Superior and inferior extremity anatomy topic
Reading File
Asking for Preferences
Superior and inferior extremity anatomy topic
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive content for a thorough response. Let me compile the complete anatomy overview.
Superior (Upper) & Inferior (Lower) Extremity Anatomy
Source: Gray's Anatomy for Students
SUPERIOR EXTREMITY - Upper Limb
Overview & Gateway
The upper limb connects to the trunk through the axillary inlet on each side of the superior thoracic aperture. This triangular inlet is bounded by:
- The superior margin of the scapula (posteriorly)
- The clavicle (anteriorly)
- The lateral margin of rib I (medially)
All major structures (arteries, veins, nerves) pass over rib I and through the axilla to enter or leave the upper limb.
Bones & Joints
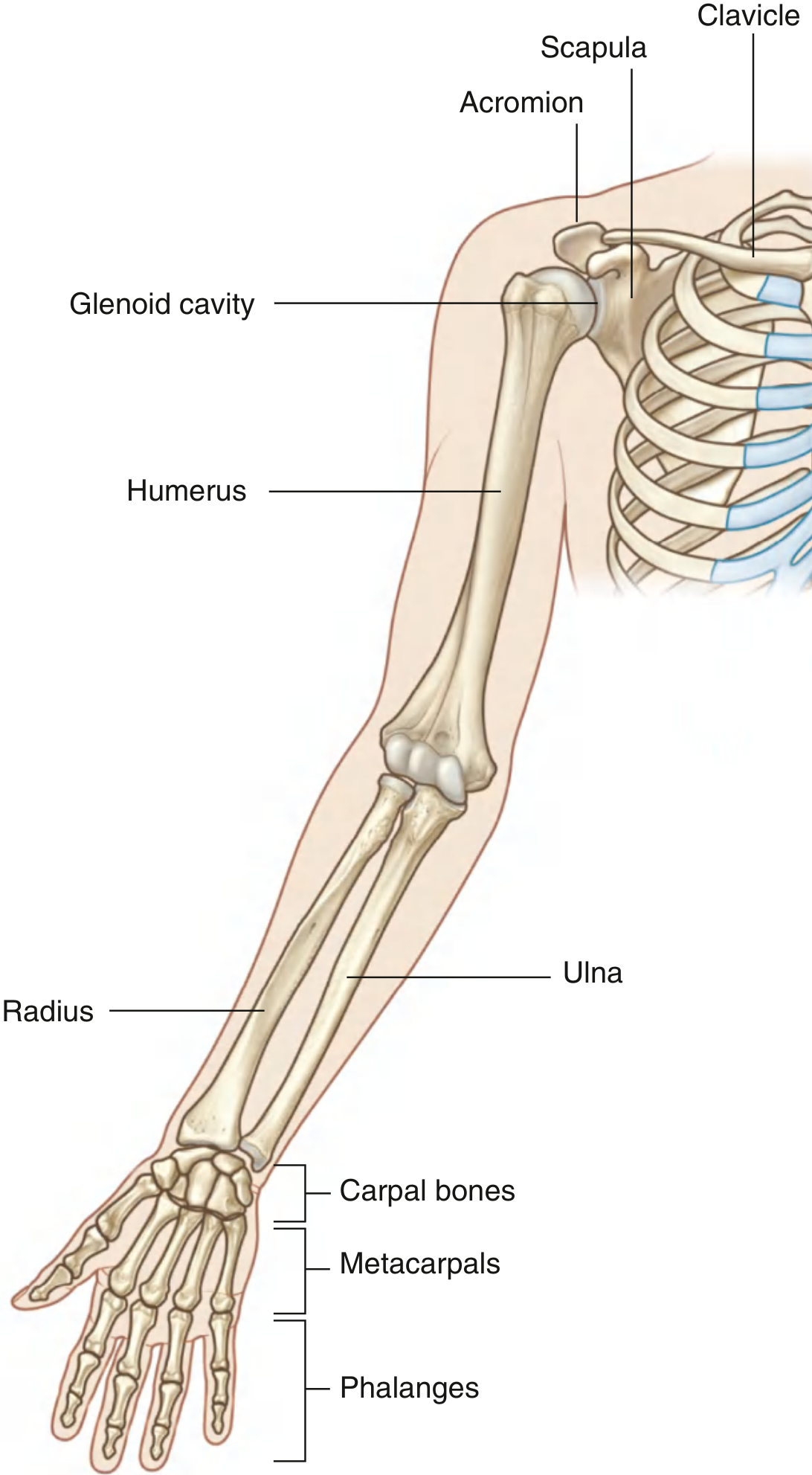
Fig. 7.7 - Bones of the Upper Limb (Gray's Anatomy for Students)
| Region | Bones | Key Joint |
|---|---|---|
| Shoulder girdle | Clavicle + Scapula | Acromioclavicular + Sternoclavicular |
| Arm | Humerus | Glenohumeral (ball & socket) |
| Forearm | Radius (lateral) + Ulna (medial) | Elbow (hinge) + Radioulnar |
| Wrist | 8 Carpal bones | Radiocarpal joint |
| Hand | 5 Metacarpals + Phalanges | MCP (condylar) + IP (hinge) |
- The thumb has 2 phalanges; digits II-V have 3 each
- The saddle joint of the thumb (carpometacarpal I) provides the greatest mobility of any digit
- The clavicle articulates medially with the manubrium and laterally with the acromion of the scapula
Movements
- Glenohumeral joint: flexion, extension, abduction, adduction, medial/lateral rotation, circumduction
- Elbow: flexion and extension
- Forearm: pronation (radius crosses over ulna) and supination (returns to anatomical position)
- Wrist: flexion, extension, abduction (radial deviation), adduction (ulnar deviation), circumduction
- MCP joints: flexion, extension, abduction, adduction, circumduction
- IP joints: flexion and extension only (hinge)
Muscles
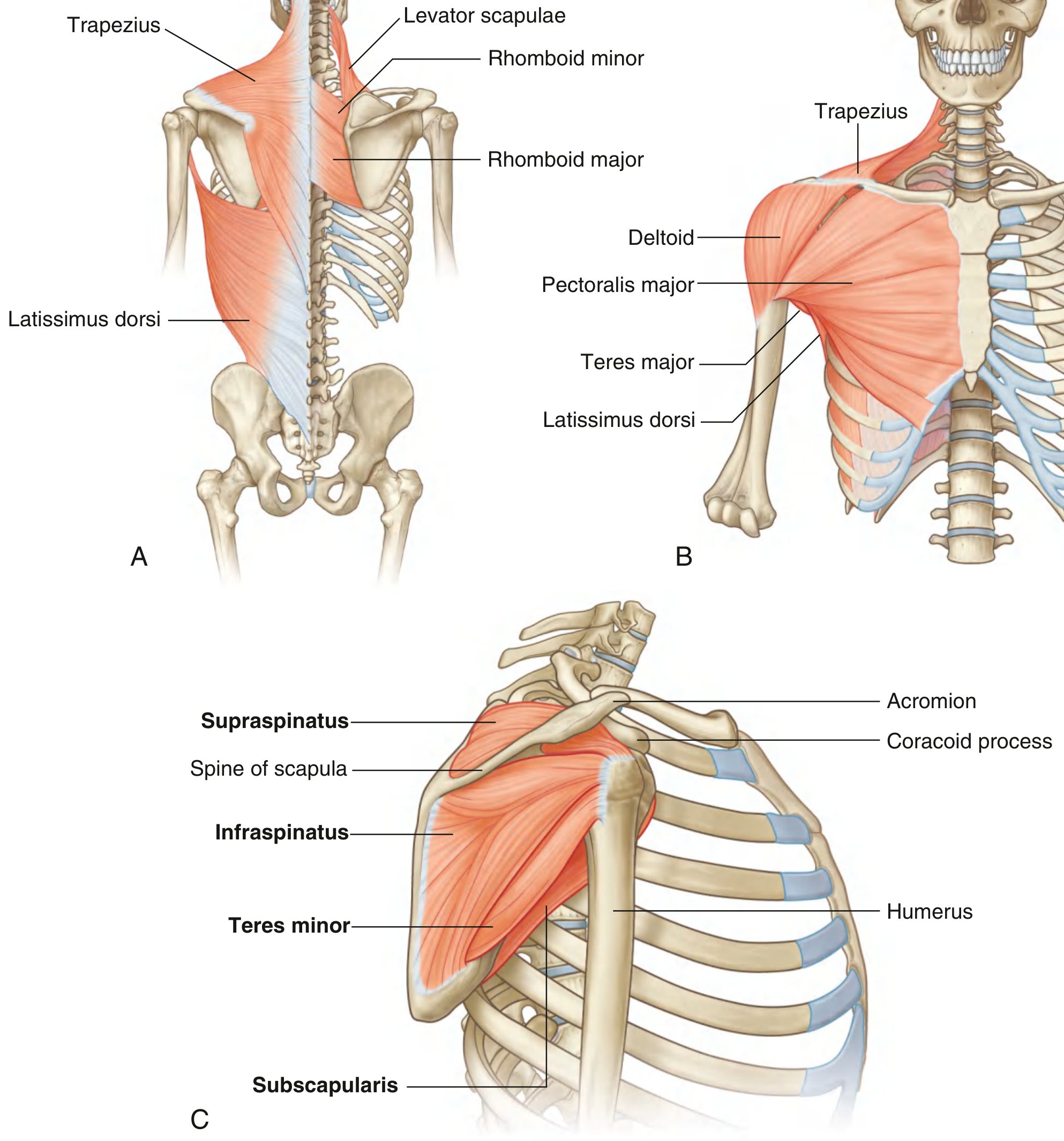
Fig. 7.9 - Shoulder Muscles & Rotator Cuff (Gray's Anatomy for Students)
Shoulder muscles connecting scapula/clavicle to trunk:
- Posterior: trapezius, levator scapulae, rhomboids, latissimus dorsi
- Anterior: pectoralis major, deltoid, teres major
Rotator Cuff (SITS): the 4 muscles stabilizing the glenohumeral joint:
- Supraspinatus - abduction (initiates)
- Infraspinatus - lateral rotation
- Teres minor - lateral rotation
- Subscapularis - medial rotation
Arm compartments:
- Anterior (flexor): biceps brachii, brachialis, coracobrachialis
- Posterior (extensor): triceps brachii
Forearm compartments:
- Anterior: flexors of wrist and fingers + pronators
- Posterior: extensors of wrist and fingers + supinator
Hand muscles (intrinsics): thenar eminence (thumb), hypothenar eminence (little finger), lumbricals, interossei - modify long tendon actions and enable precision grip
Nerves - Brachial Plexus (C5-T1)
The brachial plexus (anterior rami of C5 to C8 and T1) forms in the neck and passes through the axillary inlet. Major terminal branches:
