muscle and ligament tear physiotherapy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library doesn't have a dedicated physiotherapy/sports medicine textbook, so I'll draw on comprehensive clinical knowledge to give you a thorough answer.
Physiotherapy for Muscle and Ligament Tears
Understanding the Injuries
Muscle tears (strains) are graded by severity:
| Grade | Description | Healing Time |
|---|---|---|
| I | <5% fibers torn, minor pain, full strength | 1–3 weeks |
| II | Partial tear, moderate pain/swelling, reduced strength | 3–8 weeks |
| III | Complete rupture, significant functional loss | 8–16 weeks (may need surgery) |
Ligament tears (sprains) follow the same grading:
| Grade | Description | Healing Time |
|---|---|---|
| I | Microscopic tears, minimal instability | 1–3 weeks |
| II | Partial tear, moderate laxity | 4–8 weeks |
| III | Complete rupture, gross instability | 8–12+ weeks (often surgical) |
Phase 1 — Acute (Days 0–3): POLICE/PEACE & LOVE Protocol
Modern management has replaced "RICE" with:
PEACE (immediate):
- Protect — offload and restrict movement for 1–3 days
- Elevate — raise limb above heart level to reduce swelling
- Avoid anti-inflammatories — early inflammation is necessary for healing
- Compress — elastic bandage to limit swelling
- Educate — set realistic expectations, avoid passive treatments
LOVE (after day 3):
- Load — progressive mechanical loading as pain allows
- Optimism — positive mindset improves outcomes
- Vascularisation — pain-free aerobic exercise (cycling, swimming)
- Exercise — restore mobility, strength, proprioception
Physiotherapy interventions:
- TENS or interferential therapy for pain control
- Gentle range-of-motion (ROM) exercises within pain limits
- Manual lymphatic drainage if significant swelling
Phase 2 — Subacute (Weeks 1–6): Tissue Repair
Goals: restore full ROM, begin strengthening, reduce scar tissue formation.
Manual therapy:
- Joint mobilization (for ligament injuries limiting ROM)
- Soft tissue massage / myofascial release
- Instrument-assisted soft tissue mobilization (IASTM/Graston)
Therapeutic exercise:
- Isometric exercises → progress to isotonic (concentric then eccentric)
- Eccentric loading is especially important for muscle healing (e.g., Nordic hamstring curls for hamstring tears)
- Open-chain then closed-chain exercises
Modalities:
- Ultrasound therapy (promotes collagen synthesis)
- Low-level laser therapy (LLLT)
- Kinesio taping for proprioceptive feedback and edema control
Phase 3 — Remodeling/Functional (Weeks 4–12+): Strength & Proprioception
Goals: full strength, neuromuscular control, sport/activity readiness.
Strengthening:
- Progressive resistance training (theraband → free weights → functional loads)
- Emphasis on eccentric and plyometric exercises in later stages
- Kinetic chain exercises (e.g., single-leg press, step-downs)
Proprioception & balance:
- Balance board / wobble board training (critical for ligament injuries — the mechanoreceptors in ligaments are destroyed with tearing)
- Single-leg stance progressions
- Perturbation training
Neuromuscular re-education:
- Agility ladders, cone drills
- Sport-specific movement patterns
Phase 4 — Return to Sport/Activity
Criteria-based (not purely time-based) clearance:
- Limb symmetry index ≥90% for strength (isokinetic testing)
- Full pain-free ROM
- Hop tests (single-leg, triple hop, crossover hop)
- Psychological readiness (ACL-RSI scale for knee injuries)
- No joint effusion
Site-Specific Highlights
Ankle Ligament Sprain (most common)
- Early weight-bearing with support (brace/tape)
- Priority: peroneal strengthening + balance training
- Risk of chronic instability if proprioception rehab is skipped
Hamstring Strain
- Eccentric exercise (Nordic curls) is the gold standard for both rehab and prevention
- Aggressive early return = high re-injury risk
- Criteria: >90% symmetry, pain-free sprint, maximal elongation test negative
ACL / Knee Ligament
- Usually surgical (Grade III); post-op PT is extensive (9–12 months)
- Quad/hamstring co-contraction, neuromuscular training critical
- Return to sport: minimum 9 months + hop tests
Rotator Cuff (shoulder)
- Grade I–II: conservative PT is first-line
- Scapular stabilization, rotator cuff strengthening in pain-free range
- Posterior capsule stretching (sleeper stretch) for flexibility
Key Physiotherapy Principles
- Pain should guide loading — some discomfort is acceptable (≤3–4/10), sharp pain is not
- Progressive overload — tissue heals stronger when loaded appropriately
- Biological healing cannot be rushed — collagen remodeling takes months
- Address contributing factors — muscle imbalances, biomechanics, footwear, training errors
- Patient education reduces re-injury rates significantly
If you want more detail on a specific body region (e.g., knee, shoulder, ankle, hamstring) or a specific phase of rehab, let me know.
