Hypoglycemia , defination, causes, pathophysiology , clinical festures, imvestigation, management, diffrential diagnoais and approach as per harrison 22nd edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have comprehensive data from the chapter. Now let me compile the full, detailed response from Harrison's 22nd edition content I've read.
Hypoglycemia - Harrison's Principles of Internal Medicine, 22nd Edition (Chapter 418)
Author: Stephen N. Davis
1. DEFINITION
Hypoglycemia is most commonly caused by insulin or insulin-producing drugs used to treat diabetes mellitus, or by exposure to other drugs including alcohol. It may be documented by Whipple's Triad:
- Symptoms consistent with hypoglycemia
- A low plasma glucose concentration measured with a precise method
- Relief of symptoms after the plasma glucose level is raised
The lower limit of the fasting plasma glucose concentration is normally ~70 mg/dL (~3.9 mmol/L), but lower venous glucose levels occur normally late after a meal, during pregnancy, and during prolonged fasting (>24 hours). Severe hypoglycemia can cause serious morbidity, increase the risk for cardiovascular events, and increase mortality during and after the initial episode. It should be considered in any patient with episodes of confusion, altered consciousness, or seizure.
2. GLUCOSE COUNTERREGULATION (Pathophysiology Basis)
Glucose is an obligate metabolic fuel for the brain. The brain cannot synthesize glucose or store more than a few minutes' supply as glycogen - it requires a continuous arterial supply. Plasma glucose concentrations are normally maintained within 70-110 mg/dL (3.9-6.1 mmol/L) in the fasting state.
Normal Counterregulatory Hierarchy (glucose thresholds in descending order):
| Plasma Glucose | Response |
|---|---|
| ~80 mg/dL (4.4 mmol/L) | Decreased insulin secretion |
| ~65 mg/dL (3.6 mmol/L) | Increased glucagon secretion |
| ~65 mg/dL (3.6 mmol/L) | Increased epinephrine secretion |
| ~55 mg/dL (3.1 mmol/L) | Symptoms (neurogenic + neuroglycopenic) |
| ~50 mg/dL (2.8 mmol/L) | Cognitive impairment |
| <20 mg/dL (<1.1 mmol/L) | Coma, convulsions |
Key counterregulatory hormones:
- Glucagon (first-line, from pancreatic alpha cells) - stimulates glycogenolysis and gluconeogenesis
- Epinephrine (critical when glucagon is deficient) - stimulates hepatic glucose production, limits glucose utilization, and provides warning symptoms
- Cortisol and growth hormone - important for recovery from prolonged hypoglycemia but not rapid acute defense
3. CAUSES (Table 418-1, Harrison's)
A. Ill or Medicated Individuals
1. Drugs (most common overall cause)
- Insulin or insulin secretagogues (sulfonylureas, meglitinides)
- Alcohol - inhibits gluconeogenesis; occurs after binge drinking with inadequate food intake
- Others: quinine, pentamidine, quinolones, indomethacin, beta-blockers (mask symptoms), ACE inhibitors, IGF-1
2. Critical Illness
- Hepatic failure (reduced glycogen stores + impaired gluconeogenesis)
- Renal failure (reduced renal gluconeogenesis + reduced insulin clearance)
- Cardiac failure (hepatic congestion)
- Sepsis (increased peripheral glucose consumption, cytokine-mediated insulin release)
- Inanition (prolonged starvation)
3. Hormone Deficiency
- Cortisol deficiency (Addison's disease, hypopituitarism) - reduces gluconeogenic substrates and limits epinephrine-stimulated glucose production
- Growth hormone deficiency
- Glucagon + epinephrine deficiency (seen in insulin-deficient diabetes)
4. Non-islet Cell Tumors (NICTH)
- Large mesenchymal/epithelial tumors (e.g., fibrosarcoma, hepatocellular carcinoma)
- Cause hypoglycemia via excess secretion of incompletely processed (big) IGF-II, which activates insulin receptors
B. Seemingly Well Individuals
5. Endogenous Hyperinsulinism
- Insulinoma - most common surgically correctable cause; ~90% benign, solitary pancreatic beta-cell tumor
- Functional beta-cell disorders (nesidioblastosis)
- Noninsulinoma pancreatogenous hypoglycemia (NIPHS)
- Post-gastric bypass hypoglycemia (postprandial, typically within 1-3 hours; due to exaggerated GLP-1 response and postprandial hyperinsulinism)
- Insulin autoimmune hypoglycemia - antibodies to insulin or insulin receptor
- Antibody to insulin receptor
- Ectopic insulin secretion (very rare)
6. Inborn Errors of Metabolism (more common in infancy)
- Hyperinsulinism of infancy (mutations in KATP channel genes: ABCC8/KCNJ11)
- Glucokinase-activating mutations
- Fatty acid oxidation defects
- Glycogen storage diseases
- Gluconeogenic enzyme deficiencies
7. Factitious Hypoglycemia
- Surreptitious insulin or sulfonylurea use (healthcare workers, patients with psychiatric disorders)
4. PATHOPHYSIOLOGY
In Diabetic Patients - Hypoglycemia-Associated Autonomic Failure (HAAF)
In insulin-deficient diabetes (T1DM and advanced T2DM), iatrogenic hypoglycemia is the result of the interplay of:
- Relative or absolute therapeutic insulin excess
- Compromised glucose counterregulation
Even marked insulin excess alone can cause hypoglycemia; however, in most cases it results from the combination of hyperinsulinemia with loss of the normal counterregulatory responses.
