Cholecystectomy
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Sabiston, Maingot's, Fischer's Mastery, and Current Surgical Therapy, plus excellent images. Let me compile a thorough, well-structured answer.
Laparoscopic Cholecystectomy - Technique & Anatomy
Historical Background
Laparoscopic cholecystectomy (LC) was first performed by Muhe in 1985 and then popularized by Mouret in 1987. It is now one of the most commonly performed general surgery procedures worldwide, with >80% of cholecystectomies done laparoscopically. Compared to open cholecystectomy, it delivers smaller incisions, less pain, shorter hospitalization, and faster return to function - though it carries a higher bile duct injury (BDI) rate (0.4-1.3% vs. 0.2% open). - Sabiston Textbook of Surgery, p. 1838
Indications and Contraindications
Standard indications: biliary colic, acute cholecystitis, gallstone pancreatitis, choledocholithiasis (as part of management), biliary dyskinesia, gallbladder polyps >1 cm.
Absolute contraindications:
- Inability to tolerate general anesthesia
- End-stage liver disease with portal hypertension (unsafe portal dissection)
- Coagulopathy
Relative contraindications:
- Severe COPD (poor CO2 exchange)
- Congestive heart failure
- Pulmonary hypertension
- Significant prior upper abdominal surgery (higher conversion rate)
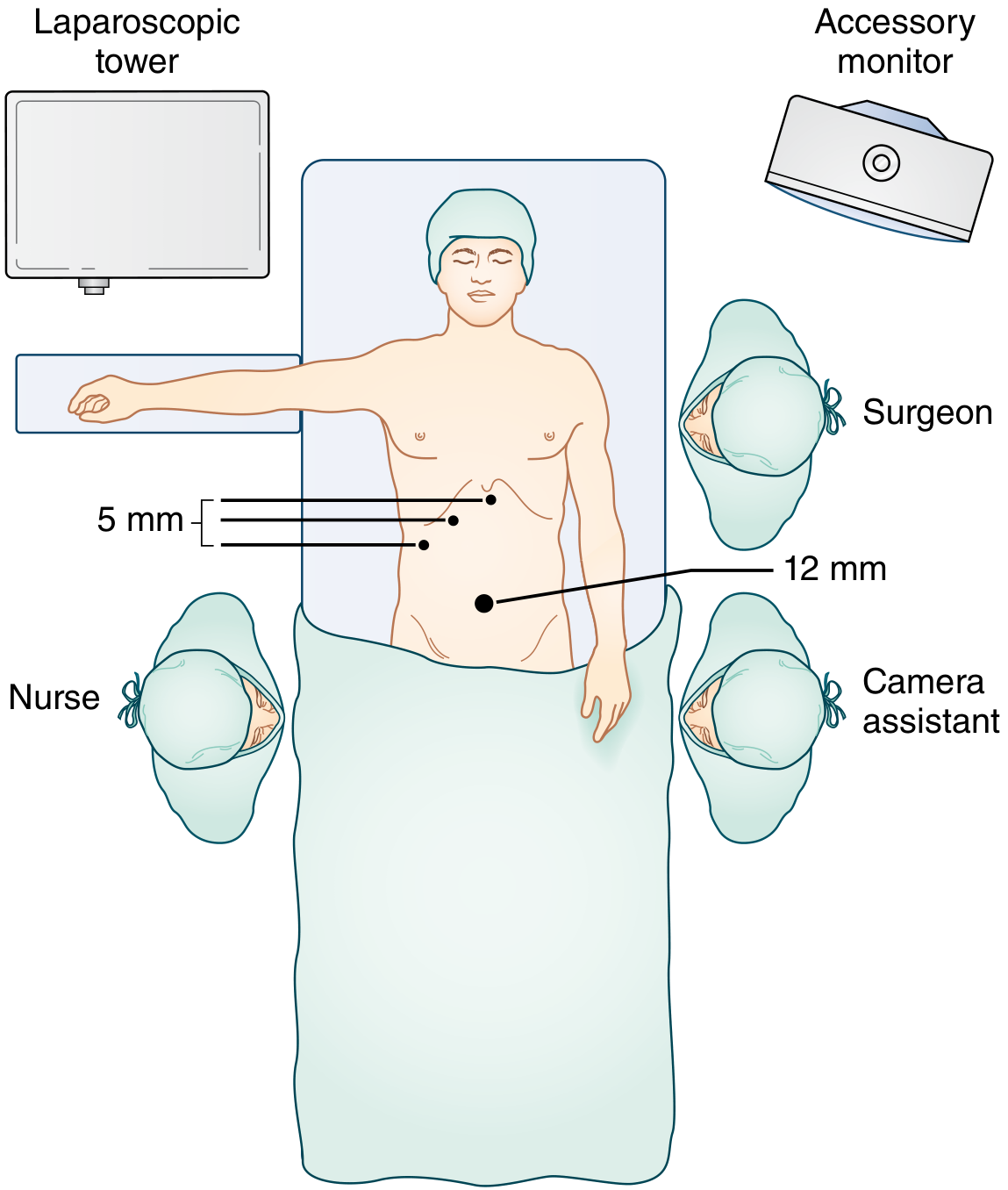
Operating Room Setup
American technique: Surgeon stands to the left of the patient; first assistant to the right. Two video monitors, one on each side of the table. The patient is supine with one arm tucked (to allow for potential intraoperative cholangiogram).