| Nerve | Roots | Primary Motor Supply | Sensory Area |
|---|---|---|---|
| Musculocutaneous | C5-C7 | Anterior arm (biceps, brachialis) | Lateral forearm |
| Median | C6-T1 | Anterior forearm, thenar muscles | Lateral 3.5 fingers (palm) |
| Ulnar | C8-T1 | Intrinsic hand muscles | Medial 1.5 fingers |
| Radial | C5-T1 | Posterior arm & forearm (extensors) | Posterior arm/forearm, dorsal hand |
| Axillary | C5-C6 | Deltoid, teres minor | Lateral shoulder ("regimental badge") |
Clinically relevant - nerves near bone:
- Radial nerve spirals around the posterior humerus (radial/spiral groove) - at risk with mid-shaft humeral fractures
- Ulnar nerve passes posterior to the medial epicondyle - "funny bone"
- Median nerve passes through the carpal tunnel - compressed in carpal tunnel syndrome
Blood Supply
- Subclavian artery → passes over rib I → becomes the axillary artery → becomes the brachial artery in the arm
- Brachial artery divides at the cubital fossa into the radial artery (lateral) and ulnar artery (medial)
- These form the palmar arches in the hand (superficial + deep)
- Key branches: posterior circumflex humeral (from 3rd part of axillary; travels with axillary nerve through quadrangular space), subscapular artery (largest branch of axillary)
INFERIOR EXTREMITY - Lower Limb
Overview & Gateway
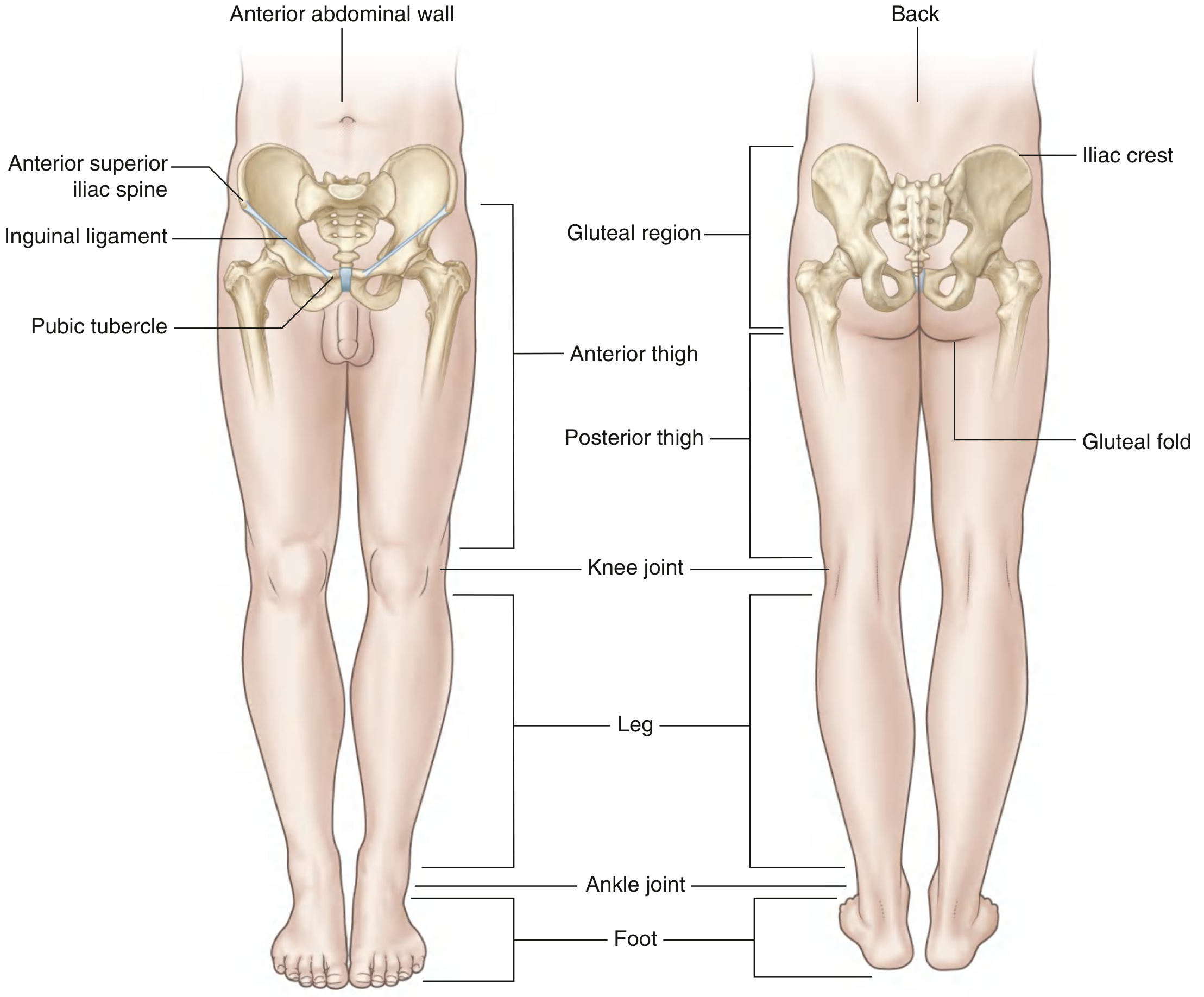
Fig. 6.2 - Regions of the Lower Limb (Gray's Anatomy for Students)
The lower limb communicates with the abdomen through the inguinal aperture (below the inguinal ligament). As vessels cross this boundary, the external iliac artery and vein become the femoral artery and vein.
The lower limb is divided into 4 regions:
- Gluteal region - posterolateral, iliac crest to gluteal fold
- Thigh - hip joint to knee joint
- Leg - knee to ankle
- Foot - distal to ankle joint
Key areas of transition:
- Femoral triangle (proximal thigh) - entry point for femoral nerve, artery, and vein
- Popliteal fossa (posterior knee) - diamond-shaped passage for vessels and nerves
- Tarsal tunnel (posteromedial ankle) - passage for flexor tendons, tibial nerve, and vessels from leg to foot
Bones & Joints
| Region | Bones | Key Joint |
|---|---|---|
| Hip girdle | Os coxae (ilium + ischium + pubis) | Sacroiliac joint |
| Thigh | Femur | Hip joint (ball & socket) + Knee (hinge) |
| Leg | Tibia (medial) + Fibula (lateral) | Ankle joint (mortise) |
| Foot | 7 Tarsal + 5 Metatarsals + Phalanges | Subtalar, MTP, IP joints |
- The hip joint lies just inferior to the middle third of the inguinal ligament
- The knee is the largest joint - stabilized by ACL, PCL, MCL, LCL, and menisci
- The patella is the largest sesamoid bone in the body
- The tarsals include the calcaneus (heel), talus, navicular, cuboid, and 3 cuneiforms
Function: Weight Bearing
When standing erect, the center of gravity falls slightly posterior to the hip joints and anterior to the knee and ankle joints - this arrangement allows the hip and knee to remain in passive extension with minimal muscle effort. The arrangement of ligaments at the hip and knee supports this passive "locked" position.
