Everything about drye eye disease
Reading File
Finding Sources
Searching PubMed
"dry eye disease" AND management
Searching the Web
dry eye disease pathophysiology diagnosis treatment 2025
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Dry Eye Disease (Keratoconjunctivitis Sicca) - A Complete Overview
Definition
Dry eye disease (DED) is a multifactorial disease of the ocular surface and tear film accompanied by increased osmolarity of the tear film and inflammation of the ocular surface. It results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface. - Kanski's Clinical Ophthalmology, 10th ed.
Related terminology:
- Keratoconjunctivitis sicca (KCS) - any eye with some degree of dryness
- Xerophthalmia - dry eye specifically associated with vitamin A deficiency
- Xerosis - extreme ocular dryness with keratinization from severe conjunctival cicatrization
- Sjögren syndrome - autoimmune inflammatory disease of which dry eye is a key feature
Tear Film Anatomy and Physiology
The tear film has three layers, each secreted by distinct glands:
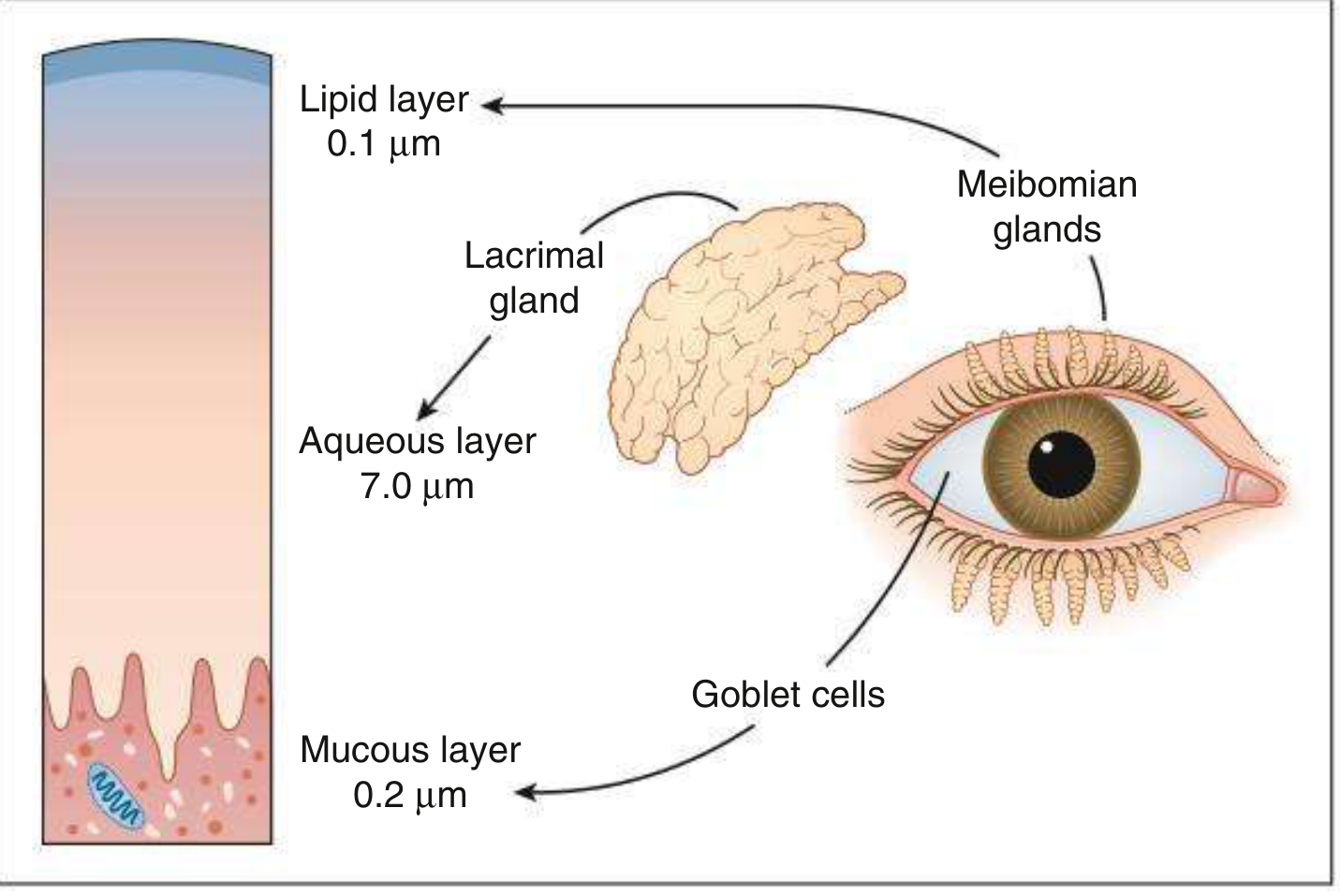
| Layer | Thickness | Source | Function |
|---|---|---|---|
| Lipid | ~0.1 µm | Meibomian glands | Prevents aqueous evaporation; acts as surfactant |
| Aqueous | ~7.0 µm | Lacrimal glands | Oxygen supply, antimicrobial proteins, lubrication |
| Mucous | ~0.2 µm | Conjunctival goblet cells | Wets hydrophobic corneal epithelium; anchors tear film |
The tear film contains as many as 100 distinct proteins. Effective resurfacing after each blink requires a normal blink reflex, contact between eyelid and ocular surface, and normal corneal epithelium.
Hormonal regulation:
- Androgens are the prime hormones regulating lipid production by meibomian glands
- Estrogen and progesterone receptors in the conjunctiva and lacrimal glands are essential for normal function
- Neural fibers adjacent to lacrimal glands and goblet cells stimulate aqueous and mucus secretion
Epidemiology
- Extremely common - affects millions worldwide
- Particularly prevalent in postmenopausal women and the elderly
- A 2025 systematic review found a significant prevalence even among children (PMID: 39971589)
- Strong association with reduced systemic androsterone sulphate and epiandrosterone sulphate
- Dyslipidemia is an independent risk factor for DED (PMID: 37989379)
Pathophysiology
The four core, inter-related mechanisms behind dry eye disease are:
- Tear instability - film breaks up before the next blink, exposing the ocular surface