Why counterregulation fails in diabetes:
- T1DM early: Glucagon response to hypoglycemia is lost (because glucagon secretion is normally suppressed by local insulin from beta cells - which are now absent)
- T1DM long-standing + Advanced T2DM: Both glucagon AND epinephrine responses are impaired
- This creates defective glucose counterregulation - the patient cannot mount adequate defense against falling glucose
HAAF Cycle (shown in flowchart below):
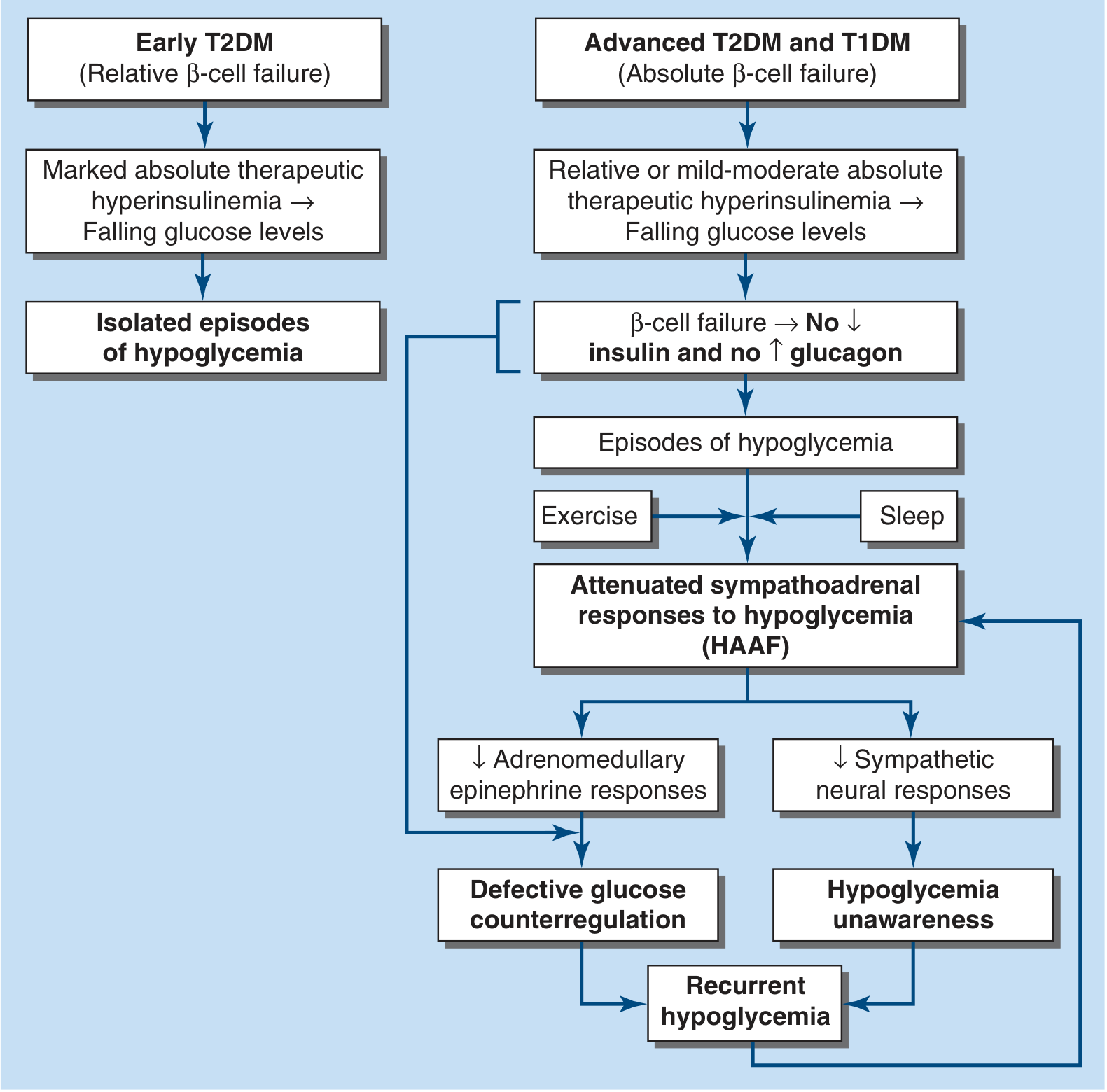
The concept of HAAF posits that recent antecedent iatrogenic hypoglycemia (or sleep or prior exercise) causes:
- Attenuated adrenomedullary epinephrine responses → Defective glucose counterregulation
- Attenuated sympathetic neural responses → Hypoglycemia unawareness
- Both together → Recurrent hypoglycemia - creating a vicious cycle
Hypoglycemia unawareness: Loss of the warning adrenergic symptoms of hypoglycemia. Patients no longer experience palpitations, tremor, or sweating at low glucose levels. This greatly increases the risk of severe hypoglycemia.
