Carbapenam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Carbapenems
Carbapenems are a class of beta-lactam antibiotics with the broadest antibacterial spectrum of any currently available antibiotic group. They are considered "last-resort" or empiric agents for serious, polymicrobial, or drug-resistant infections.
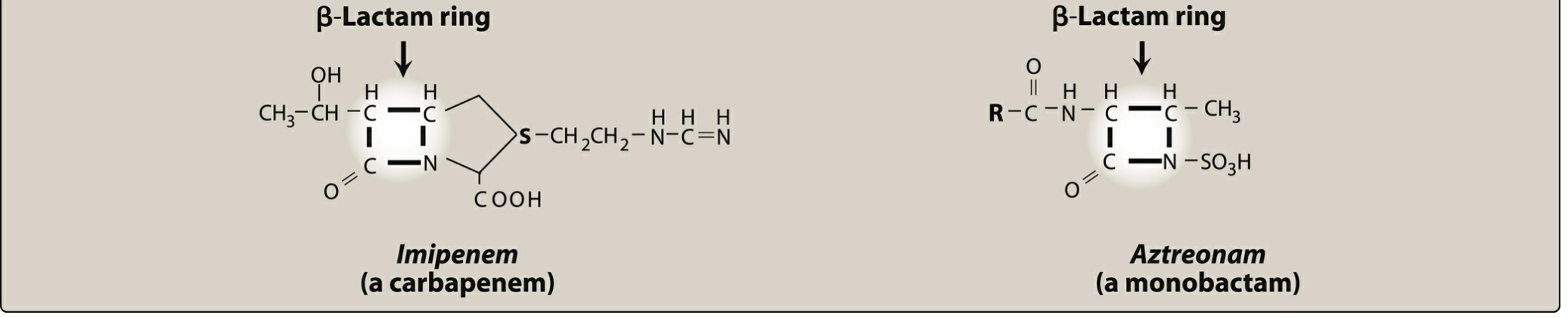
Structure
Carbapenems are synthetic beta-lactam antibiotics structurally related to penicillins. The key structural difference is that the sulfur atom of the thiazolidine ring has been externalized and replaced by a carbon atom, producing a bicyclic core with a beta-lactam ring fused to a five-membered ring.
Drugs in the Class
| Drug | Trade Name | Key Feature |
|---|---|---|
| Imipenem/cilastatin | Primaxin | First carbapenem; requires cilastatin to prevent renal degradation |
| Meropenem | Merrem | Does not require cilastatin; less seizurogenic |
| Ertapenem | Invanz | Once-daily dosing; no Pseudomonas coverage |
| Doripenem | Doribax | Greatest Pseudomonas activity; no longer available in USA |
Mechanism of Action
Like all beta-lactams, carbapenems inhibit bacterial cell wall synthesis by binding to penicillin-binding proteins (PBPs), preventing cross-linking of peptidoglycan. They are bactericidal and time-dependent in their killing.
Antibacterial Spectrum
Carbapenems (especially imipenem/meropenem) have the broadest spectrum of any beta-lactam:
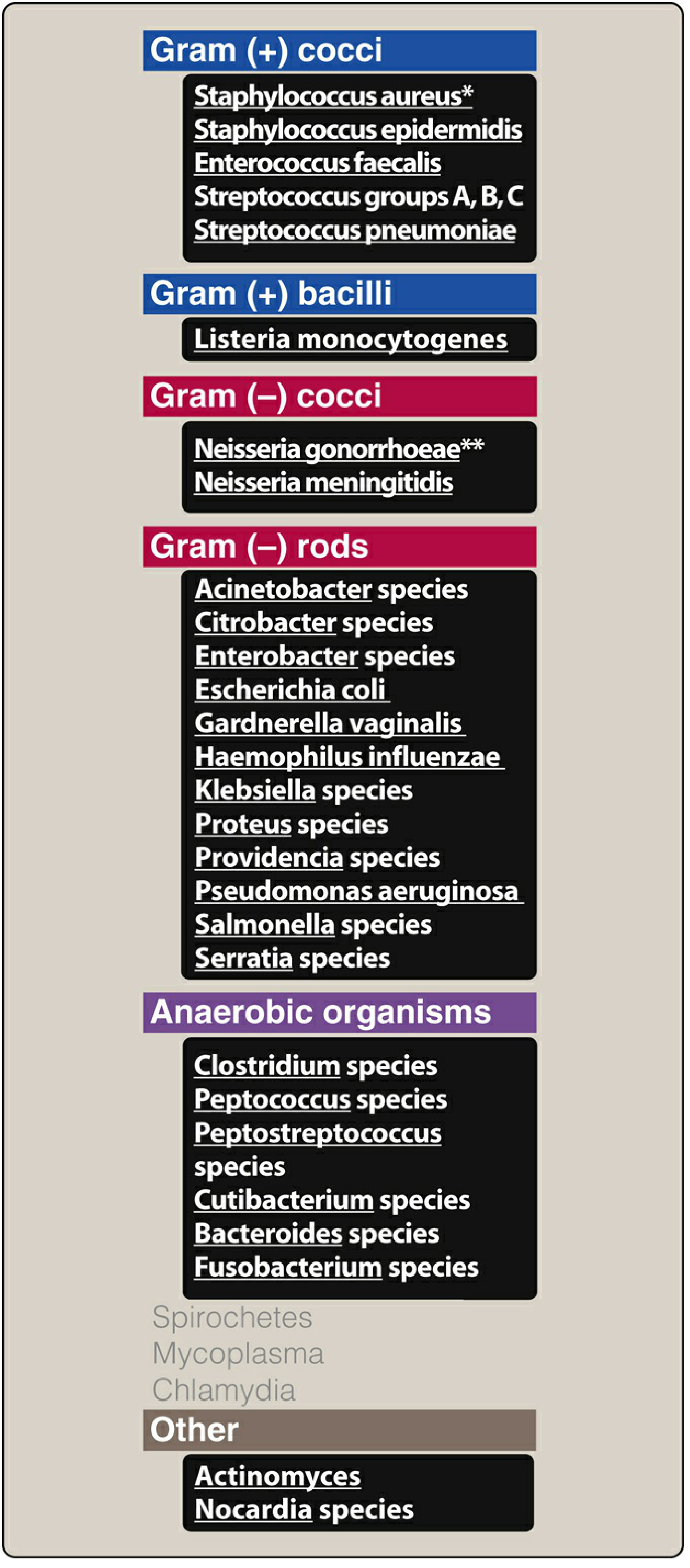