- Tear hyperosmolarity - triggers inflammatory cascades on the epithelium
- Inflammation - present in ~80% of KCS patients; both a cause and consequence of dry eye. Involves T-cell mediated damage to lacrimal glands and conjunctival goblet cells
- Ocular surface damage - loss of goblet cells, epithelial metaplasia, squamous metaplasia in severe cases
Whether a patient has primary aqueous deficiency or evaporative dry eye, the end result is ocular surface inflammation and discomfort (Kanski's). This inflammatory cycle perpetuates and amplifies disease - the rationale for anti-inflammatory therapies.
Elevated matrix metalloproteinase-9 (MMP-9) in tears contributes to epithelial damage and is a useful diagnostic biomarker.
Classification (DEWS 2007 Framework)
1. Aqueous-Deficient Dry Eye
Sjögren syndrome (SS):
- Autoimmune lymphocytic destruction of lacrimal and salivary glands
- Classic triad: dry eyes + dry mouth + parotid enlargement
- Primary SS (isolated) or secondary SS (with RA, SLE)
- Diagnosed by ACR criteria: anti-SSA/anti-SSB antibodies, ocular surface staining, focal lymphocytic sialadenitis on biopsy
Non-Sjögren aqueous deficiency:
- Lacrimal gland insufficiency: age-related, congenital alacrima, familial dysautonomia, inflammatory/neoplastic infiltration, AIDS, graft-versus-host disease
- Lacrimal gland duct obstruction: trachoma, cicatricial pemphigoid, chemical injury, Stevens-Johnson syndrome
- Reflex hyposecretion: contact lens wear, diabetes, refractive surgery, neurotrophic keratitis (sensory block); 7th CN damage or systemic anticholinergic drugs (motor block)
2. Evaporative Dry Eye
Intrinsic causes (lid/gland disease):
- Meibomian gland dysfunction (MGD) - most common cause overall; associated with posterior blepharitis, rosacea
- Disorders of lid aperture: excessive scleral show, lid retraction, proptosis, facial nerve palsy
- Low blink rate: Parkinson's disease, prolonged computer/screen use, reading
- Drug effects: antihistamines, beta-blockers, antispasmodics, diuretics
Extrinsic causes:
- Vitamin A deficiency
- Topical drugs including preservative toxicity
- Contact lens wear
- Ocular surface disease (allergic conjunctivitis)
Environmental/lifestyle factors:
- Arid climate, allergen exposure, smoking
- Air conditioning, central heating, wind, low humidity
- Extended computer work (reduced blink rate)
Most patients have significant overlap between evaporative and aqueous-deficient mechanisms.