French technique: Patient's legs are abducted; surgeon stands between the legs.
An orogastric tube decompresses the stomach. The patient must be well secured to the table for steep reverse Trendelenburg positioning (30°), with 15° left lateral tilt - this allows the colon and duodenum to fall away from the liver edge by gravity.
Pneumoperitoneum
CO2 is used - it is noncombustible and rapidly absorbed from the peritoneal cavity (though it can cause hypercarbia in patients with significant cardiopulmonary disease). Entry is most commonly at the midline near the umbilicus via:
- Closed technique (Veress needle): CO2 insufflated through a Veress needle, then replaced blindly with a laparoscopic port.
- Open technique (Hasson): Laparoscopic port inserted under direct vision via a small incision - preferred in patients with prior abdominal surgery or concern for adhesions.
Port Placement
The standard 4-port technique uses:
| Port | Size | Location | Function |
|---|---|---|---|
| 1 | 12 mm | Periumbilical | Camera; gallbladder extraction |
| 2 | 5 mm | Right anterior axillary line | Elevate gallbladder fundus (assistant) |
| 3 | 5 mm | Right midclavicular (subcostal) | Grasp infundibulum / retract neck |
| 4 | 5 mm | Subxiphoid/epigastric | Surgeon's primary working port (dissection) |
A 30° or 45° angled laparoscope is preferred over 0° - it allows multiple viewing angles of the same operative field.
