Epistaxix
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of epistaxis (nosebleed) based on authoritative sources.
Epistaxis
Definition & Epidemiology
Epistaxis is bleeding from the nasal cavity. It is a common otolaryngologic problem with a bimodal age distribution — peaks in children and in the elderly. Incidence is higher in winter months and colder climates, likely due to dry indoor heating that desiccates nasal mucosa. Death from epistaxis is exceedingly rare, though it can be distressing to patients.
Anatomy & Classification
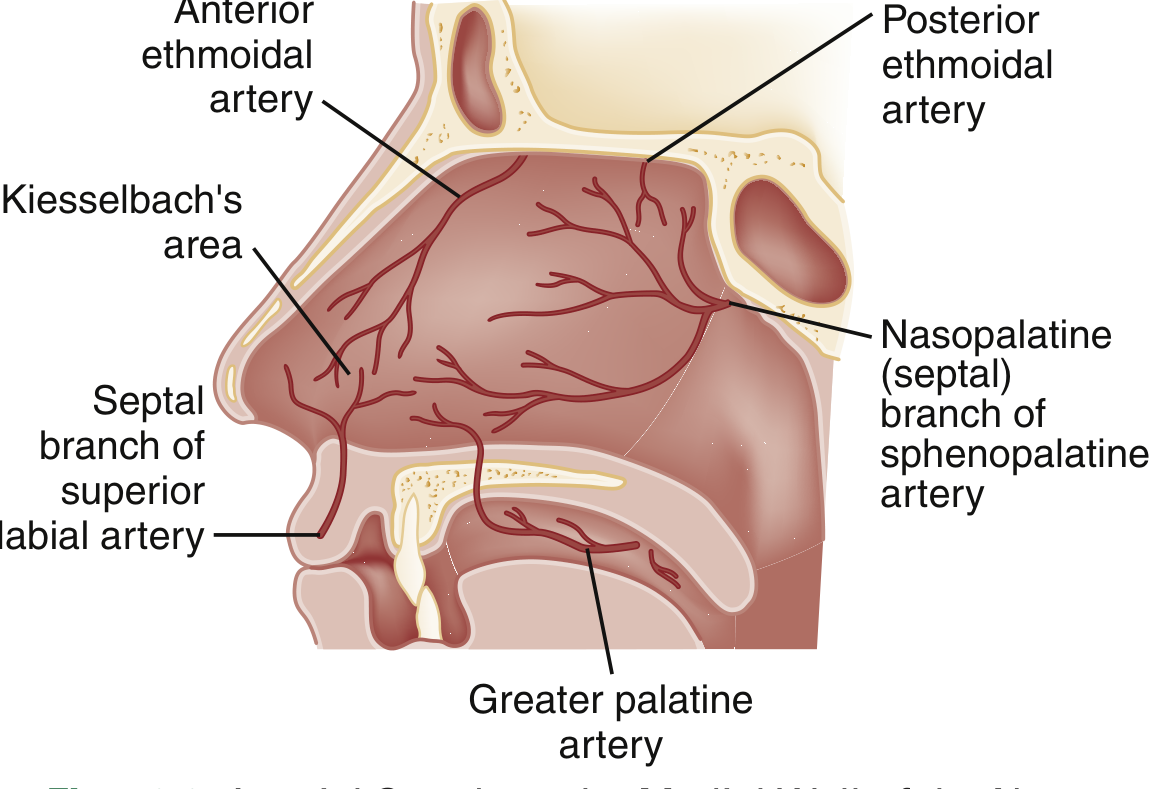
Three arterial systems supply the nasal cavity:
- Sphenopalatine artery — supplies the turbinates, meatus, and posterior/inferior septum; implicated in most severe posterior epistaxis
- Anterior and posterior ethmoidal arteries (from the ophthalmic branch of the internal carotid) — supply the superior mucosa
- Superior labial branch of the facial artery — supplies the anterior mucosal septum
Anterior epistaxis (~90% of cases): Arises from Kiesselbach's plexus on the anteroinferior nasal septum. Typically unilateral and self-limiting.
Posterior epistaxis (~10% of cases): More severe, occurs predominantly in older adults with multiple comorbidities; harder to visualize and manage.
Causes
| Category | Examples |
|---|---|
| Local/Spontaneous | Dry mucosa, nose picking, trauma, septal deviation |
| Vascular | Hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease) |
| Systemic | Coagulopathy, anticoagulants, antiplatelet drugs |
| Neoplastic | Nasal/nasopharyngeal tumors |
| Hypertension | Causation not proven, but persistent hypertension associated with prolonged bleeding |
Clinical Assessment
- Airway, breathing, circulation — address hemodynamic instability first
- History: timing, frequency, severity; trauma; medications (anticoagulants, NSAIDs, aspirin); bleeding disorders
- Examination: have the patient blow the nose to clear clots, then apply bilateral pressure on the cartilaginous nose for 10–15 minutes
- Administer 2 sprays of 0.05% oxymetazoline into the affected naris before applying pressure to optimize hemostasis and facilitate inspection
- Identify the bleeding site to guide cautery
Management
Anterior Epistaxis
Step-wise approach:
- Direct pressure (10–15 min on cartilaginous nose) ± nose clip (superior to manual pressure alone)
- Topical vasoconstrictors — oxymetazoline 0.05%
- Chemical cautery — silver nitrate sticks applied to the bleeding point; reduces recurrence risk
- Nasal packing — anterior packing if cautery insufficient; prophylactic antibiotics are not routinely recommended with anterior packing
- Tranexamic acid — effective adjunct (topical or systemic); decreases immediate and delayed rebleeding
Posterior Epistaxis
- Requires specialized packing techniques (posterior pack or balloon catheter)
- Inpatient monitoring required — posterior packs can cause hypoxia/cardiac events, especially in elderly
- Consider ENT consultation
Refractory Epistaxis
- Endovascular embolization: Superselective catheterization of the internal maxillary and facial arteries; success rates 91–97%, complication rates 0–3%
- Surgical ligation of the internal maxillary arteries or anterior ethmoidal artery
- Bilateral selective internal and external carotid angiography should be performed to identify feeders
Special Considerations
- Anticoagulated patients: Higher risk of recurrence; consider reversing anticoagulation if clinically appropriate
- Hereditary hemorrhagic telangiectasia (HHT/Osler-Weber-Rendu): Recurrent epistaxis from mucosal telangiectasias — requires specialist management (laser, embolization, bevacizumab in severe cases)
- Hypertension: Not causally linked to epistaxis, but elevated BP at presentation may perpetuate bleeding — treat if severely elevated
Sources: Rosen's Emergency Medicine, pp. 913–920 | Cummings Otolaryngology Head and Neck Surgery | Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.