
42 year old with post Lap hysterectomy 2 months ago with continuous urinary leakage from the vagina how to manage
Reading File
Finding Sources
Searching PubMed
"vesicovaginal fistula" AND repair
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both textbooks. Here is a structured management plan for this patient:
Management of Post-Laparoscopic Hysterectomy Vesicovaginal Fistula (VVF)
Summary of CT Findings
The CT Urogram confirms a vesicovaginal fistula (VVF) — fistulous communication between the base of the urinary bladder and the vaginal vault, near the right vesicoureteric junction (VUJ), with active contrast extravasation into the vaginal vault. Both ureters are normal, and there is no hydronephrosis, ruling out a concurrent ureterovaginal fistula.
Diagnostic Algorithm
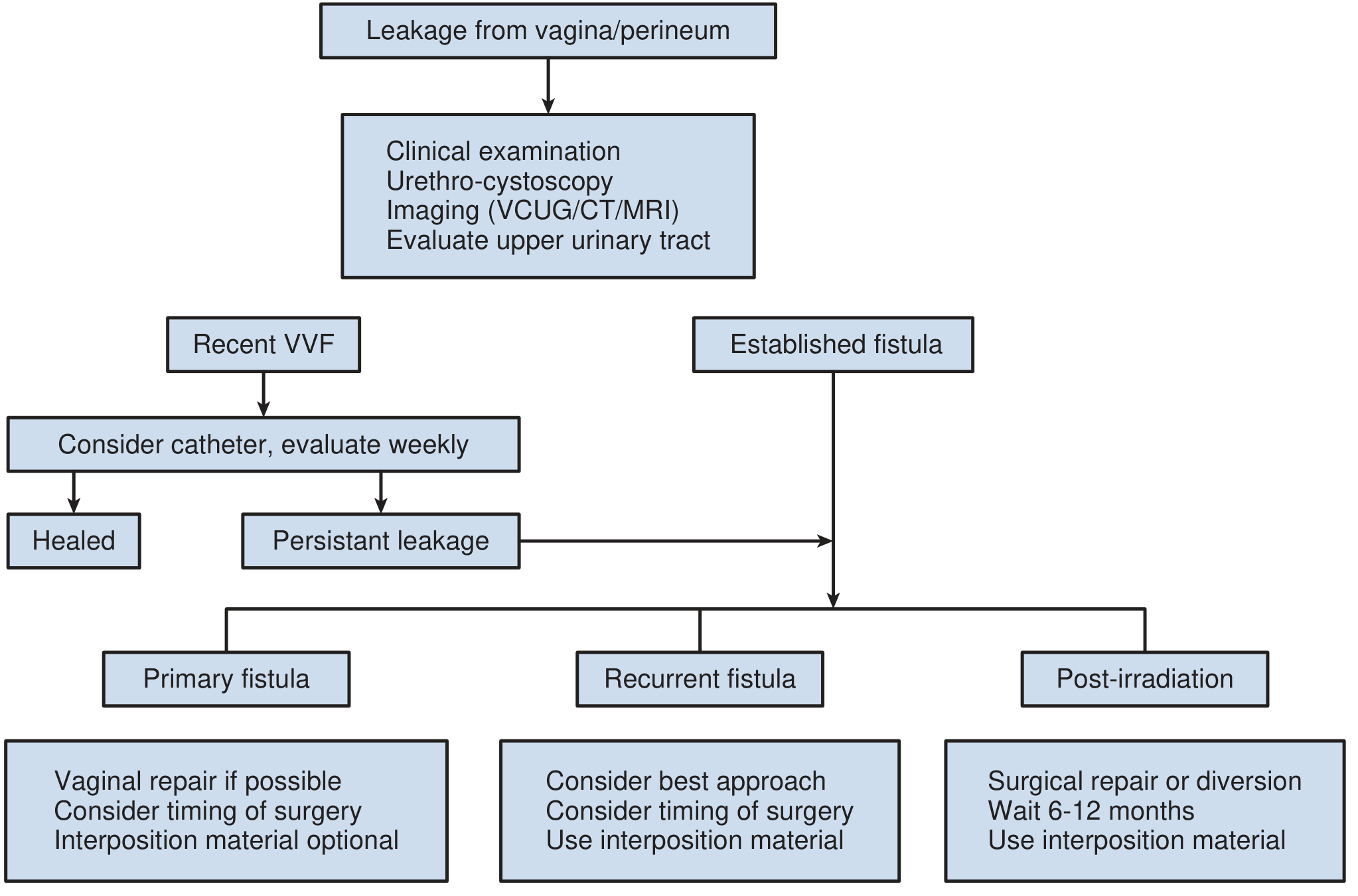
Step-by-Step Management
1. Confirm & Characterize the Fistula
CT Urogram already confirms VVF. Additionally perform:
| Investigation | Purpose |
|---|---|
| Cystoscopy | Identify exact fistula location, size, proximity to ureteric orifices; assess bladder mucosa |
| Examination under anesthesia (EUA) + speculum exam | Visualize the vaginal opening of the fistula |
| Double dye test (oral pyridium + intravesical methylene blue + tampon) | Distinguish VVF from ureterovaginal fistula if any doubt remains |
| Retrograde pyelogram/ureteroscopy | If fistula is near the right VUJ (as in this case), rule out partial ureteric involvement |
Critical: Given the proximity of the fistula to the right VUJ, ureteric integrity must be confirmed before repair planning.