Muscles by Compartment
| Compartment | Key Muscles | Primary Action |
|---|---|---|
| Gluteal region | Gluteus maximus, medius, minimus | Extension & abduction of hip |
| Anterior thigh | Quadriceps femoris (4 heads), iliopsoas, sartorius | Knee extension; hip flexion |
| Medial thigh | Adductors (magnus, longus, brevis), gracilis | Hip adduction |
| Posterior thigh (hamstrings) | Biceps femoris, semimembranosus, semitendinosus | Hip extension, knee flexion |
| Anterior leg | Tibialis anterior, extensor digitorum longus, extensor hallucis longus | Dorsiflexion + toe extension |
| Lateral leg | Fibularis (peroneus) longus & brevis | Eversion of foot |
| Posterior leg | Gastrocnemius, soleus, flexor hallucis longus, flexor digitorum longus | Plantarflexion; toe flexion |
| Sole of foot | Plantar muscles (4 layers) | Toe movements + arch support |
Nerves - Lumbar (L1-L4) & Sacral Plexus (L4-S3)
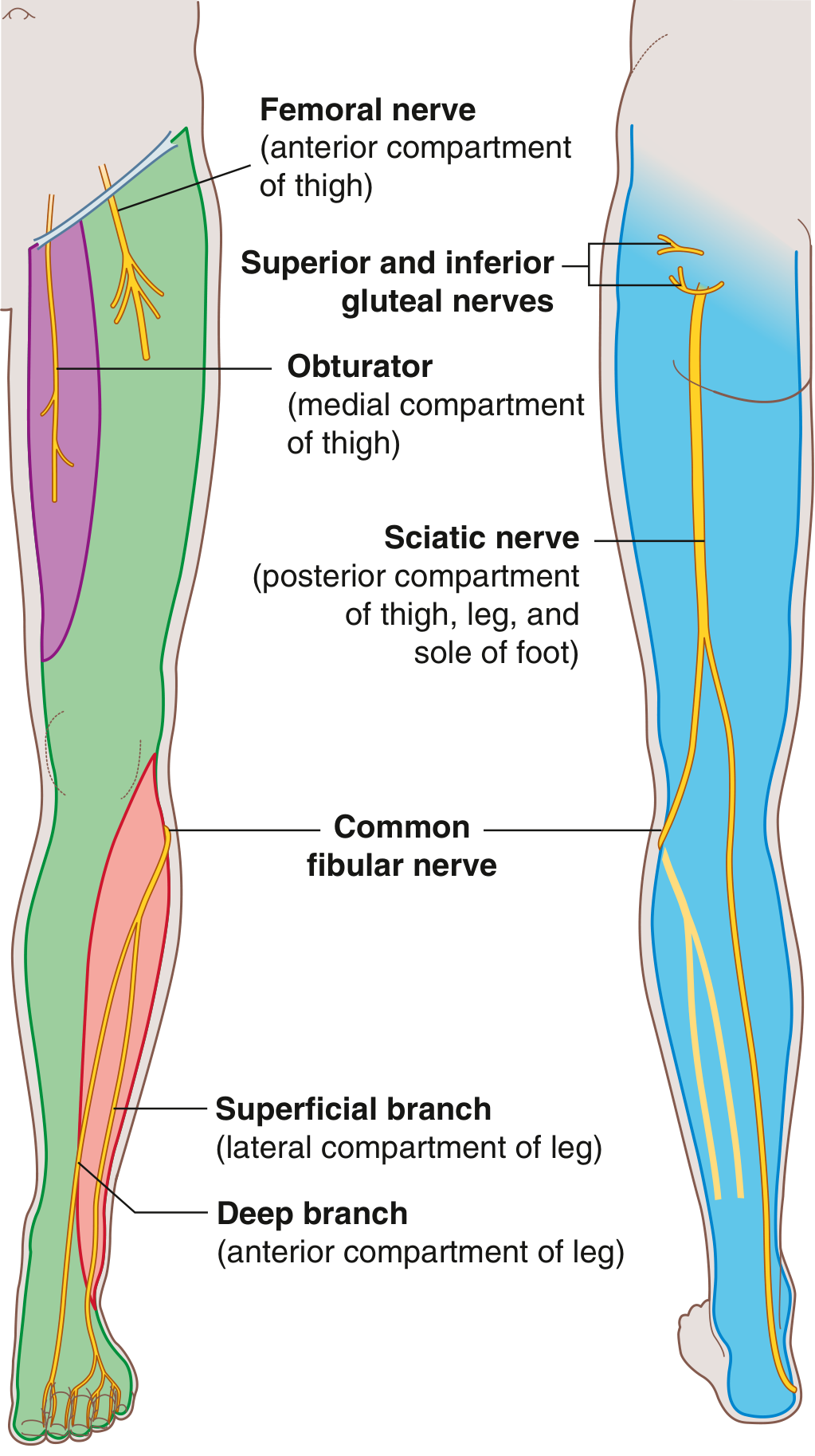
Fig. 6.18 - Major Nerves of the Lower Limb (Gray's Anatomy for Students)
| Nerve | Roots | Motor Supply | Sensory Area |
|---|---|---|---|
| Femoral | L2-L4 | Anterior thigh (quadriceps) | Anterior thigh, medial leg, medial ankle |
| Obturator | L2-L4 | Medial thigh (adductors) | Medial thigh |
| Sciatic | L4-S3 | Posterior thigh; splits into tibial + common fibular | Posterior limb |
| Tibial (from sciatic) | L4-S3 | Posterior leg, sole of foot | Lateral ankle/foot, sole |
| Common fibular (from sciatic) | L4-S2 | Anterior + lateral leg, dorsum foot | Lateral leg, dorsum of foot |
| Superior gluteal | L4-S1 | Gluteus medius, minimus, TFL | None major |
| Inferior gluteal | L5-S2 | Gluteus maximus | None major |
Dermatome quick reference:
- L1: inguinal ligament area
- L2: lateral thigh
- L3: medial lower thigh
- L4: medial great toe
- L5: medial digit II
- S1: little toe (digit V)
- S2: posterior thigh
Clinically relevant - nerves near bone:
- Common fibular nerve wraps around the neck of the fibula - highly vulnerable to injury (foot drop from lateral knee trauma or a tight cast)
- Femoral nerve can be injured in femoral triangle
Reflexes & Myotomes (Clinical Testing)
| Test | Level |
|---|---|
| Hip flexion | L1-L2 |
| Knee extension | L3-L4 |
| Knee flexion | L5-S2 |
| Plantarflexion | S1-S2 |
| Patellar reflex (tap patellar ligament) | L3-L4 |
| Ankle/calcaneal tendon reflex | S1-S2 |
Blood Supply
- External iliac artery → crosses inguinal ligament → femoral artery (femoral triangle)
- Femoral artery descends through the adductor canal → becomes popliteal artery behind the knee
- Popliteal artery divides into anterior tibial artery and posterior tibial artery (which gives off the fibular/peroneal artery)
- Posterior tibial artery passes through the tarsal tunnel and divides into medial and lateral plantar arteries in the sole
- Key clinical landmark: femoral artery is palpable just below the midpoint of the inguinal ligament
Side-by-Side Comparison
| Feature | Upper Limb | Lower Limb |
|---|---|---|
| Primary function | Dexterity, reach, manipulation | Weight bearing, locomotion |
| Nerve plexus | Brachial (C5-T1) | Lumbar + Sacral (L1-S3) |
| Gateway | Axillary inlet (over rib I) | Inguinal aperture (under inguinal ligament) |
| Main artery | Subclavian → Axillary → Brachial → Radial/Ulnar | External iliac → Femoral → Popliteal → Tibial |
| Largest nerve | Radial nerve | Sciatic nerve (largest in body) |
| Key clinical nerve injury | Median (carpal tunnel), Radial (humeral fracture) | Common fibular (neck of fibula) |
| Proximal joint | Glenohumeral (ball & socket) | Hip (ball & socket) |
| Intermediate joint | Elbow (hinge) | Knee (hinge) |
| Distal joint | Wrist (ellipsoid) | Ankle (mortise/hinge) |
All content from: Gray's Anatomy for Students (ISBN 9780323934237)
Now give dictionary for tough words
Here is a plain-language dictionary for the tough anatomical terms used in the extremity overview above.
Anatomical Dictionary - Extremity Terminology
A
Abduction
Moving a limb away from the midline of the body. Example: raising your arm out to the side.
Adduction
Moving a limb toward the midline of the body. Opposite of abduction.
Acromion
The bony projection at the top of the shoulder blade (scapula) that forms the "roof" of the shoulder joint.
Axilla
The armpit. A pyramid-shaped space that serves as the gateway between the neck and the arm, carrying all major vessels and nerves into the upper limb.
Axillary inlet
The triangular opening at the top of the armpit through which nerves, arteries, and veins travel to reach the arm.
B
Brachial plexus
A network of nerves originating from spinal cord levels C5 to T1 (neck and upper back) that branch out to supply the entire arm and hand.
Brachialis
A muscle in the front of the upper arm that flexes (bends) the elbow. Different from the biceps.
C
Calcaneus
The heel bone - the largest bone in the foot.
Carpal bones
The 8 small bones of the wrist, arranged in two rows. They allow the wrist to move in multiple directions.
Carpometacarpal (CMC) joint
The joint where the wrist bones (carpals) meet the hand bones (metacarpals). The thumb's CMC joint is a saddle joint and allows the widest range of motion.
Circumduction
A circular movement combining flexion, extension, abduction, and adduction. Imagine drawing a cone shape with your hand or foot.
Coracoid process
A hook-shaped bony projection on the front of the scapula (shoulder blade). Multiple muscles and ligaments attach here.