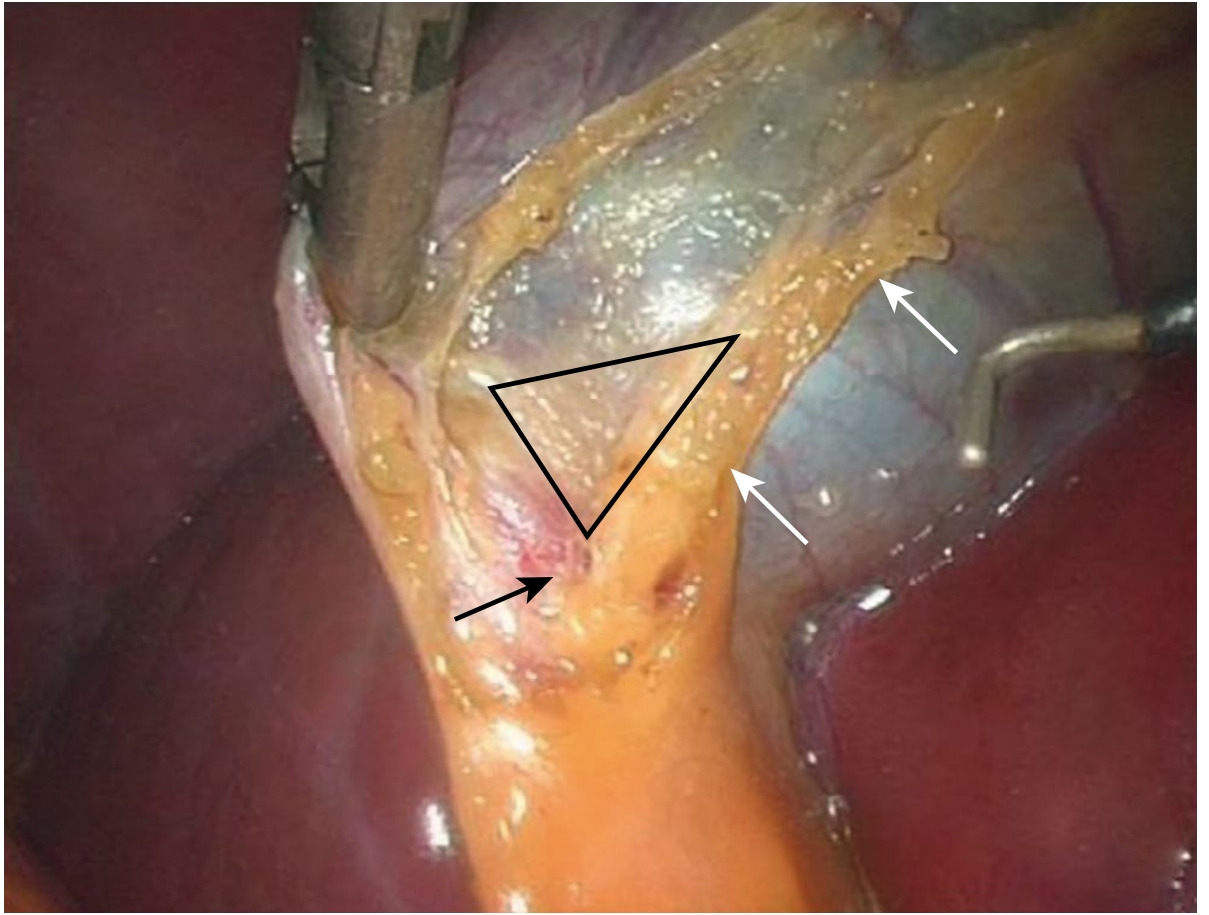
Surgical Anatomy: The Hepatocystic Triangle
The key anatomical region is the hepatocystic triangle (historically called "triangle of Calot"), bounded by:
- Medially: Common hepatic duct
- Laterally: Cystic duct
- Superiorly: Inferior surface of the liver / cystic plate
Within or near this triangle lie the cystic artery (typically arising from the right hepatic artery) and the Calot node - a lymph node that overlies the cystic artery and serves as a useful surgical landmark.
Anatomical variability is common - the cystic artery may arise from the left hepatic, proper hepatic, or