2. Immediate Conservative Management
- Insert a Foley catheter for continuous bladder drainage — up to 15% of post-surgical VVFs close spontaneously with 4–6 weeks of uninterrupted bladder drainage.
- Treat any concurrent UTI with appropriate antibiotics.
- Ensure patient is well-nourished and manage local vaginal inflammation.
- Re-evaluate at 4–6 weeks: if still leaking → plan surgical repair.
Since this patient is 2 months post-op, the spontaneous closure window has likely passed. Surgical repair is the expected next step.
3. Timing of Surgery
| Scenario | Recommendation |
|---|---|
| Early window (within 2–3 weeks of VVF) | Immediate vaginal repair acceptable |
| Established fistula (as in this case — 2 months post-op) | Wait until tissue is supple, non-inflamed — typically allow 3–4 months from diagnosis, though with a post-gynecologic (non-radiation, non-obstetric) fistula, repair can often be done once tissues are pliable |
| Radiation/obstetric fistula | Delay 6–12 months |
Since this is a post-laparoscopic hysterectomy (benign cause, no radiation), repair is indicated when vaginal cuff and bladder tissues are soft and pliable — typically reassess every 1–2 weeks and schedule when ready.
4. Surgical Repair — Choice of Approach
Transvaginal repair is preferred for the majority of post-hysterectomy VVFs:
| Approach | Indication |
|---|---|
| Transvaginal (Latzko technique or layered closure) | Post-hysterectomy VVF above trigone, accessible vaginally — preferred for this patient |
| Transabdominal (O'Connor technique) | Large fistula, complex fistula, need for ureteric reimplantation, failed vaginal repair |
| Laparoscopic/Robotic transabdominal | Increasingly used, good outcomes; especially if near VUJ and ureteric reimplantation needed |
Since the fistula is near the right VUJ, a robotic or laparoscopic transabdominal approach with possible right ureteric reimplantation (ureteroneocystostomy) should be strongly considered. Urology involvement is essential.
5. Principles of Surgical Repair (4-Layer Closure — Transvaginal)
- Bladder mucosa — close the bladder defect
- Seromuscular layer of the bladder
- Endopelvic fascia / pubocervical fascia (interpositional layer)
- Vaginal epithelium — close without tension
Key technical principles:
- Adequate tissue mobilization and sharp dissection
- Tension-free, multilayered closure
- Remove/avoid any foreign body
- Consider Martius flap (labial fat pad) or omental interposition as an adjunct in complex cases or recurrent fistulas
- Postoperative continuous bladder drainage for 2–3 weeks (Foley ± suprapubic catheter)
6. Postoperative Care
- Foley catheter for 2–3 weeks post-repair
- Pelvic rest for 3 months
- Void cystourethrogram before catheter removal to confirm closure
- Monitor for residual stress urinary incontinence (SUI) — may require a separate continence procedure later
7. Urology Referral — Mandatory
Given proximity to the right VUJ, this case requires joint management with a urologist:
- Rule out right ureteric injury
- If ureteric involvement: ureteric stenting or reimplantation may be required at the time of fistula repair
Prognosis
Success rates for primary VVF repair in post-gynecologic cases exceed 85–94% when performed by experienced surgeons. Transvaginal approaches have shown 90.8% closure vs. 83.9% for transabdominal in systematic reviews. The best chance of cure is with the first repair — careful preoperative planning is therefore essential.
Sources:
- Berek & Novak's Gynecology, p. 1464
- Campbell-Walsh-Wein Urology (3-Volume Set), pp. 3887–3892
- Hinman's Atlas of Urologic Surgery, p. 654
- Repair of Vesicovaginal Fistulae: A Systematic Review — Obstet Gynecol 2024 (PMID: 38033311)
This is a shared conversation. Sign in to Orris to start your own chat.