- Gram-positive cocci: S. aureus (MSSA), Streptococcus spp., Enterococcus faecalis, Listeria
- Gram-negative rods: E. coli, Klebsiella, Enterobacter, Serratia, Proteus, Acinetobacter, P. aeruginosa, Salmonella, H. influenzae
- Anaerobes: Bacteroides fragilis, Clostridium spp., Peptostreptococcus
Organisms NOT covered (resistant):
- Enterococcus faecium
- MRSA (methicillin-resistant S. aureus)
- Clostridioides difficile
- Stenotrophomonas maltophilia
- Burkholderia cepacia
- Ertapenem specifically: lacks P. aeruginosa, Enterococcus, and Acinetobacter coverage
Pharmacokinetics
| Feature | Details |
|---|---|
| Route | IV (all); ertapenem also IM (mixed with 1% lidocaine due to irritation) |
| Distribution | Penetrate well into body tissues and fluids, including CSF (except ertapenem); meropenem reaches therapeutic CSF levels even without meningeal inflammation |
| Elimination | Renal (glomerular filtration); dose adjustment required in renal insufficiency |
| Half-life | Imipenem ~1 hr; meropenem ~1 hr; ertapenem ~4 hr |
| Imipenem dosing | 0.25-0.5 g IV q6-8h |
| Meropenem dosing | 0.5-1 g IV q8h |
| Ertapenem dosing | 1 g IV/IM once daily |
Imipenem and Cilastatin
Imipenem is inactivated by dehydropeptidase-I in the brush border of the proximal renal tubule. It is therefore always co-administered with cilastatin, a dehydropeptidase inhibitor, to protect the drug from degradation and prolong its activity. Meropenem, doripenem, and ertapenem are not significantly degraded by this enzyme and do not require cilastatin.