gastroduodenal artery. A low-lying right or right posterior hepatic duct is a particularly dangerous variant and may not be visible on ERCP (requiring PTC for identification).
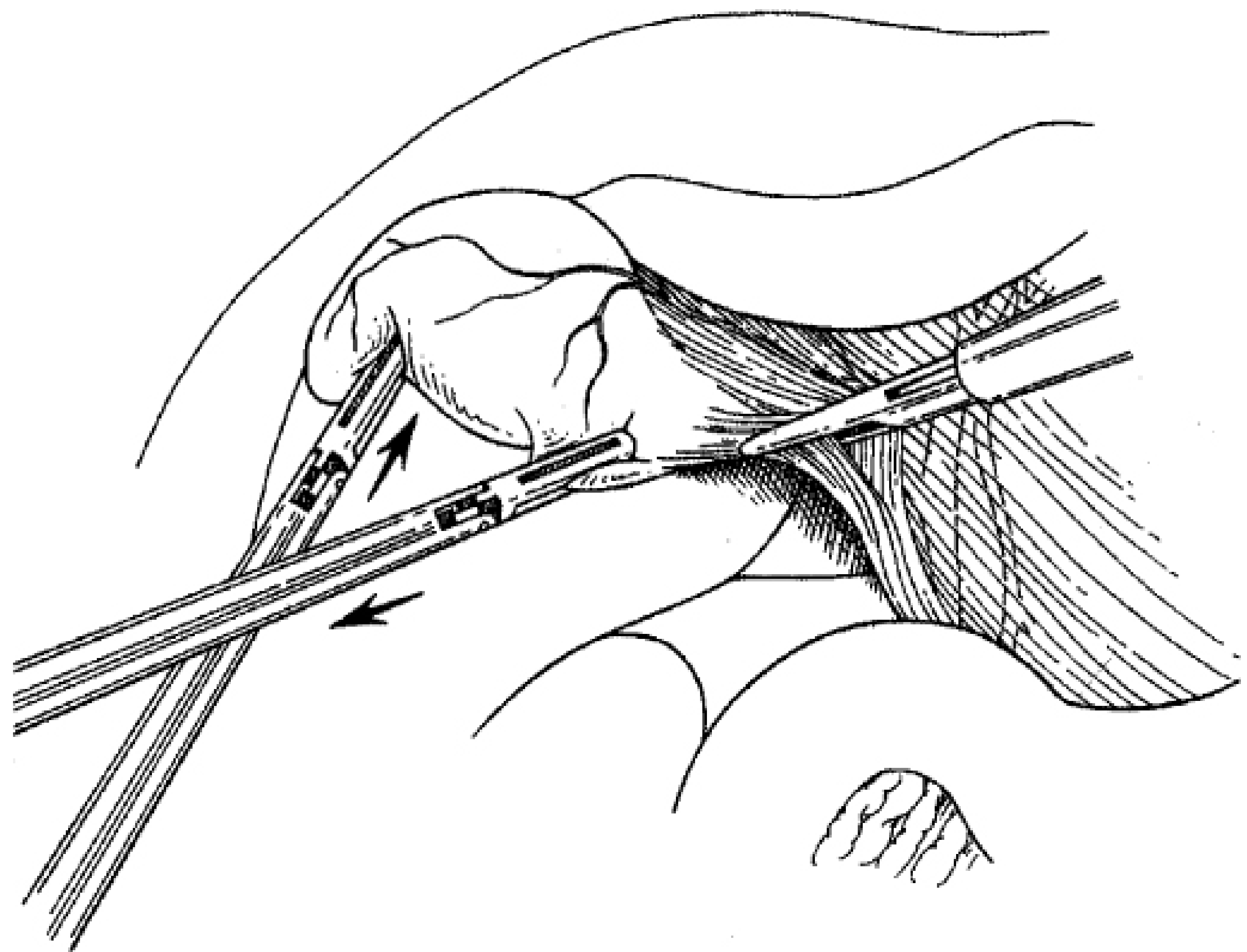
Dissection Technique
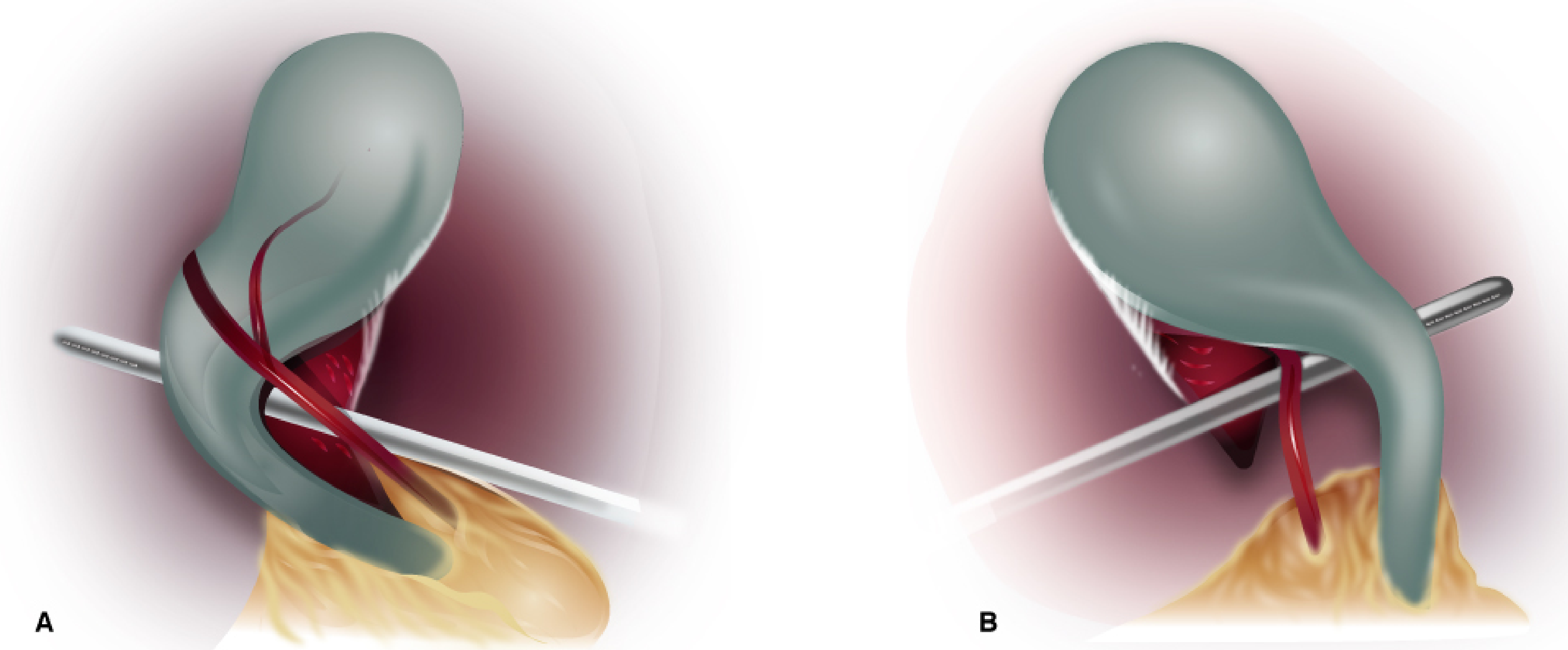
Step 1: Fundus Retraction
The assistant grasps the gallbladder fundus via the lateral axillary port and elevates it cephalad toward the right shoulder. This unfolds the hepatocystic triangle.
Step 2: Infundibulum Retraction
The surgeon uses the midclavicular port to grasp Hartmann's pouch (the infundibulum) and retracts it inferolaterally. This opens up the hepatocystic triangle.