Cubital fossa
The triangular hollow on the front (anterior) side of the elbow. Important landmark where the brachial artery divides into the radial and ulnar arteries.
D
Deltoid
The large, triangular muscle covering the shoulder. Responsible mainly for abducting the arm.
Dermatome
A strip of skin supplied by a single spinal nerve. Doctors test dermatomes to identify which spinal nerve level is damaged.
E
Extension
Straightening a joint - increasing the angle between two body parts. Example: straightening a bent knee.
External rotation (lateral rotation)
Rotating a limb outward, away from the midline. Example: turning your foot outward.
F
Femoral triangle
A pyramid-shaped depression in the front upper thigh. It is the entry point where the femoral artery, femoral vein, and femoral nerve pass from the abdomen into the leg.
Femur
The thigh bone - the longest and strongest bone in the body.
Fibula
The thin, lateral (outer) bone of the leg. Mainly provides stability and muscle attachment rather than weight bearing.
Flexion
Bending a joint - decreasing the angle between two body parts. Example: bending your elbow.
G
Glenoid cavity
The shallow, cup-shaped socket on the scapula that holds the head of the humerus, forming the shoulder joint (glenohumeral joint).
Glenohumeral joint
The shoulder joint - a ball-and-socket joint formed between the head of the humerus and the glenoid cavity of the scapula. The most mobile joint in the body.
Gluteal fold
The crease of skin at the bottom of the buttocks, marking the lower boundary of the gluteal region.
Gracilis
A long, thin muscle on the inner thigh. It adducts the thigh and flexes the knee.
H
Hamstrings
A group of three muscles on the back of the thigh (biceps femoris, semimembranosus, semitendinosus). They extend the hip and flex the knee.
Humerus
The single bone of the upper arm, running from the shoulder joint to the elbow.
Hypothenar eminence
The fleshy muscle pad on the palm at the base of the little finger.
I
Iliac crest
The curved upper rim of the hip bone (ilium) - the bony ridge you can feel at the side of your waist.
Iliopsoas
A powerful hip flexor muscle formed by the combination of the iliacus and psoas major muscles.
Infraspinatus
One of the four rotator cuff muscles. It sits below the spine of the scapula and laterally rotates the arm.
Inguinal ligament
A fibrous band running from the anterior superior iliac spine (ASIS) to the pubic tubercle. It marks the boundary between the abdomen and the thigh.
Intermuscular septa
Fibrous partitions (walls) of connective tissue that divide the limb into separate compartments, each containing specific muscles.
Interossei
Small muscles between the metacarpals (hand) or metatarsals (foot). In the hand, they abduct and adduct the fingers and assist with flexion at the MCP joints.
Interphalangeal (IP) joint
The hinge joint between two phalanges (finger bones). The proximal IP (PIP) and distal IP (DIP) joints allow only flexion and extension.
L
Lateral
Toward the outside/side, away from the midline of the body.
Latissimus dorsi
A large, flat muscle of the lower back that extends, adducts, and medially rotates the arm. It pulls the arm downward and backward.
Lumbricals
Small worm-shaped muscles in the hand (and foot) that help flex the MCP joints while extending the IP joints - allowing the "typing" position of the fingers.
M
Medial
Toward the inside, closer to the midline of the body.
Metacarpals
The five long bones that form the palm of the hand, connecting the wrist bones (carpals) to the finger bones (phalanges).
Metacarpophalangeal (MCP) joint
The knuckle joint where the metacarpal meets the first phalanx. Allows flexion, extension, abduction, and adduction.
Metatarsals
The five long bones in the foot between the ankle bones (tarsals) and the toes. Mirror the metacarpals of the hand.
Myotome
A group of muscles supplied by a single spinal nerve root. Testing specific movements allows clinicians to identify which nerve root level is injured.
O
Obturator nerve
A nerve from the lumbar plexus (L2-L4) that supplies the adductor (inner thigh) muscles and sensation to the medial thigh.
P
Patella
The kneecap - a sesamoid bone embedded within the quadriceps tendon. It protects the knee joint and improves the mechanical advantage of the quadriceps.
Pectineus
A flat, quadrangular muscle in the upper inner thigh. It flexes and adducts the hip.
Pectoralis major
The large chest muscle that forms most of the front wall of the axilla. It adducts, flexes, and medially rotates the arm.
Phalanges (singular: phalanx)
The bones of the fingers or toes. Each finger (except the thumb) has 3 phalanges: proximal, middle, and distal.
Popliteal fossa
The diamond-shaped hollow at the back of the knee. Major blood vessels and nerves pass through here between the thigh and leg.
Pronation
Rotating the forearm so the palm faces downward or backward. The radius crosses over the ulna during this movement.
Proximal
Closer to the point of attachment to the body/trunk. Opposite of distal.
Q
Quadriceps femoris
A group of four muscles on the front of the thigh (rectus femoris, vastus medialis, vastus lateralis, vastus intermedius). Together they powerfully extend the knee.
Quadrangular space
An opening in the posterior shoulder through which the axillary nerve and posterior circumflex humeral artery pass.
R
Radial artery
One of the two terminal branches of the brachial artery. Runs along the lateral (thumb) side of the forearm. The pulse you feel at the wrist for measuring heart rate.
Rhomboids
Muscles connecting the medial border of the scapula to the thoracic spine. They retract (pull back) and elevate the scapula.
Rotator cuff
Four muscles (SITS: supraspinatus, infraspinatus, teres minor, subscapularis) that surround the glenohumeral joint, stabilizing the head of the humerus within the shallow glenoid cavity.
S
Sartorius
The longest muscle in the body, running diagonally across the thigh. It flexes, abducts, and laterally rotates the hip, and flexes the knee.
Sciatic nerve
The largest nerve in the body, arising from L4-S3. It runs down the posterior thigh and divides behind the knee into the tibial and common fibular nerves.
Scapula
The shoulder blade - a flat, triangular bone on the posterior chest wall that provides attachment for many shoulder and arm muscles.
Sesamoid bone
A small bone embedded within a tendon. The patella (kneecap) is the largest example.
Subscapularis
The only rotator cuff muscle on the front (anterior/deep) surface of the scapula. It medially rotates the arm.
Supination
Rotating the forearm so the palm faces upward or forward (the anatomical position). Opposite of pronation.
Supraspinatus
One of the four rotator cuff muscles. It initiates the first 15 degrees of arm abduction and is the most commonly torn rotator cuff muscle.
T
Talus
The ankle bone. It sits on top of the calcaneus (heel bone) and articulates with the tibia and fibula above to form the ankle joint.
Tarsal tunnel
A canal on the posteromedial side of the ankle formed by bones and the flexor retinaculum. Flexor tendons, the tibial nerve, and blood vessels pass through it into the foot.
Tarsals
The 7 bones of the ankle/hindfoot region: calcaneus, talus, navicular, cuboid, and 3 cuneiforms.
Tensor fasciae latae (TFL)
A muscle on the outer hip that tightens the iliotibial (IT) band and assists with hip abduction and medial rotation.
Teres minor
One of the four rotator cuff muscles. It laterally rotates the arm and helps stabilize the glenohumeral joint.
Thenar eminence
The fleshy muscle pad at the base of the thumb. Contains 3 intrinsic thumb muscles: abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis.
Tibia
The larger, medial bone of the leg (the shin bone). It bears most of the body's weight.
Trapezius
A large, diamond-shaped muscle of the upper back and neck. Elevates, depresses, retracts, and rotates the scapula.
U
Ulna
The medial bone of the forearm. The olecranon (the bony point of the elbow) is the proximal end of the ulna. The ulnar nerve runs behind the medial epicondyle adjacent to it.
Ulnar nerve
A major nerve from the brachial plexus (C8-T1) that passes behind the medial epicondyle (the "funny bone" sensation). Supplies most intrinsic hand muscles and sensation to the little finger and half the ring finger.
V
Volar
Relating to the palm of the hand or sole of the foot. Synonymous with "palmar" (hand) or "plantar" (foot).
Quick Pronunciation Guide
| Word | Sounds Like |
|---|---|
| Acromion | a-KROH-mee-on |
| Axilla | ak-SIL-ah |
| Glenoid | GLEE-noyd |
| Humerus | HYOO-mer-us |
| Inguinal | ING-gwi-nal |
| Patella | pa-TEL-ah |
| Phalanges | fah-LAN-jeez |
| Scapula | SKAP-yoo-lah |
| Trapezius | tra-PEE-zee-us |
| Thenar | THEE-nar |
Abdominal wall topic anatomy
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Excellent - I now have complete, rich material for a comprehensive abdominal wall anatomy topic. Let me compile the full response.