5. CLINICAL FEATURES
Symptoms occur in two categories:
A. Neurogenic (Autonomic) Symptoms
Caused by perception of physiologic changes triggered by sympathoadrenal activation (epinephrine release):
- Tremor (adrenergic)
- Palpitations (adrenergic)
- Anxiety (adrenergic)
- Sweating (cholinergic)
- Hunger (cholinergic)
- Paresthesias (cholinergic)
These symptoms typically occur at plasma glucose ~55 mg/dL (3.1 mmol/L) and serve as a warning to the patient.
B. Neuroglycopenic Symptoms
Caused by brain glucose deprivation (insufficient glucose for cerebral metabolism):
- Cognitive impairment / difficulty concentrating
- Confusion / behavioral changes
- Fatigue and weakness
- Seizure
- Loss of consciousness / coma
- Focal neurologic deficits (transient hemiplegia, aphasia - rare)
- At very low levels (<1.1 mmol/L): coma and death
Clinical Note:
- In patients with hypoglycemia unawareness (HAAF), neuroglycopenic symptoms may appear WITHOUT prior neurogenic warning symptoms
- Nocturnal hypoglycemia may be asymptomatic (patient asleep) and present as morning headache, wet sheets, or waking with confusion
6. INVESTIGATIONS
A. Confirming Hypoglycemia (Whipple's Triad)
- Plasma glucose (venous sample by glucose oxidase method - NOT capillary fingerstick alone): confirmed <70 mg/dL during symptoms, with relief on glucose administration
B. Initial Workup (done when Whipple's triad is confirmed or during fasting test)
| Test | Significance |
|---|---|
| Plasma glucose | Confirm low level |
| Insulin (immunoreactive) | Elevated suggests endogenous hyperinsulinism |
| C-peptide | Elevated with endogenous insulin excess; suppressed with exogenous insulin use |
| Proinsulin | Elevated in insulinoma |
| Beta-hydroxybutyrate | Suppressed (<2.7 mmol/L) during hypoglycemia = insulin excess |
| Plasma sulfonylurea screen | Rules out sulfonylurea use (factitious) |
| Cortisol | To rule out adrenal insufficiency |
| IGF-II / IGF-I ratio | Elevated in non-islet cell tumor hypoglycemia (big IGF-II) |
C. The 72-Hour Supervised Fast
The standard diagnostic test for insulinoma/endogenous hyperinsulinism:
- Insulin, C-peptide, proinsulin, beta-hydroxybutyrate, and glucose measured every 6 hours (every 1-2 hours when glucose falls <60 mg/dL)
- Fast is ended when:
- Plasma glucose falls to <45 mg/dL AND patient has symptoms, OR
- After 72 hours without hypoglycemia (essentially excludes insulinoma)
- At the end: give IV glucagon 1 mg - a plasma glucose rise of >25 mg/dL confirms insulin-mediated hypoglycemia
Interpretation criteria (at time of hypoglycemia):
| Insulin (μU/mL) | C-peptide (nmol/L) | Proinsulin (pmol/L) | Sulfonylurea screen | Diagnosis |
|---|---|---|---|---|
| ≥3 | ≥0.2 | ≥5 | Negative | Insulinoma or NIPHS |
| ≥3 | ≥0.2 | ≥5 | Positive | Sulfonylurea use |
| ≥3 | Suppressed | - | Negative | Exogenous insulin (factitious) |
| <3 | <0.2 | <5 | Negative | Non-insulin-mediated |
D. Localization Studies (if endogenous hyperinsulinism confirmed)
- CT/MRI of the pancreas - first-line; 70-80% sensitivity for insulinoma
- Endoscopic ultrasound (EUS) - high sensitivity (80-90%); can detect tumors <1 cm
- Somatostatin receptor scintigraphy (SRS/octreotide scan) - useful for non-beta-cell tumors
- Selective arterial calcium stimulation test (SACST) - intra-arterial calcium injection into feeding arteries with hepatic vein insulin sampling; regionalizes hyperfunctioning tissue
- Intraoperative ultrasound - gold standard for localizing at surgery
E. For Non-Islet Cell Tumors
- Serum IGF-II, IGF-I, and IGFBP-3
- "Big IGF-II" (high molecular weight precursor form) - confirmatory
- Imaging (CT/MRI) for large tumor identification
F. For Post-Gastric Bypass Hypoglycemia