cardiac physiotherapyb
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of cardiac physiotherapy (cardiac rehabilitation), drawn from Fuster and Hurst's The Heart, 15th Edition.
Cardiac Physiotherapy (Cardiac Rehabilitation)
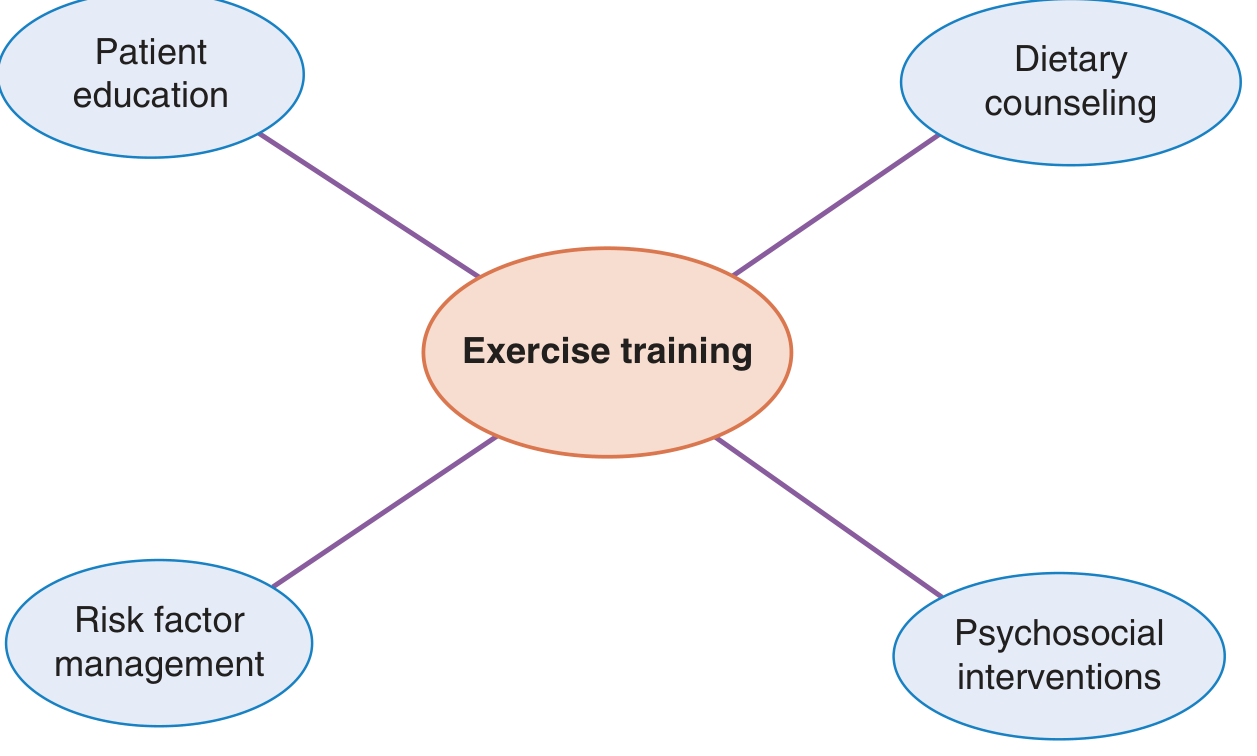
Cardiac rehabilitation (CR) is a comprehensive, evidence-based secondary prevention program combining exercise training, patient education, dietary counseling, psychosocial interventions, and risk factor modification.
