Diabetes
Reading File
search_medical_text
diabetes mellitus types classification pathophysiology
search_medical_text
diabetes mellitus diagnosis management treatment complications
GradeResponse
GradeResponse
Diabetes Mellitus
Diabetes mellitus is a group of metabolic disorders characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both (Laboratory Analysis in the Diagnosis and Management of Diabetes Mellitus, p. 1).
Classification
| Type | Mechanism | Key Features |
|---|---|---|
| Type 1 DM | Autoimmune destruction of pancreatic β-cells | Absolute insulin deficiency; insulin required for survival |
| Type 2 DM | Insulin resistance + inadequate insulin secretion | Most common form; often manageable with lifestyle/oral agents early on |
| Gestational DM (GDM) | Resembles T2DM; develops during ~17% of pregnancies | Usually remits after delivery; major risk factor for future T2DM |
| Other specific types | Monogenic (MODY), pancreatic disease, drug-induced, etc. | Classified per 2014 revised criteria |
Pathophysiology
- Type 1: Autoimmune destruction of islet β-cells → no insulin synthesis or secretion → absolute dependence on exogenous insulin.
- Type 2: Peripheral insulin resistance (especially in muscle, liver, and fat) combined with progressive β-cell dysfunction → relative insulin deficiency. Often driven by obesity, physical inactivity, and genetic predisposition.
Diagnosis
Diagnosis is based on one of the following criteria (ADA Standards):
| Criterion | Threshold |
|---|---|
| Fasting plasma glucose (FPG) | ≥ 126 mg/dL (7.0 mmol/L) |
| 2-hour plasma glucose (75g OGTT) | ≥ 200 mg/dL (11.1 mmol/L) |
| HbA1c | ≥ 6.5% (48 mmol/mol) |
| Random plasma glucose + symptoms | ≥ 200 mg/dL (11.1 mmol/L) |
Prediabetes: FPG 100–125 mg/dL, 2-hr glucose 140–199 mg/dL, or HbA1c 5.7–6.4%.
Management
Management is individualized and includes (Eye Care of the Patient with Diabetes Mellitus, p. 23):
1. Lifestyle Modifications
- Weight reduction (especially in T2DM)
- Regular aerobic exercise
- Medical nutrition therapy (carbohydrate monitoring, reduced saturated fat)
2. Glucose-Lowering Pharmacotherapy
Type 2 DM (stepwise approach):
- Metformin — first-line; reduces hepatic glucose output
- GLP-1 receptor agonists (e.g., semaglutide, liraglutide) — weight loss, CV benefit
- SGLT-2 inhibitors (e.g., empagliflozin, dapagliflozin) — renal/CV protection
- DPP-4 inhibitors (e.g., sitagliptin) — weight-neutral
- Sulfonylureas (e.g., glipizide) — inexpensive; hypoglycemia risk
- Insulin — when oral agents insufficient
Type 1 DM:
- Basal-bolus insulin regimen (e.g., insulin glargine + rapid-acting analogs)
- Continuous glucose monitoring (CGM) + insulin pump (CSII) for eligible patients
3. Cardiovascular & Metabolic Risk Reduction
- Blood pressure target: typically < 130/80 mmHg
- Statin therapy for most adults with diabetes
- Antiplatelet therapy in select high-risk patients
4. Glycemic Targets
- HbA1c < 7% for most non-pregnant adults
- Less stringent (< 8%) for elderly, limited life expectancy, or hypoglycemia-prone patients
Complications
Microvascular
| Complication | Key Points |
|---|---|
| Diabetic nephropathy | Leading cause of end-stage renal disease; ACE inhibitors/ARBs are nephroprotective |
| Diabetic retinopathy | Leading cause of new blindness in working-age adults; annual fundus exam required |
| Diabetic neuropathy | Distal symmetric polyneuropathy most common; autonomic neuropathy also occurs |
Macrovascular
- Coronary artery disease, stroke, and peripheral artery disease — 2–4× higher risk than general population
- Atherosclerosis accelerated by hyperglycemia, dyslipidemia, and hypertension
Acute
- Diabetic ketoacidosis (DKA) — primarily T1DM; high anion gap metabolic acidosis, hyperglycemia, ketonemia
- Hyperosmolar hyperglycemic state (HHS) — primarily T2DM; extreme hyperglycemia (>600 mg/dL), minimal ketosis
- Hypoglycemia — most common acute complication of treatment
Monitoring
- HbA1c: every 3 months until at goal, then every 6 months
- Self-monitoring of blood glucose (SMBG) or CGM
- Annual: urine albumin-to-creatinine ratio, eGFR, lipid panel, foot exam, eye exam
- Blood pressure at every visit
Special Populations
- Pregnancy: tight glycemic control critical; insulin preferred (metformin/glyburide used in some guidelines for GDM)
- Elderly: hypoglycemia avoidance prioritized; simpler regimens preferred
- CKD: dose-adjust or avoid certain agents (e.g., metformin contraindicated with eGFR < 30)
Do you have a specific aspect of diabetes you'd like to explore further — a particular type, complication, drug class, or patient scenario?