- Mixed meal test (reproduces postprandial symptoms): measure glucose, insulin, C-peptide, and GLP-1 every 30 min for 5 hours
- 72-hour fast typically does NOT induce hypoglycemia (helps distinguish from insulinoma)
7. MANAGEMENT
A. Acute Treatment
Conscious patient (able to swallow):
- 15-20 g fast-acting oral carbohydrate: 4 glucose tablets, 120-180 mL fruit juice, regular soft drink, or glucose gel
- Recheck glucose in 15 minutes; repeat if still <70 mg/dL
- Follow with a snack containing complex carbohydrate + protein once glucose has normalized (prevents recurrence)
Unconscious or unable to swallow:
- IV dextrose: 25 g (50 mL of 50% dextrose) IV push, followed by 5% or 10% dextrose infusion to maintain glucose >100 mg/dL
- Glucagon IM/SC: 1 mg (adult); effective when IV access is unavailable; acts within 10-15 min by stimulating hepatic glycogenolysis
- Less effective in: prolonged fasting/starvation (depleted glycogen stores), alcohol-induced hypoglycemia, adrenal insufficiency
- Nasal glucagon (3 mg) is now approved as an alternative to IM glucagon for home use
Following recovery:
- Identify and treat the underlying cause
- Monitor glucose until the patient is stable and eating
- For long-acting insulin or sulfonylurea-induced hypoglycemia: prolonged dextrose infusion may be needed (sulfonylureas may cause hypoglycemia for 24-48+ hours)
B. Insulinoma Management
- Surgical resection (enucleation or partial pancreatectomy) - curative in ~90% of benign insulinomas
- Diazoxide - inhibits insulin secretion via opening of KATP channels; used preoperatively or for inoperable cases (dose 150-450 mg/day orally)
- Octreotide/lanreotide (somatostatin analogues) - used for metastatic insulinoma and some other causes
- Everolimus and sunitinib - approved for unresectable/metastatic pancreatic NETs (including insulinoma)
C. Non-Islet Cell Tumor Hypoglycemia
- Primary treatment: reduce tumor burden (surgery, embolization, chemotherapy)
- Glucocorticoids (prednisone 30-60 mg/day) and/or growth hormone can alleviate hypoglycemia by increasing glucose production and antagonizing IGF-II effects
- Frequent small meals and continuous nasogastric glucose infusion (palliative)
D. Post-Gastric Bypass Hypoglycemia
- Dietary modification - small, low-carbohydrate meals; avoid rapidly absorbed carbohydrates
- Acarbose (alpha-glucosidase inhibitor) - slows carbohydrate absorption, reduces postprandial glucose/insulin excursions
- Diazoxide or octreotide (if dietary measures fail)
- Calcium channel blockers (verapamil, nifedipine) - reduce insulin secretion
- Reversal of bypass (gastrostomy tube feeding) - in severe, refractory cases
- Partial pancreatectomy is generally NOT recommended (high recurrence)
E. Hypoglycemia in Diabetic Patients - Prevention and Risk Factor Reduction
- Identify and address risk factors: excessive insulin dose, missed/delayed meals, unplanned exercise, alcohol intake, renal/hepatic failure
- Relaxed glycemic targets in patients with HAAF, hypoglycemia unawareness, or comorbidities (HbA1c target ~8%)
- Structured patient education on hypoglycemia recognition and treatment
- Continuous glucose monitoring (CGM) with or without insulin pump (closed-loop systems) - shown to reduce hypoglycemia frequency
- Avoid beta-blockers when possible (mask adrenergic warning symptoms)
- Scrupulous avoidance of antecedent hypoglycemia for 2-3 weeks can restore hypoglycemia awareness in many patients (reversal of HAAF)
F. Adrenal Insufficiency as a Cause
- Hydrocortisone replacement - treats the underlying cause
8. PREVENTION OF RECURRENT HYPOGLYCEMIA
For patients with diabetes:
- Regimen adjustment (reduce insulin dose, change timing, switch to analog insulin)