Abdominal Wall Anatomy
Sources: Gray's Anatomy for Students, Bailey & Love's Short Practice of Surgery, Sabiston Textbook of Surgery
Boundaries
The abdominal wall is a large musculofascial envelope with the following borders:
- Superior: xiphoid process and costal margins
- Posterior: vertebral column
- Inferior: upper parts of the pelvic bones (iliac crests, inguinal ligaments, pubic symphysis)
Layers of the Abdominal Wall (Superficial to Deep)
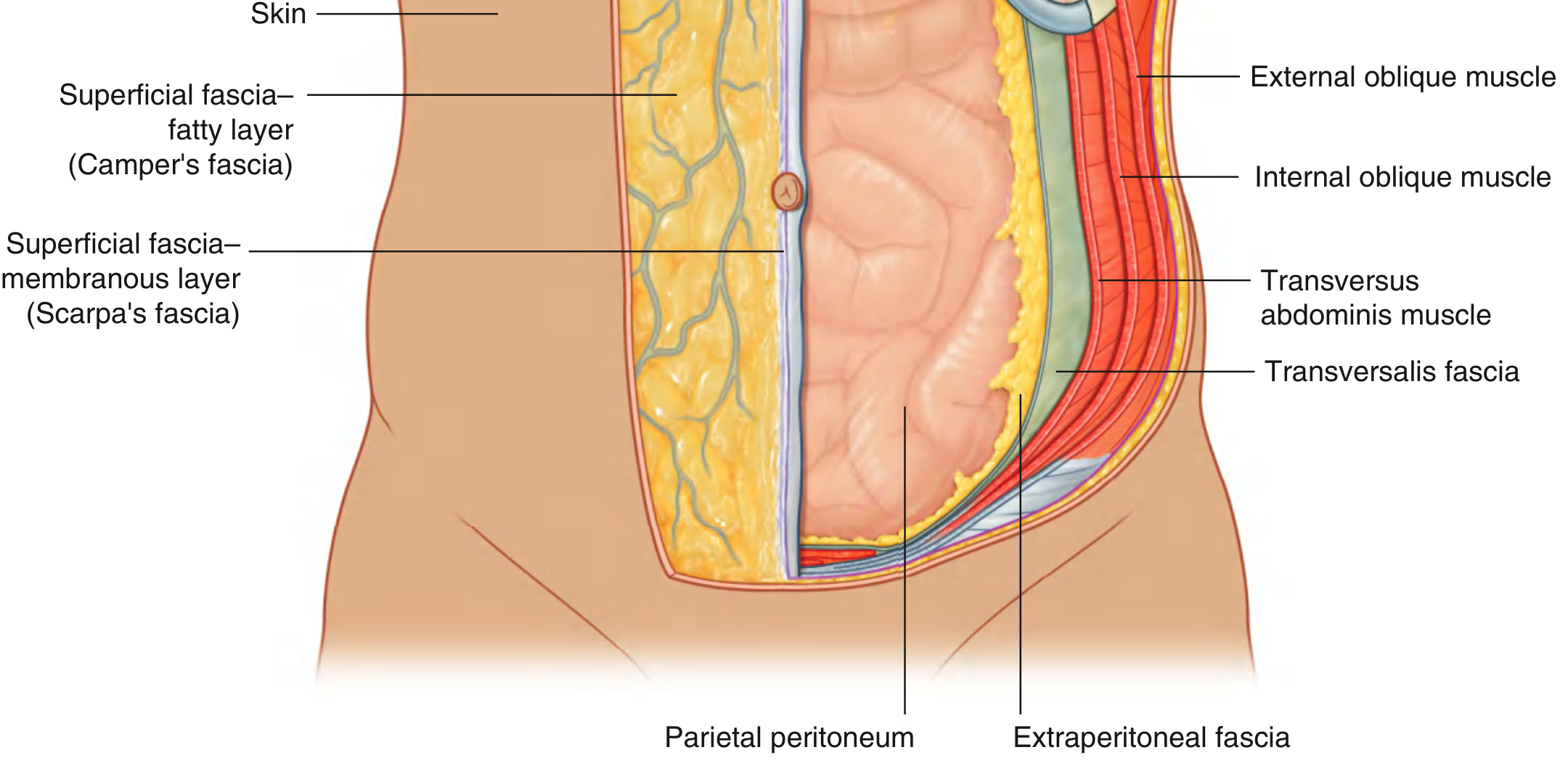
Fig. 4.24 - Layers of the Abdominal Wall (Gray's Anatomy for Students)
From outside to inside, the layers are:
- Skin
- Superficial fascia (two sub-layers below the umbilicus)
- Muscles + deep fascia (3 flat muscles laterally + 2 vertical muscles centrally)
- Transversalis fascia
- Extraperitoneal fascia (fat layer)
- Parietal peritoneum (innermost lining)
Layer 2: Superficial Fascia
Below the umbilicus, the superficial fascia splits into two named layers:
| Layer | Eponym | Contents | Continuity |
|---|---|---|---|
| Superficial fatty layer | Camper's fascia | Fat; varies in thickness | Continues over inguinal ligament into thigh; into scrotum/labia majora |
| Deep membranous layer | Scarpa's fascia | Little or no fat; thin membrane | Fuses with fascia lata just below inguinal ligament; attached to linea alba and pubic symphysis; continues as Colles' fascia in perineum |
Clinical note: Urine or blood tracking in the perineum (e.g., ruptured urethra) is contained by Scarpa's and Colles' fascia - it can spread upward under Scarpa's fascia onto the anterior abdominal wall but is blocked from going below the inguinal ligament (fused to fascia lata).
Layer 3: Muscles of the Abdominal Wall
The abdominal wall is a musculoaponeurotic girdle - a combination of muscles and their flat tendinous extensions (aponeuroses) that work together.
3 Flat (Lateral) Muscles
These three muscles are stacked in layers from outside to inside. Their fibers run in different directions, like layers of plywood, giving the wall great strength.
| Muscle | Fiber Direction | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|---|
| External oblique | Inferiomedial ("hands in pockets") | Lower 8 ribs (V-XII) | Iliac crest; linea alba via aponeurosis | T7-T12 | Compress abdomen; trunk flexion; rotate trunk to opposite side |
| Internal oblique | Superomedial (perpendicular to external) | Thoracolumbar fascia; iliac crest; lateral 2/3 inguinal ligament | Lower 3-4 ribs; linea alba; pubic crest | T7-T12, L1 | Compress abdomen; trunk flexion; rotate trunk to same side |
| Transversus abdominis | Transverse (horizontal) | Thoracolumbar fascia; iliac crest; lateral 1/3 inguinal ligament; lower 6 costal cartilages | Linea alba; pubic crest | T7-T12, L1 | Compress abdominal contents only (no rotation) |
2 Vertical (Anterior) Muscles
| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Rectus abdominis | Pubic crest, pubic tubercle, pubic symphysis | Costal cartilages V-VII; xiphoid process | T7-T12 | Flex vertebral column; compress abdomen; tense wall |
| Pyramidalis (small, often absent) | Front of pubis | Linea alba | T12 | Tenses linea alba |
Key Midline Structures
Linea Alba
- A fibrous band running from the xiphoid process to the pubic symphysis in the midline
- Formed by the interlacing (entwining) of the aponeuroses of all three flat muscles from both sides
- Wider above the umbilicus; narrows below it
- Surgeons use the linea alba for midline laparotomy incisions - avascular and easy to close
- Weakness here → epigastric or umbilical hernia
Rectus Sheath
The rectus abdominis muscle is enclosed in a fibrous sheath formed by the aponeuroses of the three flat muscles. The arrangement of the sheath changes at the arcuate line (midway between umbilicus and pubic symphysis):
| Location | Anterior rectus sheath | Posterior rectus sheath |
|---|---|---|
| Above arcuate line | External oblique aponeurosis + anterior leaf of internal oblique | Posterior leaf of internal oblique + transversus abdominis |
| Below arcuate line | All three aponeuroses pass anterior | Nothing - only transversalis fascia |
This creates a point of weakness below the arcuate line - the posterior wall is deficient (no muscle aponeurosis, only transversalis fascia). A spigelian hernia can occur at the linea semilunaris near the arcuate line.
