Femur head fracture dislocation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile this.
Femoral Head Fracture-Dislocation
Femoral head fractures almost always occur in the context of hip dislocation — the femoral head shears against the acetabular rim as it dislocates. These are high-energy injuries with a high rate of systemic and musculoskeletal associated injuries.
Mechanism & Epidemiology
- High-energy axial load to the hip (motor vehicle collisions, falls from height)
- Position of the hip at moment of impact determines dislocation direction
- Posterior dislocation is far more common — 9:1 ratio over anterior
- Posterior dislocation → leg flexed, adducted, internally rotated
- Anterior dislocation → leg extended, abducted, externally rotated
- 93% rate of MRI abnormalities at the ipsilateral knee; 30% rate of meniscal tear
- Associated sciatic nerve injury in up to 20% of posterior dislocations (peroneal division most often)
Classification
Pipkin Classification (most widely used)
The Pipkin system classifies femoral head fractures associated with posterior hip dislocation:
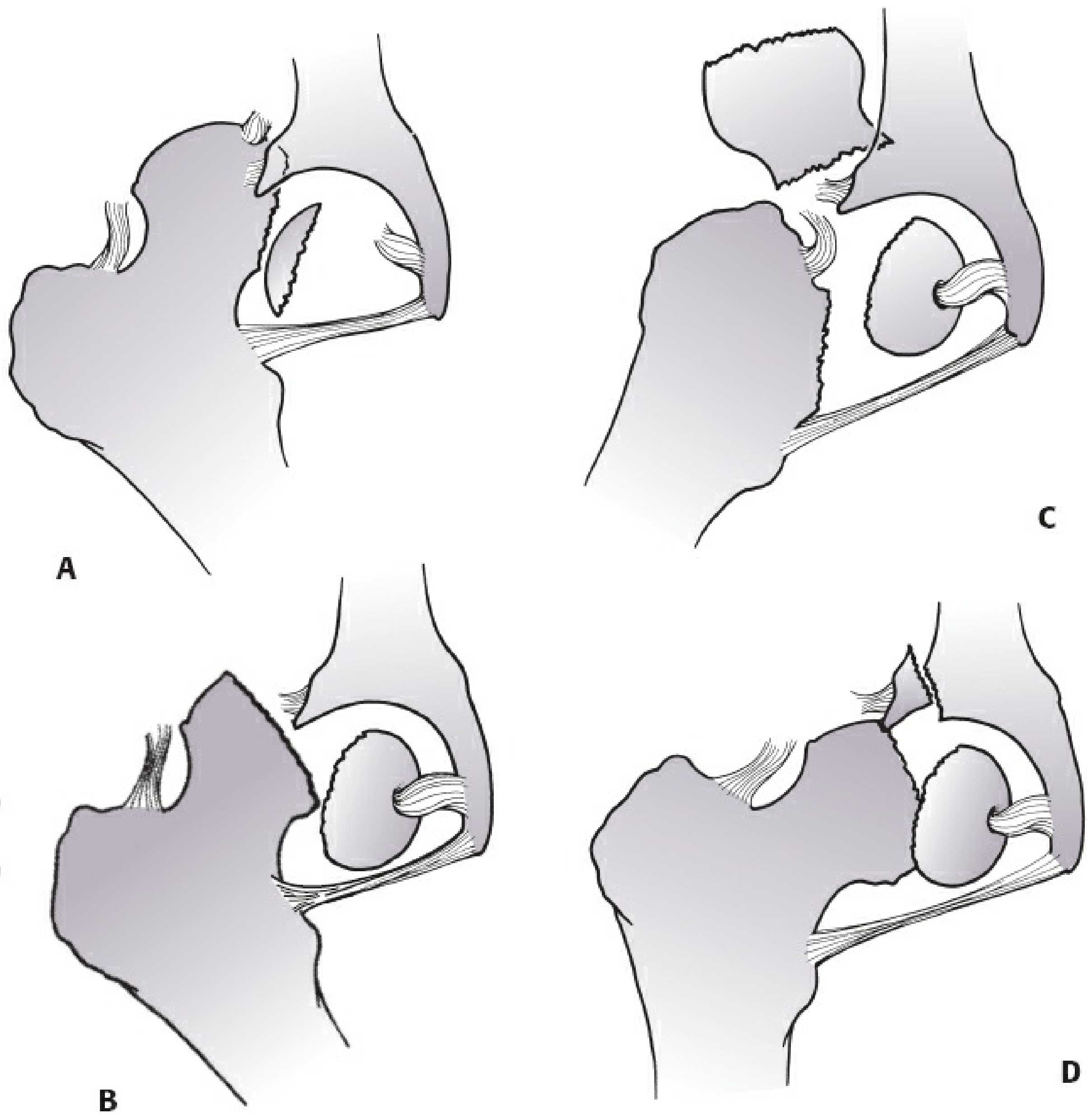
| Type | Description |
|---|---|
| I | Posterior dislocation + femoral head fracture caudad (below) the fovea — non-weight-bearing portion |
| II | Posterior dislocation + femoral head fracture cephalad (above) the fovea — weight-bearing surface |
| III | Femoral head fracture + associated femoral neck fracture — worst AVN risk |
| IV | Type I, II, or III + associated acetabular fracture |
Thompson & Epstein Classification (posterior dislocations)
| Type | Description |
|---|---|
| I | Dislocation with or without minor fracture |
| II | Dislocation + single large posterior rim acetabular fracture |
| III | Dislocation + comminuted rim fracture |
| IV | Dislocation + acetabular floor fracture |
| V | Dislocation + femoral head fracture |
Stewart & Milford Classification
| Type | Description |
|---|---|
| I | Simple dislocation, no fracture |
| II | Dislocation + rim fragment(s), socket still stable |
| III | Dislocation + rim fracture causing gross instability |
| IV | Dislocation + fracture of head or neck of femur |
Brumback Classification
A unified system for both anterior and posterior dislocations that additionally incorporates size of the head fragment and post-reduction hip stability.
