Give a diagramatic or interpreted overview of Prevention of CHD according to Park's Preventive medicine book
Park's Preventive and Social Medicine CHD prevention levels primary secondary tertiary
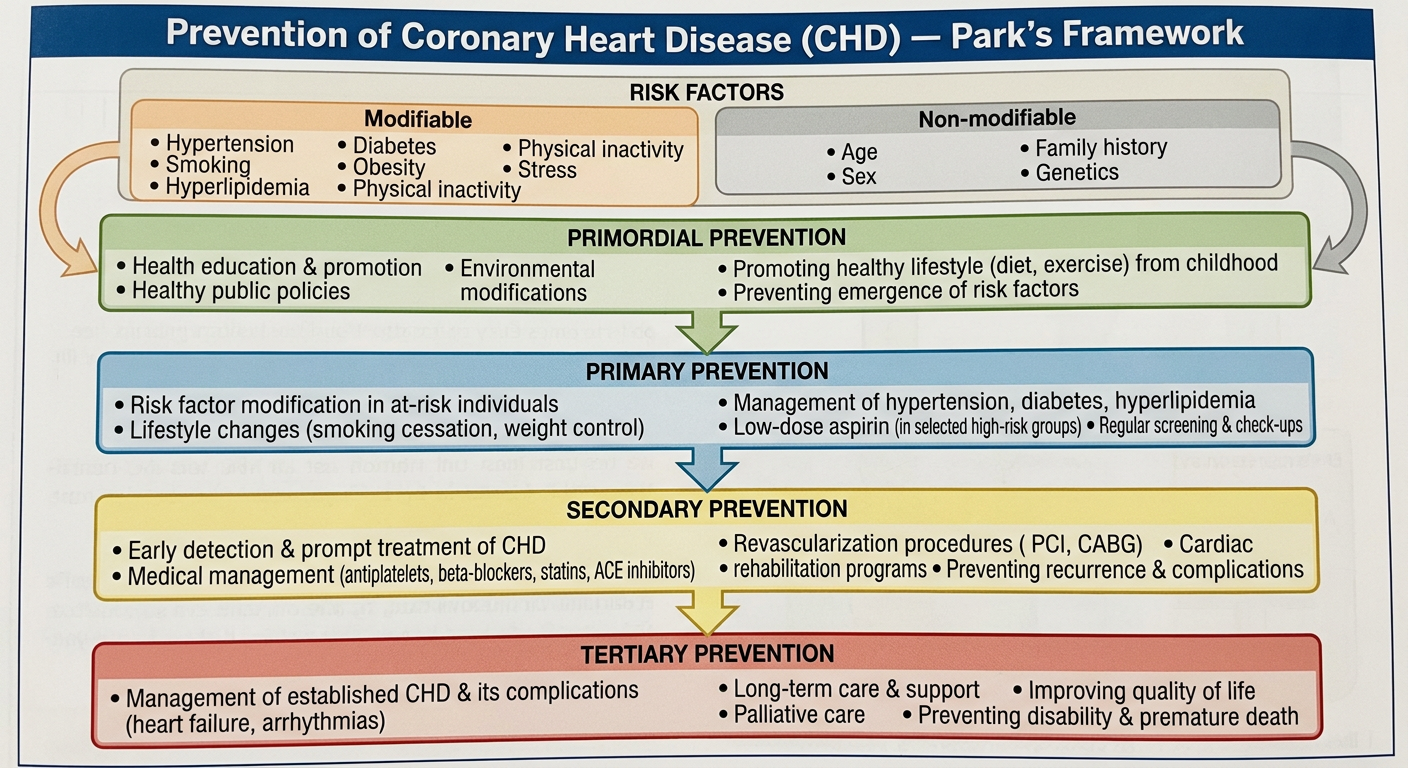
A detailed medical educational diagram titled "Prevention of Coronary Heart Disease (CHD) — Park's Framework" showing four levels of prevention arranged vertically: Primordial Prevention, Primary Prevention, Secondary Prevention, and Tertiary Prevention. Each level has its own color-coded box with bullet points listing specific measures. Include risk factors section showing modifiable (hypertension, smoking, hyperlipidemia, diabetes, obesity, physical inactivity, stress) and non-modifiable (age, sex, family history, genetics). Use arrows and clean flowchart style. Professional medical textbook diagram aesthetic with clear hierarchy and readable text.
Prevention of Coronary Heart Disease (CHD) — Park's Framework
Risk Factors for CHD
Non-Modifiable
| Factor | Details |
|---|---|
| Age | Risk rises after 45 (men), 55 (women) |
| Sex | Males at higher risk; women's risk rises post-menopause |
| Family history | First-degree relatives with premature CHD |
| Genetic factors | Familial hypercholesterolaemia, etc. |
Modifiable (Major)
| Factor | Target |
|---|---|
| Hypertension | BP < 130/80 mmHg |
| Hyperlipidaemia | LDL-C reduction; total cholesterol < 200 mg/dL |
| Cigarette smoking | Complete cessation |
| Diabetes mellitus | HbA1c < 7%; glycaemic control |
| Obesity | BMI 18.5–24.9; waist < 90 cm (M), < 80 cm (F) |
| Physical inactivity | ≥150 min/week moderate activity |
| Psychosocial stress | Type A behaviour, depression |
Modifiable (Minor/Emerging)
- Hypertriglyceridaemia, Low HDL, Homocysteinaemia, CRP elevation, Fibrinogen, Lipoprotein(a), Oral contraceptive use
The Four Levels of Prevention
🔵 Primordial Prevention
Targets the pre-risk stage — preventing the emergence of risk factors themselves in the population
- National/Community level policies: food labelling, salt reduction in processed foods, tobacco control legislation (FCTC), trans-fat bans
- Health education: promotion of healthy diet, physical activity, non-smoking habits from childhood
- School-based programmes: nutrition education, physical fitness curricula
- Urban planning: creating environments conducive to walking, cycling
- Social/economic development to reduce poverty and improve living standards
Concept: Prevention is directed at social, environmental, and economic conditions that allow risk factors to arise — not at the individual risk factors themselves.