The key maneuver is this inferolateral traction of the infundibulum - it straightens and exposes the cystic duct-CBD junction, separating them visually.
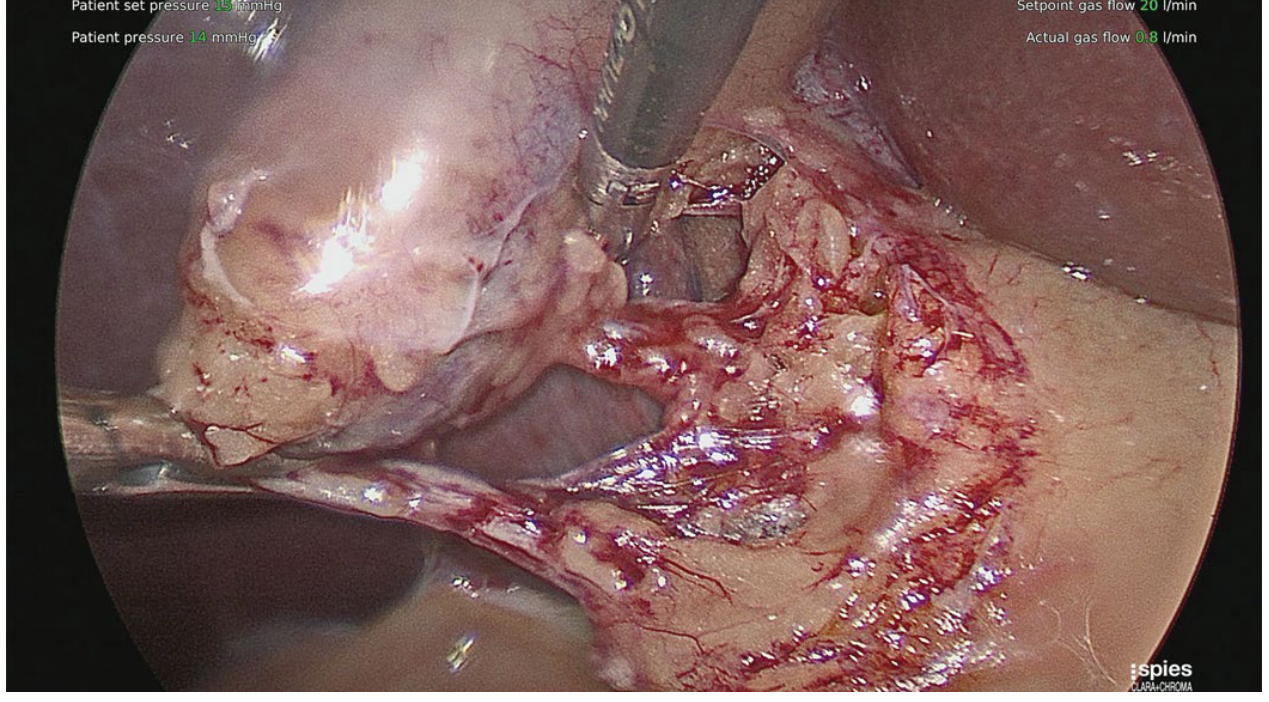
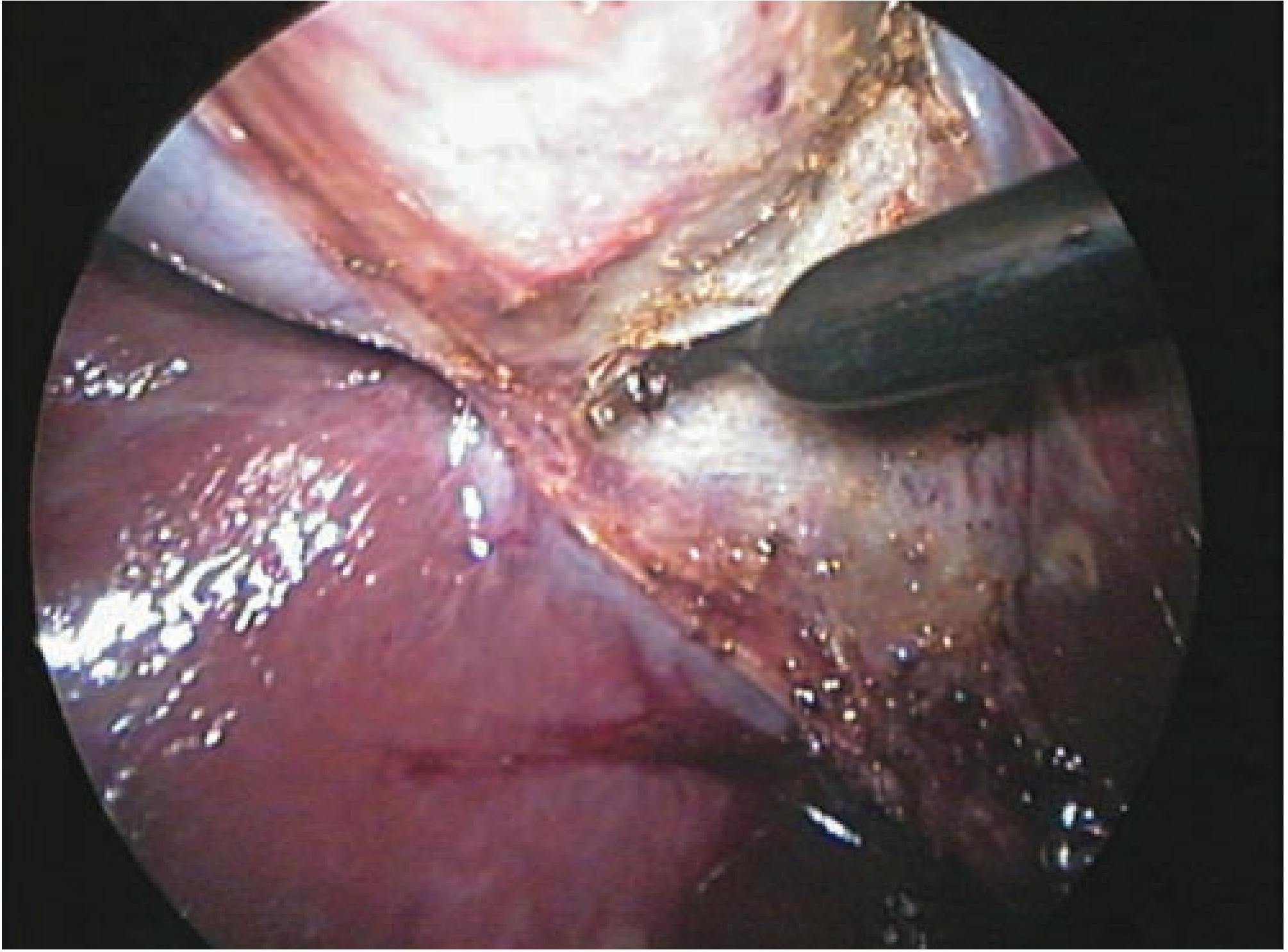
Step 3: Dissection of the Hepatocystic Triangle
Using hook electrocautery or a Maryland dissector via the epigastric port, the surgeon strips the peritoneum and fibrofatty tissue from the hepatocystic triangle, working on the gallbladder wall (not in the triangle itself). The critical principle from Maingot's: "Stay on the gallbladder, stay on the gallbladder, and stay on the gallbladder" - the most effective strategy to avoid CBD or right hepatic artery injury.