Back pain with tingling sensation to legs differential diagnosis
Reading File
search_medical_text
back pain with leg tingling radiculopathy differential diagnosis
search_medical_text
lumbar spinal stenosis cauda equina herniated disc clinical features
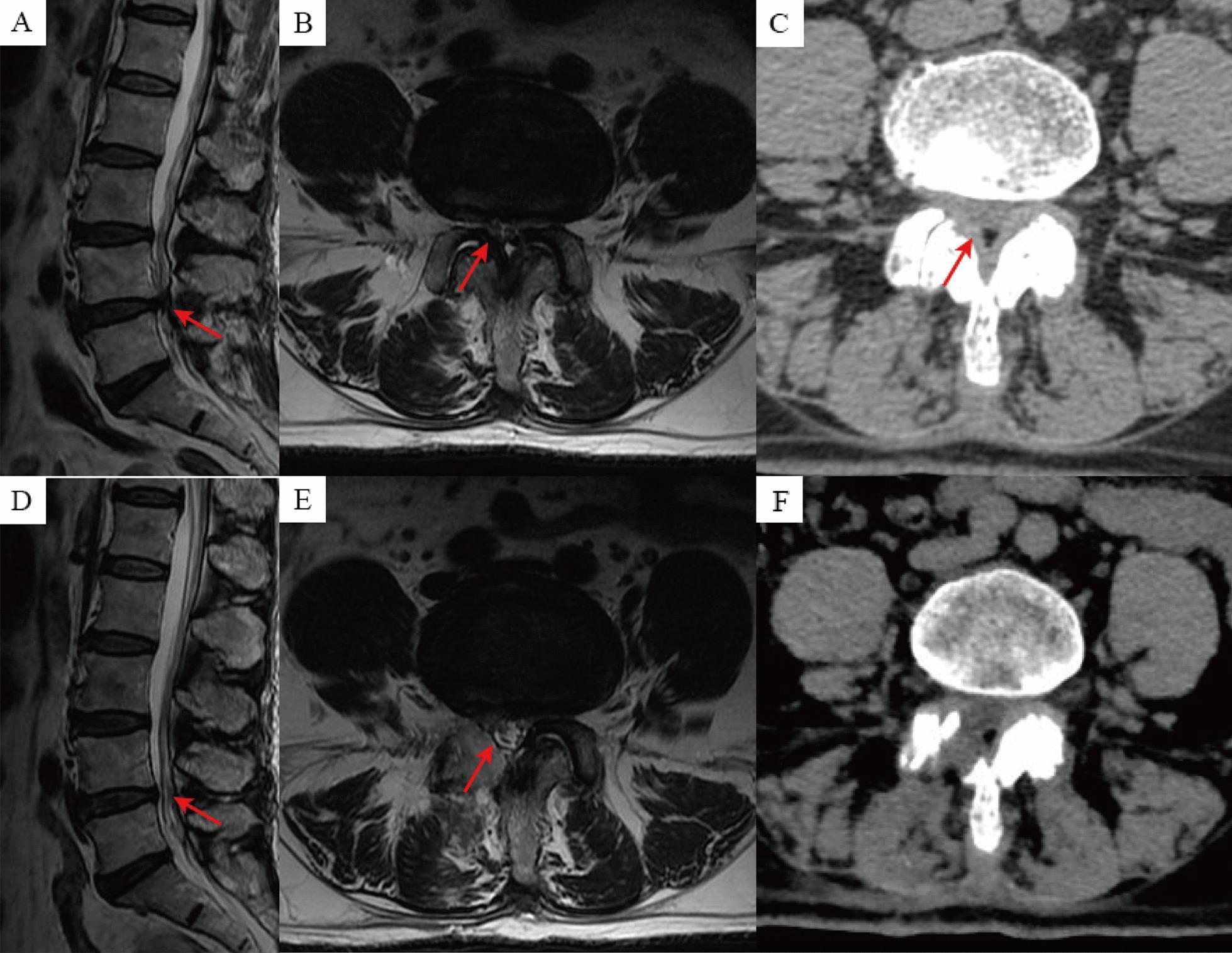
search_medical_image
lumbar disc herniation spinal stenosis MRI imaging
GradeResponse
GradeResponse
GradeResponse
Back Pain with Tingling Sensation to the Legs — Differential Diagnosis
Back pain radiating to the legs with tingling (paresthesia) is a classic presentation of nerve involvement. The differential is broad, spanning structural, neurological, vascular, and systemic causes.
Structured Differential Diagnosis
1. Lumbar Disc Herniation / Radiculopathy (Most Common)
- Mechanism: Herniated nucleus pulposus compresses a nerve root, most often at L4-L5 or L5-S1.
- Presentation: Sharp/shooting back pain radiating down the leg in a dermatomal pattern; tingling, numbness, or weakness in the corresponding territory. "Sciatica" refers specifically to posteriorly-radiating leg pain in an L5/S1 distribution.
- Key finding: Positive straight leg raise (SLR) test.
- Prognosis: Generally favorable — two-thirds of herniated discs show spontaneous regression on imaging over 6 months (Harrison's Principles of Internal Medicine, 21st ed., p. 622).
2. Lumbar Spinal Stenosis
- Mechanism: Narrowing of the spinal canal (due to osteophytes, ligamentum flavum hypertrophy, facet joint enlargement) compresses the thecal sac and nerve roots.