Adverse Effects
- GI: Nausea, vomiting, diarrhea (most common)
- Seizures: High doses of imipenem, particularly in patients with renal failure or CNS disease. Meropenem is much less epileptogenic.
- Hypersensitivity: Cross-reactivity with penicillin is possible (shared bicyclic beta-lactam core) - use with caution in true penicillin allergy
- Infusion site reactions
- Eosinophilia and neutropenia (less common than other beta-lactams)
Clinical Indications
Carbapenems are reserved for:
- Polymicrobial infections (mixed aerobic/anaerobic)
- ESBL-producing gram-negative organisms (treatment of choice)
- Enterobacter infections (resist beta-lactamase destruction)
- Resistant P. aeruginosa infections (not ertapenem)
- Empiric therapy for severe, life-threatening infections
- Serious nosocomial infections (hospital-acquired/ventilator-associated pneumonia, complicated UTI, intra-abdominal infections)
Resistance - Carbapenem-Resistant Organisms (CRO)
Carbapenem resistance is a major clinical challenge. Resistant organisms may lack susceptibility to all traditional beta-lactams, fluoroquinolones, and aminoglycosides.
Resistance Mechanisms:
- Carbapenemases (serine carbapenemases - KPC, OXA; metallo-beta-lactamases - MBL/NDM/VIM)
- Outer membrane porin loss
- Efflux pump upregulation
Newer Agents for CROs:
| Combination | Active Against |
|---|---|
| Meropenem-vaborbactam (Vabomere) | KPC-producing Enterobacterales |
| Imipenem-cilastatin-relebactam (Recarbrio) | KPC-producing Enterobacterales, hospital/VAP |
| Ceftazidime-avibactam | KPC, AmpC, OXA-48 (not MBL) |
| Cefiderocol | All classes including MBL |
- None of the carbapenem/beta-lactamase inhibitor combinations cover metallo-beta-lactamases (MBL/NDM), except cefiderocol.
- Colistin (5 mg/kg once, then 1.67 mg/kg q8h) remains an option for pan-resistant CRO infections.
Beta-Lactamase Inhibitor Activity Summary
| Inhibitor | Class A (KPC) | Class B (MBL) | Class C (AmpC) | Class D (OXA) |
|---|---|---|---|---|
| Vaborbactam | + | - | - | - |
| Relebactam | + | - | + | +/- |
| Avibactam | + | - | + | +/- |
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Ch. 29
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Ch. 43
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Goldman-Cecil Medicine, 2-Vol Set, Ch. 281
