 🦵 Popliteal Masses — "The Big Three"
When a patient has a lump behind the knee, the 3 most common causes are:
| Mass | What It Is |
|---|---|
| Baker's Cyst (Popliteal Cyst) | Fluid-filled synovial sac |
| Popliteal Artery Aneurysm | Dilated popliteal artery |
| Arterial Adventitial Cyst | Cyst within the artery wall |
All three are diagnosed and distinguished using Ultrasound + Doppler.
2. 🫧 Baker's Cyst (Popliteal Cyst)
What it is:
A fluid-filled sac formed when the synovial membrane of the knee joint herniates (bulges out) into the popliteal fossa — typically between the medial head of gastrocnemius and the semimembranosus tendon.
Causes:
- Osteoarthritis
- Rheumatoid arthritis
- Gout
- Knee joint trauma
Symptoms:
- Swelling and tenderness behind the knee
- Worse with walking, jumping (active flexion)
- Can extend into the calf if large
Why it's dangerous:
- Mimics DVT (Deep Vein Thrombosis) — this is called Pseudothrombophlebitis Syndrome
- 2–6% of patients suspected of having DVT actually have a Baker's cyst!
- A Baker's cyst can also compress the tibial nerve → causing pain, weakness, and sensory loss in the foot
How to treat:
- Many resolve on their own
- Ultrasound-guided aspiration + steroid injection
- Surgery if the underlying joint problem is severe

3. 💢 Popliteal Artery Aneurysm
What it is:
Abnormal widening (dilation) of the popliteal artery — classified as aneurysmal when diameter > 7 mm.
Key features:
- Most common peripheral artery aneurysm
- Often bilateral (both legs affected)
- Strongly associated with Abdominal Aortic Aneurysm (AAA) — always check the whole arterial tree!
Why it's unique vs. other aneurysms:
- Unlike aortic aneurysms, popliteal ones rarely rupture
- They tend to form thrombus (clots) inside → clots break off → travel downstream → distal embolization
- This causes lower limb ischemia — in severe cases, amputation
On examination:
- A pulsatile mass behind the knee
- Bruit (whooshing sound) heard with a stethoscope
Diagnosis: Ultrasound + Doppler
Treatment: Surgical excision + graft interposition
4. 🏃 Popliteal Artery Entrapment Syndrome (PAES)
Who gets it: Young, athletic people (especially military recruits)
What happens: An abnormally positioned or hypertrophied muscle (usually the medial head of gastrocnemius) compresses the popliteal artery inside the fossa.
Two types:
- Anatomic — fixed structural abnormality (muscle in wrong position)
- Functional — muscle is hypertrophied and only compresses during activity
Symptoms:
- Calf pain during exercise (intermittent claudication in a young person)
- Cold feet after exercise
- Foot pulse disappears on plantar flexion
If untreated: progresses to arterial degeneration → thromboembolism → tissue death
Diagnosis: CT angiography or MR angiography with active plantar flexion (provocative test)
Treatment: Surgery — resection or re-routing of the compressing muscle
5. 🩸 Popliteal Vein — DVT Risk
Deep Vein Thrombosis (DVT) at the popliteal vein level is serious because:
- Clots at or above the popliteal vein are high-risk for pulmonary embolism (PE)
- Blood clot travels from the popliteal vein → femoral vein → inferior vena cava → lungs
Diagnosis: Compression ultrasound
Treatment: Anticoagulants (blood thinners)
6. 🫀 Varicose Veins Surgery — Risk to Popliteal Fossa
The small saphenous vein enters the popliteal fossa through its roof and joins the popliteal vein. During varicose vein surgery, the surgeon must ligate (tie off) this junction.
Classic surgical danger: The common fibular nerve runs close to the small saphenous vein in the popliteal fossa.
Real case: A surgeon accidentally ligated the common fibular nerve instead of the small saphenous vein — the patient woke up with foot drop (could not lift the foot), wasting of fibular muscles, and sensory loss on the lateral leg and foot.
Lesson: Surgical dissection in the popliteal fossa must be very precise — the NVA arrangement (Nerve → Vein → Artery) makes it easy to confuse structures.
7. ⚡ Nerve Injuries in the Popliteal Fossa
Common Fibular (Peroneal) Nerve Injury
- Most commonly injured nerve in the lower limb
- Lies superficially near the neck of the fibula (lateral border of fossa)
- Injured by: fractures, surgical error, prolonged squatting, tight casts, direct trauma
- Results in: Foot drop (cannot dorsiflex foot), sensory loss on dorsum of foot and lateral leg
Tibial Nerve Injury in the Fossa
- Less common, but caused by:
- Baker's cysts compressing the nerve
- Trauma or hemorrhage in the fossa
- Nerve tumors
- Entrapment by soleus arch or hypertrophied popliteus
- Results in: Weakness of plantar flexion and toe flexion, sensory loss on the sole of the foot
8. 🩻 Cystic Adventitial Disease
A rare but important condition:
- A mucinous (jelly-like) cyst grows inside the wall of the popliteal artery
- Narrows the lumen from within
- Classically affects middle-aged men
- Presents with intermittent claudication
- Diagnosed on MR/CT angiography — treated surgically
9. 🩺 Palpation of the Popliteal Pulse — Clinical Significance
- The popliteal artery is the deepest structure in the fossa → difficult to feel
- Felt by deep bimanual pressure with the knee slightly flexed and patient prone or supine
- Absent or diminished popliteal pulse = peripheral vascular disease or proximal occlusion
- Easily palpable (bounding) pulse = think aneurysm
Quick Summary
| Condition | Structure Affected | Key Feature |
|---|---|---|
| Baker's Cyst | Synovial membrane/bursa | Mimics DVT; compresses tibial nerve |
| Popliteal Artery Aneurysm | Popliteal artery | Pulsatile mass; clots → ischemia |
| PAES | Popliteal artery | Young athlete; pain on plantar flexion |
| DVT | Popliteal vein | High PE risk |
| Varicose vein surgery | Small saphenous / common fibular nerve | Risk of foot drop |
| Tibial nerve injury | Tibial nerve | Weak plantar flexion; sensory loss on sole |
| Common fibular nerve injury | Common fibular nerve | Foot drop; sensory loss dorsum of foot |
| Cystic adventitial disease | Popliteal artery wall | Claudication; middle-aged men |
Sources: Gray's Anatomy for Students, p. 720–722, 782–787 | Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 3725–3729 | Goldman-Cecil Medicine, p. 1082–1097 | Localization in Clinical Neurology, 8e, p. 151
This is a shared conversation. Sign in to Orris to start your own chat.