🟢 Primary Prevention
Targets individuals at risk (risk factors present, no disease yet) — preventing CHD from ever occurring
- Health education about CHD risk factors
- Promote balanced diet low in saturated fats, trans fats, salt, and refined sugars
- Encourage regular aerobic exercise (brisk walking, cycling, swimming)
- Weight management & avoidance of central obesity
- Stress management; work–life balance
- Anti-tobacco programmes; smoking cessation support (NRT, counselling)
- Control of hypertension (lifestyle + pharmacotherapy where indicated)
- Control of hyperlipidaemia (statins in high-risk individuals, diet)
- Glycaemic control in diabetes
- Aspirin in selected high-risk individuals (as per guidelines)
- Screening and referral programmes for risk factor detection
Key principle: Even a modest reduction in population-wide risk factor levels produces large absolute reductions in CHD incidence (Rose's strategy).
🟡 Secondary Prevention
Targets those with established CHD — halting progression, preventing recurrence and complications
- ECG, stress testing, coronary angiography
- Screening of high-risk asymptomatic individuals
- Thrombolysis/primary PTCA/CABG for acute MI
- Antiplatelet therapy (aspirin + clopidogrel)
- Beta-blockers (post-MI cardioprotection)
- ACE inhibitors/ARBs (post-MI, HF with reduced EF)
- High-intensity statins (LDL-C ≥ 50% reduction)
- Nitrates for angina
- Rehabilitation post-MI
- Prevent heart failure progression
- Prevent arrhythmias (ICD implantation where indicated)
- Prevent re-infarction through strict risk factor control
🔴 Tertiary Prevention
Targets those with severe/complicated CHD — restoring maximal function and preventing further disability
- Cardiac rehabilitation programme (Phase I–III):
- Phase I: In-hospital mobilisation
- Phase II: Supervised outpatient exercise
- Phase III: Long-term community maintenance
- Psychosocial rehabilitation; management of depression and anxiety
- Vocational rehabilitation — return to work
- Continued pharmacotherapy adherence (statins, antiplatelets, beta-blockers, ACEi)
- Lifestyle modification reinforcement
- Regular follow-up and monitoring
- Management of end-stage heart failure (diuretics, device therapy, transplant evaluation)
- Palliative care for irreversible cardiac disability
Summary Diagram (Textual)
NATURAL HISTORY OF CHD
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
No risk Risk factors Subclinical Clinical Complications
factors emerging CHD CHD / Death
│ │ │ │ │
▼ ▼ ▼ ▼ ▼
┌──────────┐ ┌───────────┐ ┌───────────┐ ┌────────────┐ ┌──────────┐
│PRIMORDIAL│ │ PRIMARY │ │ SECONDARY │ │ SECONDARY │ │TERTIARY │
│Prevention│ │Prevention │ │Prevention │ │Prevention │ │Prevention│
│(pop-level│ │(risk factor│ │(early Dx &│ │(treatment) │ │(rehab & │
│ policies)│ │ control) │ │ screening)│ │ │ │ palliate)│
└──────────┘ └───────────┘ └───────────┘ └────────────┘ └──────────┘
↑ ↑ ↑ ↑ ↑
Leavell & Leavell & Leavell & Leavell & Leavell &
Clark Level Clark Level 1 Clark Level 2 Clark Level 3 Clark Level 4/5
(added (Health (Early diag. (Treatment (Rehab)
by WHO) Promo + + Rx) + Disab.
Specific limit.)
Protection)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Key Park's Concepts in CHD Prevention
| Concept | Relevance |
|---|---|
| Leavell & Clark's levels | 5 levels mapped to natural history of disease |
| Primordial prevention | Added specifically for NCDs like CHD by WHO/Park |
| Rose's Population Strategy | Small shift in population BP/cholesterol = large CHD reduction |
| High-Risk Strategy | Target intensive prevention at those with most risk |
| Epidemiological triad | Host (genetics, age) + Agent (atherogenic factors) + Environment (diet, stress, smoking culture) |
| Web of causation | CHD is multi-factorial; no single cause — prevention must be multi-pronged |
Note: Park's Textbook of Preventive and Social Medicine (24th ed.) places CHD prevention within the broader framework of non-communicable disease (NCD) control, emphasising that primordial prevention — absent from earlier Leavell & Clark schemas — is the most impactful level for population-wide CHD burden reduction, as it prevents the very emergence of risk factors.