- Presentation: Bilateral leg pain, tingling, and weakness — classically neurogenic claudication (symptoms worsen with walking/standing and improve with sitting/forward flexion).
- Demographics: Most common cause of spinal surgery in patients over 65 years (Epidural Interventions in the Management of Chronic Spinal Pain, p. 33).
- Imaging: MRI shows reduced dural sac cross-sectional area; CT shows bony canal narrowing.
3. Cauda Equina Syndrome (Surgical Emergency)
- Mechanism: Massive central disc herniation or other mass compresses the cauda equina nerve roots below L1-L2.
- Presentation: Bilateral leg weakness/tingling, saddle anesthesia (perianal numbness), urinary retention or incontinence, and fecal incontinence.
- Action: Requires urgent MRI and emergent surgical decompression. Do not miss.
4. Piriformis Syndrome
- Mechanism: Spasm or hypertrophy of the piriformis muscle compresses the sciatic nerve in the gluteal region.
- Presentation: Buttock pain with radiation down the posterior leg mimicking disc-related sciatica; no true spinal pathology on MRI.
- Key finding: Pain reproduced by the FAIR test (flexion, adduction, internal rotation of the hip).
5. Spondylolisthesis
- Mechanism: Anterior displacement of one vertebral body over another (commonly L4 over L5), causing nerve root or canal compression.
- Presentation: Low back pain, leg tingling/radiculopathy, and sometimes neurogenic claudication.
- Imaging: Plain X-ray (lateral view) shows "step-off" deformity; MRI for neural involvement.