Symptoms
- Burning, dryness, foreign body sensation (grittiness)
- Mildly to moderately decreased or blurred vision
- Excess or paradoxical tearing (reflex lacrimation)
- Stringy mucous discharge; lid crusting
- Redness, photophobia
Key patterns:
- Evaporative (MGD): worse in the morning (symptoms upon waking)
- Aqueous-deficient: worse later in the day after extended eye use
- Exacerbated by smoke, wind, heat, low humidity, prolonged screen use
- Usually bilateral, chronic; "discomfort often out of proportion to clinical signs"
Signs
Critical Signs
- Scanty or irregular tear meniscus at inferior lid margin (normal: ≥0.5 mm height, convex shape)
- Decreased tear break-up time (TBUT) < 10 seconds (measured from blink to appearance of first dry spot with fluorescein stain)
Other Signs
- Punctate epithelial erosions (PEE): fluorescein, rose bengal, or lissamine green staining of cornea and conjunctiva - typically inferior or interpalpebral
- Posterior blepharitis with meibomian gland dysfunction
- Filamentary keratitis: mucus-debris strands attached at one end to corneal surface (stain with rose bengal)
- Mucous plaques: semi-transparent white-to-grey elevated lesions in severe cases
- Excess mucus and debris in tear film
Severe/Sight-threatening complications:
- Epithelial breakdown and persistent epithelial defects
- Corneal melting (keratolysis)
- Corneal perforation
- Bacterial superinfection / keratitis
Investigations / Diagnosis
No single test is definitive; a battery of tests improves diagnostic accuracy. Correlation between symptoms and objective signs is often poor but improves with severity.
| Test | Method | Normal / Abnormal Threshold |
|---|---|---|
| Tear break-up time (TBUT) | Fluorescein instilled; time from blink to first dry spot | Normal: >10 s; Abnormal: <10 s |
| Schirmer's test (unanesthetized) | Filter paper in inferior fornix x5 min | Normal: ≥15 mm wetting |
| Schirmer's test (anesthetized) | Same with topical anesthetic (measures basal secretion only) | Abnormal: ≤5 mm; borderline: <10 mm |
| Tear meniscus height | Slit lamp | Normal: ≥0.5 mm; convex |
| Tear osmolarity | TearLab device | Elevated (>308 mOsm/L) confirms DED; useful for monitoring treatment response |
| MMP-9 (InflammaDry) | Immunoassay of inferior fornix secretion | Elevated suggests inflammation/DED |
| Ocular surface staining | Fluorescein/rose bengal/lissamine green | Interpalpebral or inferior staining |
| Tear lactoferrin | Immunoassay | Low levels indicate aqueous-deficient DED |
| Sjögren workup | Anti-SSA, anti-SSB, RF, ANA, salivary gland biopsy | If systemic features present |
TIP: Tear film osmolarity is the most accurate single marker - useful to confirm diagnosis and monitor treatment response. (Kanski's)
Treatment
Treatment is stepped up based on severity. Always treat contributing conditions (blepharitis, exposure keratopathy) alongside dry eye itself.