Imaging
- AP and lateral hip radiographs — initial evaluation
- CT after reduction — mandatory to evaluate:
- Location and size of femoral head fragment
- Associated acetabular fracture
- Intra-articular loose bodies
- MRI — for osteonecrosis surveillance or occult injuries
Treatment
Emergent Step: Closed Reduction
- Urgent closed reduction is the first priority — the goal is minimizing femoral head ischemia
- AVN rate: 2–10% if reduced within 6 hours
- AVN rate >50% if reduction delayed beyond 12 hours
- Post-reduction: re-evaluate stability, obtain AP pelvis + Judet views + CT
Nonoperative Treatment
- Pipkin Type I — small fragment, congruent joint OR nondisplaced larger fragment → protected weight bearing 4–6 weeks; serial radiographs weekly × 3–4 weeks
- Pipkin Type II — nondisplaced; observe with frequent radiographs to rule out secondary displacement
Operative Treatment
Indications:
-
1 mm articular step-off (except small Pipkin type I)
- Associated loose bodies in joint
- Incongruent reduction
- Associated femoral neck or acetabular fracture requiring fixation
Techniques:
| Scenario | Approach |
|---|---|
| Pipkin I/II, no posterior wall fracture | Anterior (Smith-Petersen) — direct visualization of anterior fragment |
| Pipkin I with small fragment | Excision preferred if causing impingement |
| Pipkin II with displaced large fragment | ORIF with headless countersunk lag screws |
| Pipkin III or IV | Surgical hip dislocation — allows complete visualization |
| Older patient with severe injury | Hip arthroplasty |
Complications
| Complication | Notes |
|---|---|
| Osteonecrosis (AVN) | Up to 15% overall; highest in Pipkin III; directly related to time to reduction and degree of displacement |
| Post-traumatic arthritis | Less common when associated with posterior wall acetabular fracture |
| Sciatic nerve injury | Up to 20% with posterior dislocation; peroneal division most affected |
| Recurrent dislocation | Rare |
| Non-union / malunion | With femoral neck component (Pipkin III) |
Almost all cases of AVN appear within 2 years of injury.
— Rockwood and Green's Fractures in Adults, 10th ed. 2025, pp. 2574–2577, 2621
— Miller's Review of Orthopaedics, 9th Edition, pp. 919–920
This is a shared conversation. Sign in to Orris to start your own chat.