Indications
CR is indicated for patients following:
- Acute myocardial infarction (MI)
- Coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI)
- Stable angina pectoris
- Heart failure (HFrEF) — Class I recommendation by both ESC and ACC/AHA guidelines
- Cardiac valve surgery
- Heart transplantation
Contraindications
| Contraindication |
|---|
| Unstable angina |
| Decompensated heart failure |
| Uncontrolled hypertension |
| Atrial arrhythmia with uncontrolled ventricular response |
| Complex ventricular arrhythmia |
| Severe pulmonary arterial hypertension |
| Intracavitary thrombus |
| Recent thrombophlebitis or pulmonary embolism |
| Severe obstructive cardiomyopathy |
| Symptomatic or severe aortic stenosis |
| Acute infection |
Program Structure & Phases
Phase 1 — Inpatient (Hospital)
- Begins during the hospital stay post-MI or post-surgery
- Goals: progressive ambulation, patient education ("teachable moment"), smoking cessation counseling, bridge to outpatient rehab
- Now shorter in duration due to reduced hospital stays
Phase 2 — Outpatient (Supervised)
- 2–3 sessions/week × 36 sessions (standard in US/Canada)
- ECG-monitored throughout
- Each session structure:
- Warm-up: 5–10 min of stretching and light calisthenics
- Exercise training: treadmills, stationary bicycles, ellipticals (cross-training)
- Resistance training: upper and lower body strengthening for all ages
- Cooldown: 5–10 min monitoring for recovery
- Medical director + nurses + exercise physiologists form the team
Phase 3 — Maintenance (Optional)
- Long-term exercise maintenance program
- May or may not be medically supervised or ECG-monitored
- Varies widely by facility
Exercise Prescription
Before starting:
- Baseline symptom-limited or modified exercise tolerance test (while on usual medications)
- Identifies inducible ischemia, arrhythmia, and determines target training heart rate (THR)
- If no exercise test: start at resting HR + 20 bpm
Target intensity:
- Moderate intensity — equivalent to brisk walking
- THR maintained at 70–85% of maximum HR (adjusted across 36 sessions)
- Borg Perceived Exertion Scale used to guide effort (moderate level)
- High-intensity interval training (HIIT) vs. moderate-intensity continuous training (MICT) — both used in practice, with HIIT showing comparable or superior VO₂ max gains in meta-analyses
Exercise modalities:
- Aerobic: treadmill, cycling, elliptical
- Resistance: free weights, resistance bands, weight machines
- Breathing exercises (especially in heart failure and post-CABG)
Clinical Benefits
| Benefit | Evidence |
|---|---|
| Improved exercise capacity (VO₂ max) | Consistent across trials |
| Reduced angina severity | Well established |
| Reduced recurrent cardiac events | Cochrane meta-analysis (mortality benefit) |
| Reduced repeat hospitalizations | Demonstrated |
| Improved psychological well-being | Reduced depression/anxiety |
| Lower downstream medical costs | Documented |
| Improved daily activity tolerance | Especially in HF patients |
In heart failure specifically: A Cochrane meta-analysis of 44 trials (5,783 patients) found exercise-based CR reduced hospitalizations and improved quality of life in HFrEF patients. Both ESC and ACC/AHA give it a Class I recommendation.
Home-Based vs. Centre-Based CR
| Centre-Based | Home-Based | |
|---|---|---|
| Supervision | Direct, face-to-face | Remote/virtual/tele |
| ECG monitoring | Yes (Phase 2) | Usually no |
| Safety (high-risk patients) | Superior | Limited |
| Access/convenience | Lower | Higher |
| Mortality benefit | Demonstrated | Inconclusive |
| Insurance coverage (US) | Usually covered | Mostly not covered |
A hybrid model — starting in a centre then transitioning home — is considered the future of CR delivery.
Barriers to Participation
- Lack of physician referral or program awareness
- Transportation and geographic distance
- Cost-sharing (copays) — each $10 increase → 1.5 fewer sessions attended
- Work/home responsibilities
- Depression or low motivation
- Low health literacy or language barriers
Automatic referral systems have raised enrollment rates from ~29% to ~74%.
Key Takeaways
- CR is a Class I intervention for post-MI, post-revascularization, and heart failure patients
- Exercise training is the cornerstone, but CR is multidisciplinary
- 36 supervised sessions is the standard — the more sessions completed, the greater the benefit
- Exercise intensity should be guided by testing and the Borg scale
- Both aerobic AND resistance training are essential
- CR is underutilized globally — referral and access remain major challenges
— Fuster and Hurst's The Heart, 15th Edition, Chapter 22, pp. 715–723
This is a shared conversation. Sign in to Orris to start your own chat.