Linea Semilunaris
- The curved lateral border of the rectus abdominis muscle, visible as an external groove
- Marks where the flat muscle aponeuroses begin to split to form the rectus sheath
Tendinous Intersections
- 3-4 fibrous bands crossing the rectus abdominis horizontally
- Fused to the anterior rectus sheath (but not the posterior) - this is why you can see distinct "six-pack" segments
Associated Ligaments (from External Oblique Aponeurosis)
The lower border of the external oblique aponeurosis condenses and folds inward to form several important ligaments:
| Ligament | Also Known As | Description |
|---|---|---|
| Inguinal ligament | Poupart's ligament | Lower folded border of external oblique aponeurosis; runs from ASIS to pubic tubercle; forms the floor of the inguinal canal |
| Lacunar ligament | - | Crescent-shaped extension at the medial end; passes backward to pecten pubis |
| Pectineal ligament | Cooper's ligament | Extension of lacunar ligament along the pecten pubis; important landmark in hernia repair |
The Inguinal Canal
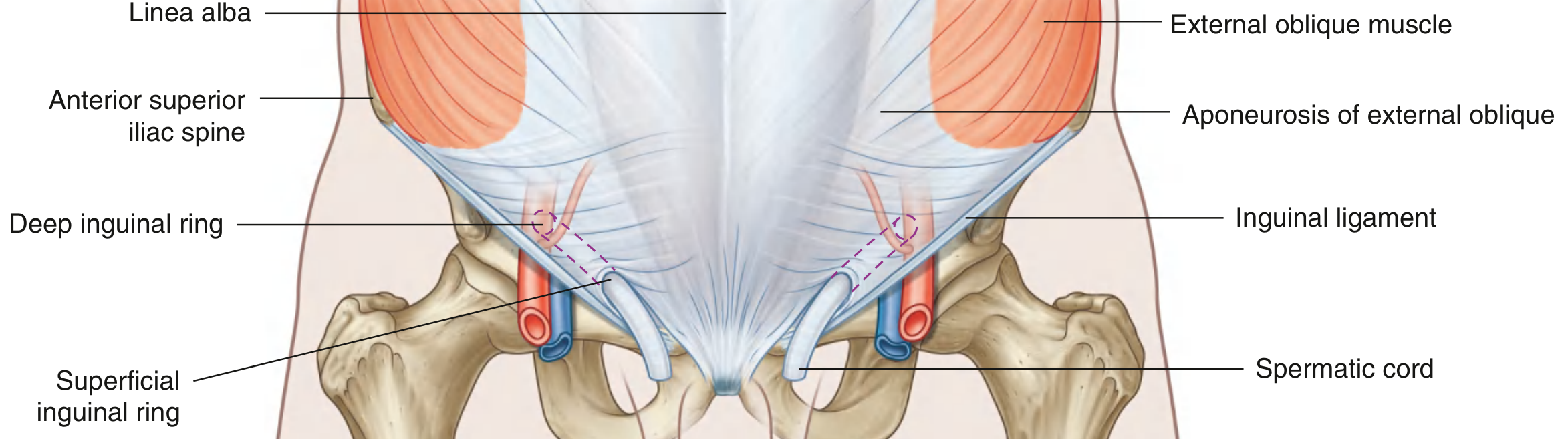
Fig. 4.42 - Inguinal Canal (Gray's Anatomy for Students)
The inguinal canal is a 4 cm slit-like passage running downward and medially, just above and parallel to the lower half of the inguinal ligament.
Openings
| Opening | Location | Structure |
|---|---|---|
| Deep (internal) inguinal ring | Midway between ASIS and pubic symphysis, just above inguinal ligament, lateral to inferior epigastric vessels | Opening in transversalis fascia |
| Superficial (external) inguinal ring | Just superior to the pubic tubercle | Triangular opening in aponeurosis of external oblique |
Four Walls of the Inguinal Canal
| Wall | Formed by |
|---|---|
| Anterior | Aponeurosis of external oblique (full length) + fibers of internal oblique (laterally, over deep ring) |
| Posterior | Transversalis fascia (full length) + conjoint tendon (medially, over superficial ring) |
| Roof (superior) | Arching fibers of transversus abdominis + internal oblique |
| Floor (inferior) | Medial half of inguinal ligament (rolled-under trough) + lacunar ligament medially |
Contents of the Inguinal Canal
| In Males | In Females |
|---|---|
| Spermatic cord | Round ligament of uterus |
| Genital branch of genitofemoral nerve | Genital branch of genitofemoral nerve |
| Ilioinguinal nerve (exits through superficial ring) | Ilioinguinal nerve |
Spermatic cord layers (acquired as it passes through the canal):
- Internal spermatic fascia (from transversalis fascia at deep ring)
- Cremasteric fascia + cremaster muscle (from internal oblique)
- External spermatic fascia (from external oblique aponeurosis at superficial ring)
Conjoint Tendon (Inguinal Falx)
The combined insertion of the transversus abdominis and internal oblique into the pubic crest and pectineal line. It reinforces the medial posterior wall of the inguinal canal - directly behind the superficial ring where direct hernias occur.
Nerves & Dermatomes
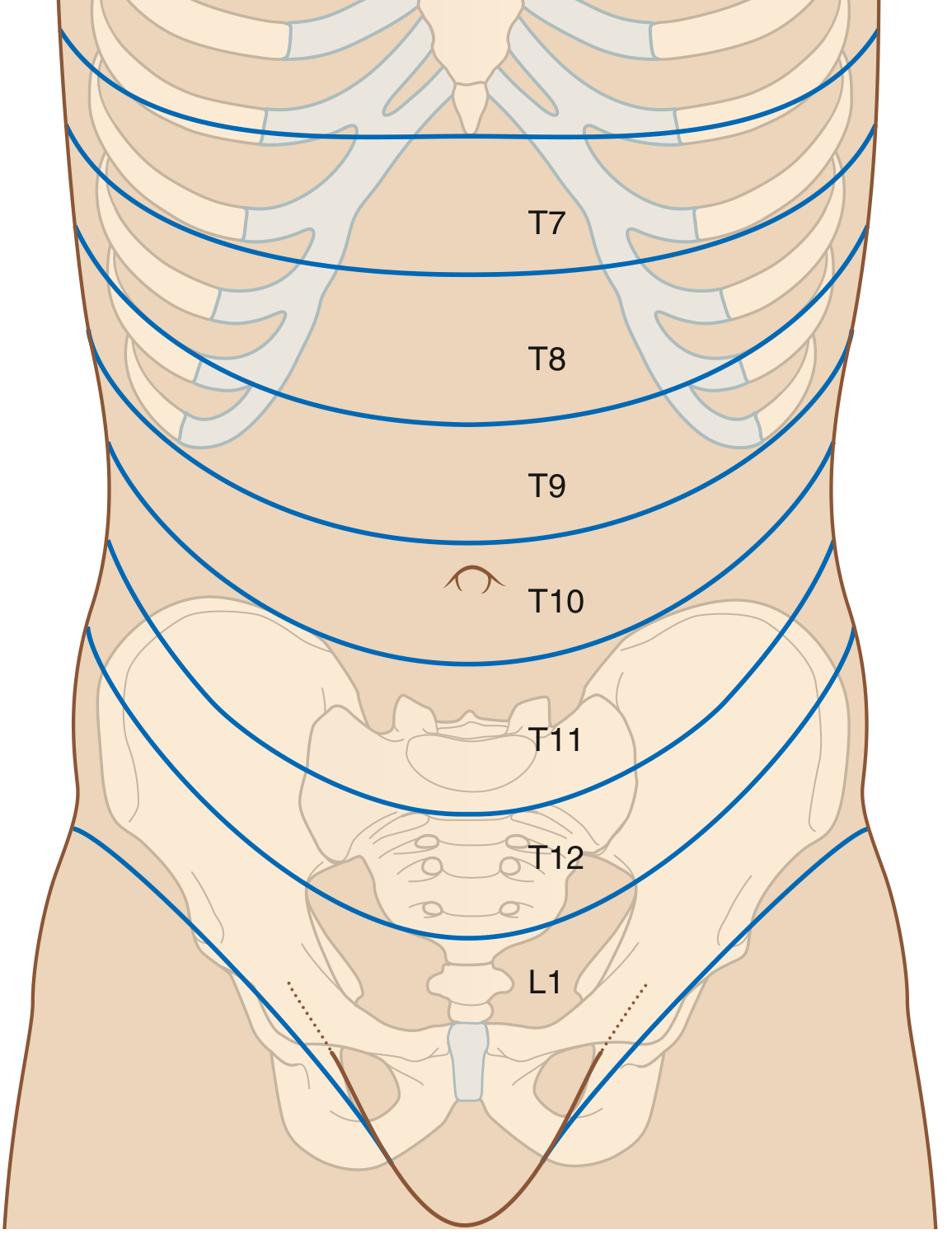
Fig. 4.38 - Abdominal Wall Dermatomes (Gray's Anatomy for Students)
The anterolateral abdominal wall is innervated by anterior rami of T7 to L1:
| Nerve Level | Area Supplied |
|---|---|
| T7 | Epigastric region (just below xiphoid) |
| T8-T9 | Upper abdomen |
| T10 | Umbilicus (key landmark) |
| T11-T12 | Below umbilicus |
| L1 (ilioinguinal + iliohypogastric) | Inguinal region, scrotum/labia majora, anterior thigh |
Clinical note: Appendicitis pain initially felt around the umbilicus (T10 = right midgut visceral referral), then shifts to the right iliac fossa (somatic) - this shift helps diagnose appendicitis.
Blood Supply
Superficial vessels
- Superior part: branches of musculophrenic artery (from internal thoracic)
- Inferior part: superficial epigastric artery + superficial circumflex iliac artery (both from femoral artery)
Deep vessels
| Vessel | Source | Region Supplied |
|---|---|---|
| Superior epigastric artery | Internal thoracic artery | Superior part of rectus sheath |
| Inferior epigastric artery | External iliac artery | Inferior part of rectus sheath; lateral to deep inguinal ring |
| Intercostal arteries (10th, 11th) + subcostal | Thoracic aorta | Lateral wall |
| Deep circumflex iliac artery | External iliac artery | Lateral inferior wall |
The superior and inferior epigastric arteries both enter the rectus sheath and anastomose with each other behind the rectus abdominis - forming a continuous vertical channel connecting the internal thoracic system (above) with the external iliac system (below).
Clinical note: The inferior epigastric vessels lie just medial to the deep inguinal ring - this relationship distinguishes indirect from direct inguinal hernias (see hernia section below).