6. Foraminal Stenosis
- Mechanism: Narrowing of the intervertebral foramen (due to osteophytes or disc degeneration) compresses the exiting nerve root.
- Presentation: Unilateral dermatomal pain and paresthesia; often indistinguishable clinically from disc herniation.
7. Peripheral Neuropathy (e.g., Diabetic)
- Mechanism: Systemic nerve damage (metabolic, toxic, autoimmune).
- Presentation: Bilateral, symmetric tingling/burning in a stocking distribution; associated with back pain if there is concomitant spinal pathology. Note: in diabetic patients, both radiculopathy and peripheral neuropathy may coexist.
- Distinguishing feature: No single dermatomal pattern; no positive SLR; nerve conduction studies abnormal.
8. Vascular Claudication
- Mechanism: Peripheral artery disease (PAD) causing ischemia to the legs.
- Presentation: Leg pain/cramping with exertion; tingling possible; improves with rest (not with positional change as in neurogenic claudication).
- Key finding: Reduced or absent peripheral pulses; ankle-brachial index (ABI) < 0.9.
9. Spinal Tumors (Primary or Metastatic)
- Mechanism: Epidural or intradural mass compresses neural structures.
- Red flags: Pain worse at night/at rest, unexplained weight loss, history of malignancy, age > 50.
- Imaging: MRI with contrast is the gold standard.
10. Vertebral Fracture (Osteoporotic or Traumatic)
- Mechanism: Compression fracture (particularly in osteoporotic elderly patients) may cause retropulsion of bone fragments into the canal.
- Presentation: Acute severe back pain after minimal trauma; neurological signs if the canal is compromised.
11. Epidural Abscess or Discitis/Osteomyelitis (Infection)
- Red flags: Fever, IV drug use, recent spinal procedure, immunocompromised state.
- Presentation: Progressive back pain + neurological deficit; constitutional symptoms.
- Emergency: Requires urgent MRI and often surgical drainage + antibiotics.
Comparison Table
| Condition | Pain Character | Laterality | Aggravating | Relieving | Key Sign/Test |
|---|---|---|---|---|---|
| Disc herniation | Sharp, shooting | Unilateral | Sitting, cough/sneeze | Walking, lying flat | (+) SLR |
| Spinal stenosis | Aching, claudicant | Bilateral | Walking, standing | Sitting, flexion | Neurogenic claudication |
| Cauda equina syndrome | Severe bilateral | Bilateral | — | — | Saddle anesthesia, urinary retention |
| Piriformis syndrome | Buttock → posterior leg | Unilateral | Sitting, hip IR | Stretching | (+) FAIR test |
| Vascular claudication | Cramping | Bilateral | Exercise | Rest | Reduced pulses, low ABI |
| Peripheral neuropathy | Burning, symmetric | Bilateral | Night, rest | — | Stocking distribution |
| Spinal tumor | Constant, nocturnal | Variable | Rest, night | — | Weight loss, age > 50 |
Red Flags Requiring Urgent Workup
- Cauda equina symptoms (saddle anesthesia, bladder/bowel dysfunction) → emergent MRI
- Fever + back pain → rule out epidural abscess
- History of cancer → rule out metastasis
- Progressive neurological deficit
- Pain unrelenting at rest or at night
Diagnostic Approach
- History: Onset, radiation pattern, aggravating/relieving factors, bowel/bladder function, systemic symptoms
- Neurological exam: Motor strength, sensation, reflexes, SLR, gait
- Imaging:
- MRI lumbar spine — preferred for soft tissue, disc, and neural structures
- X-ray — for fracture, alignment, spondylolisthesis
- CT — bony detail when MRI is unavailable
- Ancillary: EMG/NCS (to differentiate radiculopathy from peripheral neuropathy); ABI (if vascular claudication suspected); ESR/CRP, blood cultures (if infection/tumor suspected)
Would you like a deeper dive into any specific condition, its management, or workup algorithm?
This is a shared conversation. Sign in to Orris to start your own chat.