Mild Dry Eye
- Artificial tears 4x/day, preferably preservative-free
Moderate Dry Eye
- Increase artificial tear frequency up to every 1-2 hours; use only preservative-free preparations (preservative toxicity occurs with dosing >4x/day)
- Lubricating gel or ointment at bedtime
- Lifestyle modification: humidifiers, smoking cessation, reduce screen time, 20-20-20 rule
- Cyclosporine 0.05% or 0.09% drops twice daily - effective for chronic dry eye with ocular inflammation; reduces inflammatory markers, increases tear production. Takes 1-3 months for significant improvement; burning on instillation is common for initial weeks. A brief concurrent mild topical steroid (loteprednol 0.5%, fluorometholone 0.1%) b.i.d.-q.i.d. for 1 month can hasten improvement and reduce side effects
- Lifitegrast 5% (Xiidra) drops twice daily - inhibits LFA-1/ICAM-1 interaction to reduce T-cell-mediated inflammation; symptomatic improvement often within 2 weeks (vs. 1-3 months for cyclosporine). Side effects: burning, transient blurred vision, metallic taste
- Punctal occlusion (if above measures inadequate): collagen inserts (temporary), silicone/acrylic plugs (reversible). Treat blepharitis before placing plugs. A 2024 systematic review confirmed punctal cautery is effective for refractory DED (PMID: 39127391)
Severe Dry Eye
- Cyclosporine 0.05%/0.09% or lifitegrast 5% (as above)
- Punctal occlusion (lower and upper puncta); consider permanent thermal cautery if plugs repeatedly dislodge
- Lubricating gel/ointment 2-4x/day as needed
- Moisture chambers (plastic film sealed at orbital rim) or protective glasses/goggles
- 10% acetylcysteine q.i.d. to dissolve mucus strands/filaments (mucolytic)
- Additional options:
- Oral omega-3 fatty acids / flaxseed oil
- Autologous serum tears (contains growth factors, proteins, lipids - superior to manufactured tears; formulated from patient's own blood)
- Topical vitamin A
- Bandage soft contact lens or scleral lens
- Hydroxypropyl cellulose ophthalmic insert (dissolves during the day in inferior cul-de-sac)
- Lateral tarsorrhaphy (surgical partial lid closure) if all else fails
Special Situations
- Blepharitis/MGD: Lid hygiene (warm compresses, lid scrubs); doxycycline for its anti-MMP activity
- Sjögren syndrome: Systemic immunosuppression; oral pilocarpine (salivary/lacrimal stimulant); rituximab in severe cases
- Vitamin A deficiency: Systemic vitamin A replacement
- Lubricating ointments (petrolatum/mineral oil base): reserved for bedtime, critically ill patients, or very severe DED because they cause significant blurred vision
- Topical short-term corticosteroids: useful to break the inflammatory cycle, particularly as a bridge when initiating cyclosporine
Differential Diagnosis
- Superficial punctate keratopathy (from other causes)
- Allergic conjunctivitis
- Blepharitis alone
- Contact lens-related discomfort
- Conjunctival scarring disorders (OCP, SJS)
- Neurotrophic keratitis
Follow-Up
- Mild cases: weeks to months
- Moderate-severe cases: more frequent monitoring
- Severe cases with underlying systemic disease (Sjögren, RA, sarcoidosis, ocular pemphigoid): close, ongoing monitoring by ophthalmology and rheumatology
Emerging Therapies (2025-2026)
The landscape of DED treatment is evolving rapidly. Current pipeline agents include:
- Reproxalap (Aldeyra) - RASP inhibitor targeting inflammation; Phase III data showed significant reduction in ocular discomfort (May 2025), though FDA issued a CRL in April 2025 for insufficient prior evidence
- AZR-MD-001 - targeting meibomian gland dysfunction; Phase III ASTRO trial ongoing
- Agents targeting neuroregeneration, epithelial repair, and lipid regulation in meibomian glands
- Topical insulin showing promise for persistent epithelial defects and ocular surface disorders (PMID: 40381039)
- Biomarker-guided personalized treatment strategies are increasingly being studied
Sources: Kanski's Clinical Ophthalmology, 10th ed. | The Wills Eye Manual | Goodman & Gilman's Pharmacological Basis of Therapeutics | Firestein & Kelley's Textbook of Rheumatology | Recent PubMed systematic reviews (2023-2025)
This is a shared conversation. Sign in to Orris to start your own chat.