Lymphatic Drainage
- Above umbilicus → lymph drains superiorly to axillary nodes
- Below umbilicus → lymph drains inferiorly to superficial inguinal nodes
Hernias of the Abdominal Wall
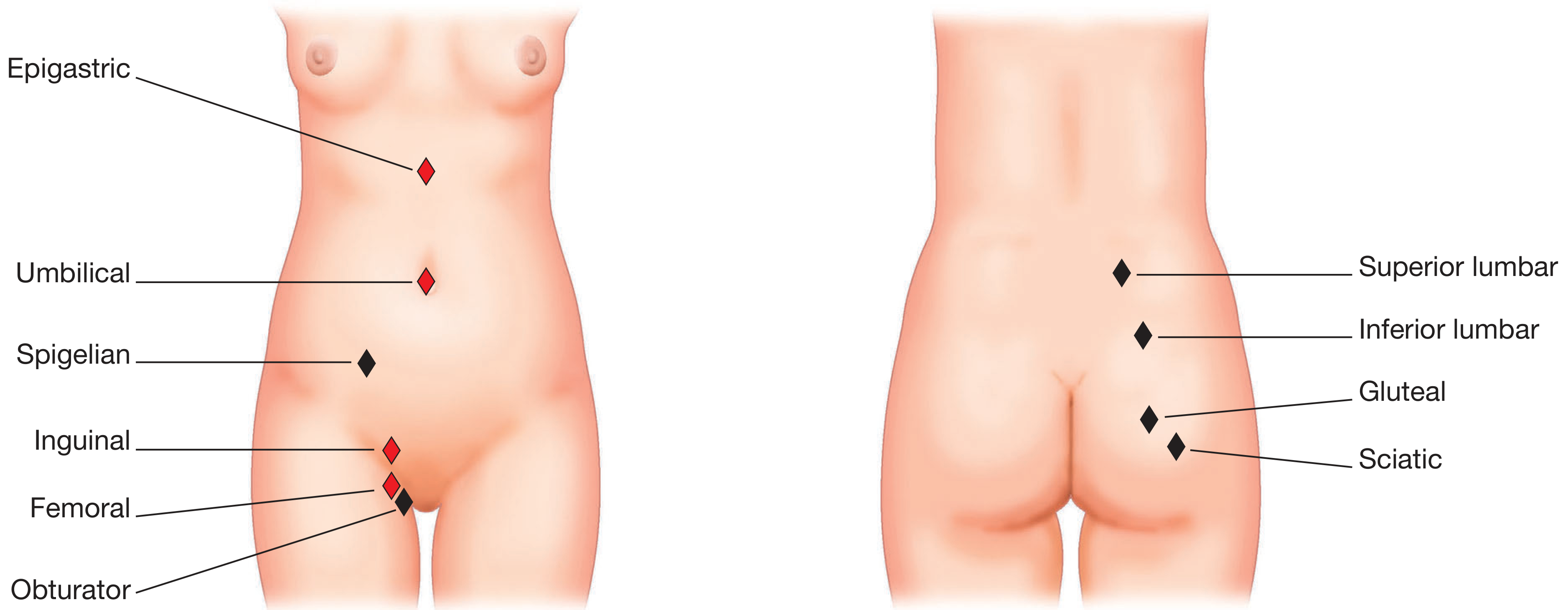
Sites of abdominal wall hernias - common (red) and rare (black) (Bailey & Love)

Fig. 64.10 - Direct, indirect inguinal and femoral hernia relationships (Bailey & Love)
Inguinal Hernias - Direct vs. Indirect
| Feature | Indirect Inguinal | Direct Inguinal |
|---|---|---|
| Path | Through deep inguinal ring → inguinal canal → superficial ring | Directly through posterior wall (Hesselbach's triangle) |
| Relation to inferior epigastric vessels | Lateral | Medial |
| Coverings | Passes through all 3 layers of spermatic cord | No internal spermatic fascia |
| Cause | Patent processus vaginalis (congenital) | Weakness in transversalis fascia (acquired) |
| More common in | Young males | Older males |
| Can descend into scrotum? | Yes | Rarely |
Hesselbach's triangle (direct hernia zone):
- Medially: lateral border of rectus abdominis
- Laterally: inferior epigastric vessels
- Inferiorly: inguinal ligament
Femoral Hernia
- Passes through the femoral canal (medial compartment of the femoral sheath), below the inguinal ligament
- More common in women
- High risk of strangulation due to rigid femoral ring boundaries (inguinal ligament above, lacunar ligament medially, pectineal ligament posteriorly, femoral vein laterally)
- Always presents below and lateral to the pubic tubercle (vs. inguinal hernia which is above and medial)
Summary of Hernia Sites
| Hernia | Location |
|---|---|
| Epigastric | Through linea alba above umbilicus |
| Umbilical | Through umbilical ring |
| Spigelian | Along linea semilunaris, near arcuate line |
| Indirect inguinal | Through deep inguinal ring (lateral to inferior epigastric) |
| Direct inguinal | Through Hesselbach's triangle (medial to inferior epigastric) |
| Femoral | Through femoral canal, below inguinal ligament |
| Incisional | Through previous surgical scar |
Clinical Summary - "Why the Inguinal Region is Weak"
The inguinal region has several overlapping points of weakness:
- The deep inguinal ring is a natural defect in the transversalis fascia
- Below the arching internal oblique/transversus fibers, there is no muscle layer - only fascia and aponeurosis
- The superficial inguinal ring is a triangular gap in the external oblique aponeurosis
- Increased intraabdominal pressure (straining, coughing, lifting) constantly stresses this region
The conjoint tendon acts as a natural "shutter" mechanism - when the internal oblique and transversus contract, the arching fibers tighten down over the deep ring, reducing the chance of herniation.
Sources: Gray's Anatomy for Students (ISBN 9780323934237), Bailey & Love's Short Practice of Surgery 28th Edition (ISBN 9780367548117), Sabiston Textbook of Surgery (ISBN 9780443124341)
I want dictionary for hard words for this topic
Abdominal Wall Anatomy - Dictionary of Hard Words
A
Anastomose / Anastomosis
When two blood vessels connect and join together. The superior and inferior epigastric arteries anastomose inside the rectus sheath, creating a continuous channel from chest to groin.
Aponeurosis (plural: aponeuroses)
A flat, broad sheet of tough white fibrous tissue that is the tendinous extension of a muscle. Instead of a round cord-like tendon, flat muscles like the obliques spread their pull across a wide area via their aponeuroses. The aponeuroses of the three flat abdominal muscles weave together to form the linea alba and the rectus sheath.
Arcuate line
A curved horizontal line on the posterior wall of the rectus sheath, located halfway between the umbilicus and the pubic symphysis. Below this line, all three aponeuroses pass in front of the rectus abdominis, leaving the posterior wall deficient (only transversalis fascia remains behind the muscle).
Anterior superior iliac spine (ASIS)
The bony projection you can feel at the front corner of the hip bone. It is the lateral attachment of the inguinal ligament and an important surgical landmark.
C
Camper's fascia
The superficial, fatty layer of the superficial fascia of the abdominal wall. Named after Dutch anatomist Petrus Camper. Contains fat and varies in thickness from person to person.
Colles' fascia
The continuation of Scarpa's fascia (deep membranous layer) into the perineum. Important clinically because urine from a ruptured urethra can track upward under Scarpa's fascia but is blocked from going down the thigh by the fascia's attachment to the fascia lata.
Conjoint tendon (Inguinal falx)
The merged tendon of the internal oblique and transversus abdominis muscles. They join together before attaching to the pubic crest and pectineal line. It reinforces the medial posterior wall of the inguinal canal - the area directly behind the superficial inguinal ring.
Cooper's ligament
See Pectineal ligament. A strong fibrous ridge along the pecten pubis, used as a solid anchoring point in hernia repair surgery.
Cremaster muscle
A thin layer of skeletal muscle that surrounds the spermatic cord and testis, derived from the internal oblique muscle. It can draw the testis upward (cremasteric reflex). The reflex is tested by stroking the inner thigh (L1-L2).
Cremasteric fascia
The covering around the spermatic cord contributed by the internal oblique muscle as the spermatic cord passes through the inguinal canal.
D
Deep inguinal ring
The proximal (internal) opening of the inguinal canal. It is a funnel-shaped defect in the transversalis fascia, located midway between the ASIS and pubic symphysis, just lateral to the inferior epigastric vessels. This is where indirect inguinal hernias begin.
Dartos fascia
A specialized layer in the scrotum containing smooth muscle fibers. It is derived from the fusion of Camper's and Scarpa's fascia as they continue over the penis and into the scrotum. The smooth muscle contracts in response to cold, wrinkling the scrotal skin.
E
Epigastric
Relating to the epigastric region - the upper middle area of the abdomen, between the costal margins and above the umbilicus.
External oblique
The outermost of the three flat abdominal muscles. Its fibers run diagonally downward and inward (like putting your hands in your front pockets). Its lower border forms the inguinal ligament.
Extraperitoneal fascia
A layer of loose fatty connective tissue lying between the transversalis fascia and the parietal peritoneum. It allows the peritoneum to slide against the abdominal wall. The urinary bladder and parts of the large intestine lie in this space.
F
Fascia lata
The deep fascia (strong fibrous stocking) of the thigh. Scarpa's fascia fuses with it just below the inguinal ligament - this fusion is why fluid tracking under Scarpa's fascia cannot go down the front of the thigh.