The Critical View of Safety (CVS)
The CVS, described by Strasberg, is the gold standard for safe identification of cystic structures before clipping. It requires all three of the following criteria to be met:
- The hepatocystic triangle is cleared of fat and fibrous tissue
- The lower one-third of the gallbladder is separated from the liver bed to expose the cystic plate
- Two and only two structures are seen entering the gallbladder
Both the anterior and posterior views must be confirmed (the "doublet view").
If CVS cannot be achieved safely, a "bail-out" strategy must be used: subtotal cholecystectomy (leaving the posterior wall of the gallbladder in the fossa), conversion to open, cholecystostomy tube, or calling for intraoperative assistance.
Clipping and Division
Once CVS is achieved:
- Two clips proximally (staying side) on both the cystic duct and cystic artery
- One clip distally (specimen side) on each structure
- Divide with laparoscopic scissors between the clips
When dividing the cystic duct, inspect the cut end: if two lumens are visible, a structure other than just the cystic duct may have been ligated - stop immediately.
Gallbladder Dissection from the Liver Bed
Using hook electrocautery via the epigastric port, the gallbladder is dissected off the liver fossa from infundibulum to fundus. The midclavicular grasper moves progressively cephalad to maintain countertraction. The venous drainage of the gallbladder flows directly into the liver bed through venuoles, so excellent hemostasis is required.
Specimen Extraction
The gallbladder is placed in an entrapment bag (especially if perforated intraoperatively or if stone burden is large), then extracted through the umbilical port (no muscle layers anterior to fascia; easier extension if needed). If stones prevent extraction, suction aspiration of bile and stone crushing with forceps can help. The umbilical fascial defect is closed with absorbable suture.
Intraoperative Cholangiography (IOC) and Fluorescent Cholangiography
IOC is performed selectively (not routinely per Tokyo Guidelines) by passing a catheter into the cystic duct via a ductotomy and injecting water-soluble contrast under fluoroscopy. Indications include:
- Gallstone pancreatitis
- Anomalous or unclear biliary anatomy
- Suspected choledocholithiasis
ICG fluorescent cholangiography (near-infrared light) is now available in most centers and provides real-time visualization of the CBD and cystic duct, though tissue thickness and inflammation limit penetration. - Sabiston, p. 1839
Conversion to Open
Conversion is not a complication - it is sound surgical judgment. Indications include:
- Inability to achieve CVS safely
- Uncontrolled bleeding
- Dense adhesions or severe inflammation obscuring anatomy
- Bile duct injury recognized intraoperatively
- Mirizzi syndrome
Late conversion is associated with higher rates of bile duct injury - convert early rather than persistently struggling laparoscopically.
Key Safety Principles Summary
| Principle | Rationale |
|---|---|
| Always achieve CVS before clipping | Prevents misidentification of CBD as cystic duct |
| Stay on the gallbladder wall | Avoids CBD and right hepatic artery injury |
| Confirm both anterior + posterior CVS views | Rules out posterior anomalous ducts |
| Use IOC or ICG when anatomy is unclear | Real-time roadmap of biliary tree |
| Convert early, not late | Late conversion has higher BDI rates |
| One clip on specimen side, two on staying side | Prevents leakage from proximal stump |
Sources: Sabiston Textbook of Surgery 21e, p. 1838-1840 | Maingot's Abdominal Operations, Ch. 48 | Fischer's Mastery of Surgery 8e, Ch. 166 | Current Surgical Therapy 14e, p. 506
This is a shared conversation. Sign in to Orris to start your own chat.