- Patient education programs
- CGM use
- Strict avoidance of hypoglycemia for 2-3 weeks to restore hypoglycemia awareness
9. DIFFERENTIAL DIAGNOSIS
Conditions mimicking hypoglycemia:
| Condition | Key Distinguishing Features |
|---|---|
| Panic disorder / anxiety | Normal glucose during symptoms; no relief with glucose; psychological history |
| Vasovagal syncope | Prodrome of nausea/pallor; triggered by pain/stress; normal glucose |
| Cardiac arrhythmias | Palpitations/syncope; ECG abnormalities; normal glucose |
| TIA / Stroke | Focal neurologic deficits persist; normal glucose; imaging confirms |
| Epilepsy | EEG abnormalities; glucose normal during seizure |
| Alcohol intoxication | History of alcohol; normal glucose (or distinct overlap) |
| Drug overdose (sedatives) | History; toxicology screen |
| Hyperosmolar states | High glucose; no relief with more glucose |
| Psychogenic hypoglycemia | Symptoms occur only when observed; Whipple's triad not met |
Distinguishing Causes of True Hypoglycemia:
| Feature | Insulinoma | Factitious (insulin) | Factitious (sulfonylurea) | NIPHS | Post-gastric bypass |
|---|---|---|---|---|---|
| Fasting vs. postprandial | Mostly fasting | Fasting | Fasting | Postprandial | Postprandial |
| Insulin level | High | High | High | High | High |
| C-peptide | High | Low | High | High | High |
| Proinsulin | High | Low | Variable | Variable | Variable |
| Sulfonylurea screen | Negative | Negative | Positive | Negative | Negative |
| Insulin antibodies | Negative | May be positive | Negative | Negative | Negative |
| 72-hr fast | Positive | Positive | Positive | Often negative | Negative |
| Mixed meal test | Normal | Normal | Normal | Positive | Positive |
10. DIAGNOSTIC APPROACH (Harrison's Stepwise Approach)
Step 1 - Confirm Whipple's Triad (symptomatic patient + documented low glucose + symptom relief with glucose correction)
Step 2 - Is the patient diabetic?
- Yes → Investigate and correct excess insulin dosing, missed meals, drug interactions, organ failure
- No → Proceed to Step 3
Step 3 - Is the patient ill/hospitalized or seemingly well?
- Ill → Think: critical illness (hepatic/renal/cardiac failure), sepsis, drugs, hormone deficiencies, non-beta-cell tumor. Treat the underlying illness.
- Seemingly well → Proceed to endogenous hyperinsulinism workup
Step 4 - Is there fasting or postprandial hypoglycemia?
- Fasting → Insulinoma, factitious, hormone deficiency, non-islet cell tumor → 72-hour fast with glucose/insulin/C-peptide/proinsulin/beta-hydroxybutyrate
- Postprandial → Post-gastric surgery hypoglycemia, NIPHS, reactive hypoglycemia → Mixed meal test
Step 5 - Interpret 72-hour fast results (see Investigation table above)
Step 6 - Localizing studies if endogenous hyperinsulinism confirmed: CT/MRI pancreas → EUS → SACST
Step 7 - Definitive treatment based on etiology
Key Points from Harrison's 22E (Chapter 418):
- Whipple's triad must be documented before extensive workup
- The 72-hour fast remains the gold standard for insulinoma diagnosis
- C-peptide is the key test to distinguish exogenous insulin injection (factitious) from endogenous causes
- HAAF and hypoglycemia unawareness create a dangerous vicious cycle - address by relaxing glycemic targets and avoiding antecedent hypoglycemia
- Glucagon IM is critical first-aid for severe hypoglycemia when IV access is unavailable
- Post-gastric bypass hypoglycemia is increasingly recognized and responds to dietary modification before pharmacologic intervention
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill) - Chapter 418: Hypoglycemia, Stephen N. Davis
This is a shared conversation. Sign in to Orris to start your own chat.