Femoral canal
The most medial compartment of the femoral sheath, just below the inguinal ligament. It is a small potential space that normally contains lymphatic vessels. A femoral hernia pushes into this canal.
Femoral ring
The upper opening of the femoral canal. It is bordered by the inguinal ligament (above), lacunar ligament (medially), pectineal ligament (posteriorly), and femoral vein (laterally). Because these borders are rigid, femoral hernias are at high risk of strangulation.
Femoral sheath
A funnel-shaped sleeve of fascia that encloses the femoral artery, femoral vein, and femoral canal as they pass under the inguinal ligament. The femoral nerve is NOT inside the sheath.
G
Genitofemoral nerve
A nerve from the lumbar plexus (L1-L2) that divides into two branches: the genital branch (travels through the inguinal canal; supplies the cremaster muscle and scrotal/labial skin) and the femoral branch (supplies a small patch of skin on the anterior thigh).
H
Hesselbach's triangle
The anatomical zone where direct inguinal hernias occur. Its three borders are: the lateral edge of the rectus abdominis (medially), the inferior epigastric vessels (laterally), and the inguinal ligament (inferiorly). A direct hernia bulges straight through the posterior wall within this triangle.
I
Iliohypogastric nerve
A branch of L1. It runs between the internal oblique and transversus abdominis muscles and supplies the skin of the lower abdominal wall (above the inguinal ligament) and the lateral buttock.
Ilioinguinal nerve
A branch of L1 that runs through the inguinal canal and exits at the superficial inguinal ring. It supplies sensation to the upper inner thigh, the anterior scrotum (males), or the anterior labia majora (females). Can be damaged during inguinal hernia repair, causing numbness or chronic pain in this area.
Inguinal ligament
Also called Poupart's ligament. The thickened, rolled-under lower border of the external oblique aponeurosis, stretching from the ASIS to the pubic tubercle. It acts as the floor of the inguinal canal and the roof of the femoral canal. A key surgical and anatomical landmark in the groin.
Internal oblique
The middle of the three flat muscles. Its fibers run in the opposite direction to the external oblique - upward and inward. It contributes to both the anterior and posterior walls of the inguinal canal and gives rise to the cremaster muscle.
Internal spermatic fascia
The innermost covering of the spermatic cord, derived from the transversalis fascia at the deep inguinal ring. It is the first layer picked up by the cord as it enters the canal.
L
Lacunar ligament
A crescent-shaped extension of fibers at the medial end of the inguinal ligament that turns backward to attach to the pecten pubis. It forms the medial border of the femoral ring. During femoral hernia repair, incising this ligament carefully creates space to reduce the hernia.
Laparotomy
A surgical incision through the abdominal wall to gain access to the abdominal cavity. Most commonly done through the linea alba (midline laparotomy).
Linea alba
Latin for "white line." The fibrous band running vertically down the exact midline of the anterior abdominal wall, from xiphoid to pubic symphysis. Formed by the interlacing of aponeuroses from both sides. It is avascular (no major blood vessels), which is why surgeons prefer it for incisions. Weakness here causes epigastric or umbilical hernias.
Linea semilunaris
The curved lateral border of the rectus abdominis muscle, visible as a groove on the surface of the abdomen in muscular individuals. It marks the lateral edge of the rectus sheath. A Spigelian hernia emerges here.
M
Musculoaponeurotic
Referring to a structure that is composed of both muscle (muscular) and aponeurosis (tendinous sheet). The entire abdominal wall is described as a musculoaponeurotic girdle because it combines muscular and flat tendinous components that work together as a unit.
P
Parietal peritoneum
The innermost layer of the abdominal wall. It is the serous membrane lining the inner surface of the abdominal and pelvic cavities (as opposed to the visceral peritoneum, which covers the organs themselves). It is pain-sensitive (supplied by somatic nerves), which is why irritation of the parietal peritoneum causes sharp, well-localized pain.
Patent processus vaginalis
During fetal development, a pouch of peritoneum (processus vaginalis) follows the testis into the scrotum. Normally this closes after birth. If it stays open (patent), it creates a ready-made pathway for an indirect inguinal hernia.
Pecten pubis
The smooth, sharp ridge on the superior ramus of the pubic bone. Several important ligaments (lacunar and pectineal/Cooper's) attach here.
Pectineal ligament (Cooper's ligament)
A strong, fibrous ridge running along the pecten pubis. Formed by fibers extending from the lacunar ligament. Used as a robust suture anchor during open inguinal and femoral hernia repair (e.g., McVay/Cooper's ligament repair).
Processus vaginalis
See Patent processus vaginalis above. The finger-like extension of peritoneum that descends with the testis during development.
Pubic symphysis
The cartilaginous joint connecting the two pubic bones at the midline. The linea alba, Scarpa's fascia, and the conjoint tendon all attach here. It is a key bony landmark for surgical planning in the lower abdomen and groin.
Pubic tubercle
A small bony projection on the upper surface of the pubic bone, about 2-3 cm from the midline. The medial end of the inguinal ligament attaches here. The superficial inguinal ring lies just above and medial to it. Clinicians use it to distinguish inguinal hernias (above and medial to the pubic tubercle) from femoral hernias (below and lateral).
R
Rectus abdominis
The paired vertical muscles running the full length of the anterior abdominal wall on either side of the midline. They flex the trunk and compress the abdominal cavity. Enclosed in the rectus sheath. The "six-pack" muscles.
Rectus sheath
The fibrous compartment enclosing the rectus abdominis muscle on all sides, formed by contributions from the aponeuroses of all three flat muscles. Its composition changes at the arcuate line - above it there is both an anterior and posterior wall; below it there is only an anterior wall (the posterior is just transversalis fascia).
S
Scarpa's fascia
The deep membranous (non-fatty) layer of the superficial fascia of the lower anterior abdominal wall. Named after Italian anatomist Antonio Scarpa. It is thin, membranous, and contains little fat. Fuses with the fascia lata below the inguinal ligament.
Spermatic cord
The bundle of structures running from the deep inguinal ring through the inguinal canal to the testis. Contents include: testicular artery, pampiniform venous plexus, vas deferens (ductus deferens), lymphatics, and the genital branch of the genitofemoral nerve. Enclosed in three fascial coverings acquired in the inguinal canal.
Spigelian hernia
A rare hernia that occurs through the linea semilunaris (at or near the arcuate line), where the posterior rectus sheath is deficient. Unlike most hernias, Spigelian hernias are often hidden beneath the intact external oblique - making them hard to diagnose without imaging.
Strangulation (hernia)
When the blood supply to herniated tissue is cut off by a tight hernia ring. The tissue becomes ischemic (loses blood) and can die (necrosis/gangrene) if not surgically treated urgently. Femoral hernias have the highest strangulation risk due to the rigid femoral ring.
Superficial inguinal ring
The distal (external) opening of the inguinal canal. A triangular gap in the aponeurosis of the external oblique, located just above and lateral to the pubic tubercle. Its apex points superolaterally; its base is the pubic crest.
T
Tendinous intersections
3-4 horizontal fibrous bands that cross the rectus abdominis and divide it into segments. They are fused to the anterior rectus sheath but not the posterior. They create the visible "blocks" of a six-pack abdomen.
Transversalis fascia
The layer of deep fascia lining the inner surface of the transversus abdominis muscle (and the entire abdominal cavity anteriorly). It forms the posterior wall of the inguinal canal. The deep inguinal ring is a funnel-shaped condensation of this fascia.
Transversus abdominis
The deepest of the three flat muscles, with fibers running completely horizontally like a corset. It compresses the abdominal contents but does not rotate the trunk. Its lower fibers arch over the inguinal canal to form its roof and fuse with internal oblique to form the conjoint tendon.
U
Umbilicus
The navel - a scar marking where the umbilical cord attached during fetal life. A key anatomical landmark at the level of the L3-L4 intervertebral disc. T10 dermatome encircles the body at this level. Weakness of the abdominal wall here leads to an umbilical hernia.
V
Vas deferens (Ductus deferens)
The muscular tube that carries sperm from the epididymis (in the scrotum) through the inguinal canal and into the pelvis. One of the key structures inside the spermatic cord. It is firm and cord-like and can be felt between the fingers when examining the spermatic cord.
Visceral peritoneum
The layer of peritoneum that directly covers the abdominal organs (stomach, intestines, etc.). Unlike the parietal peritoneum, it has no somatic nerve supply - it is not sensitive to sharp pain, only to stretch and ischemia.
Quick Reference - Named Structures & Eponyms
| Eponym | What It Is |
|---|---|
| Camper's fascia | Superficial fatty layer of abdominal superficial fascia |
| Scarpa's fascia | Deep membranous layer of abdominal superficial fascia |
| Colles' fascia | Scarpa's fascia in the perineum |
| Poupart's ligament | Inguinal ligament |
| Cooper's ligament | Pectineal ligament (along pecten pubis) |
| Hesselbach's triangle | Zone of direct inguinal hernias |
| Spigelian hernia | Hernia through linea semilunaris at arcuate line |
| Dartos fascia | Smooth muscle-containing scrotal fascia |
This is a shared conversation. Sign in to Orris to start your own chat.