NSAIDs drugs lipincott create a a good dedign pic
Finding Sources
Reading File
Reading File
Reading File
Generating Image
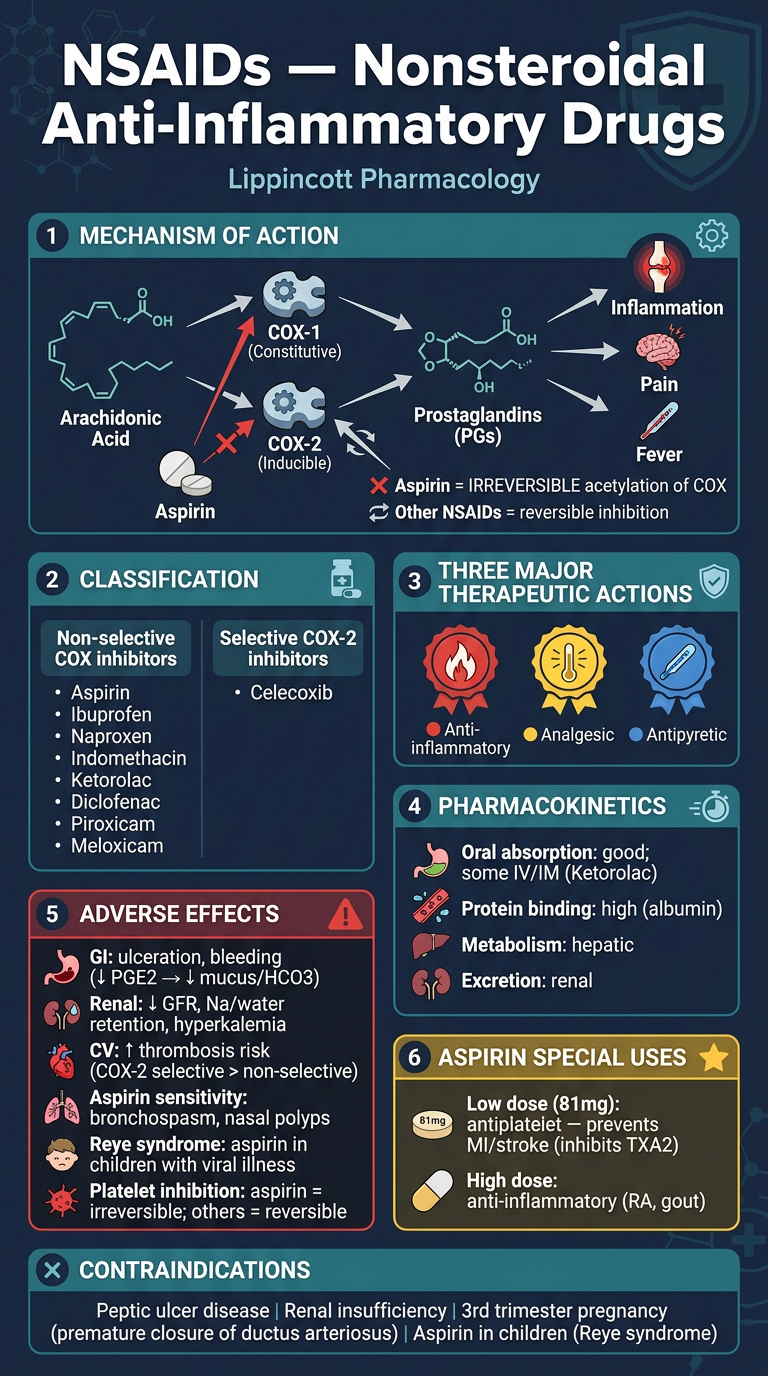
Here's your Lippincott-based NSAIDs infographic! It covers all the key pharmacology:
- Mechanism - COX-1/COX-2 inhibition pathway, with aspirin's unique irreversible acetylation
- Drug classification - non-selective vs. COX-2 selective (celecoxib) with all major agents
- 3 therapeutic actions - anti-inflammatory, analgesic, antipyretic
- Adverse effects - GI ulceration, renal effects, CV risk, Reye syndrome, bronchospasm
- Aspirin's special role - low-dose antiplatelet (TXA2 inhibition) vs. high-dose anti-inflammatory
- Key contraindications - PUD, renal insufficiency, 3rd trimester pregnancy, children with viral illness
Create a PPTX presentation on NSAID drug interactions and monitoring
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Running Command
Writing File
Running Command
Running Command
Your presentation is ready!
NSAIDs Drug Interactions Monitoring
Presentation · PPTX
9 slides, dark navy/teal/amber design theme. Here's what's inside:
| Slide | Content |
|---|---|
| 1 - Title | Cover slide with topic overview |
| 2 - Mechanism & COX Selectivity | COX pathway diagram + selectivity table for all major NSAIDs (aspirin through celecoxib) |
| 3 - Drug Interactions Part 1 | Warfarin, Aspirin+NSAIDs, Antihypertensives, Lithium - with mechanism, effect, severity badge & management |
| 4 - Drug Interactions Part 2 | Methotrexate, SSRIs/SNRIs, Corticosteroids, CYP2C9 inhibitors, Cyclosporine, Probenecid |
| 5 - Adverse Effects Profile | GI, Renal, Cardiovascular effects in color-coded columns |
| 6 - Special Populations | Pregnancy, Pediatrics, Elderly, Renal/Hepatic impairment, CVD - 6 cards with specific guidance |
| 7 - Monitoring Parameters | Full monitoring table (renal, GI, CBC, LFTs, INR, lithium levels) + GI protection strategy + patient counselling |
| 8 - Quick Reference Table | All 10 interactions in one severity-coded table (MAJOR/MODERATE) |
| 9 - Key Takeaways | 6 clinical pearls summarizing the whole presentation |
All content sourced from Lippincott Illustrated Reviews: Pharmacology, 8th Edition.
This is a shared conversation. Sign in to Orris to start your own chat.