help me learn anatomy for my medical school exam start with lower limb
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything needed for a thorough, visually-rich study guide. Here is your complete Lower Limb anatomy study guide from Gray's Anatomy for Students:
Lower Limb Anatomy - Medical School Study Guide
Source: Gray's Anatomy for Students
1. Regions Overview
The lower limb is divided into four regions based on the bounding joints:
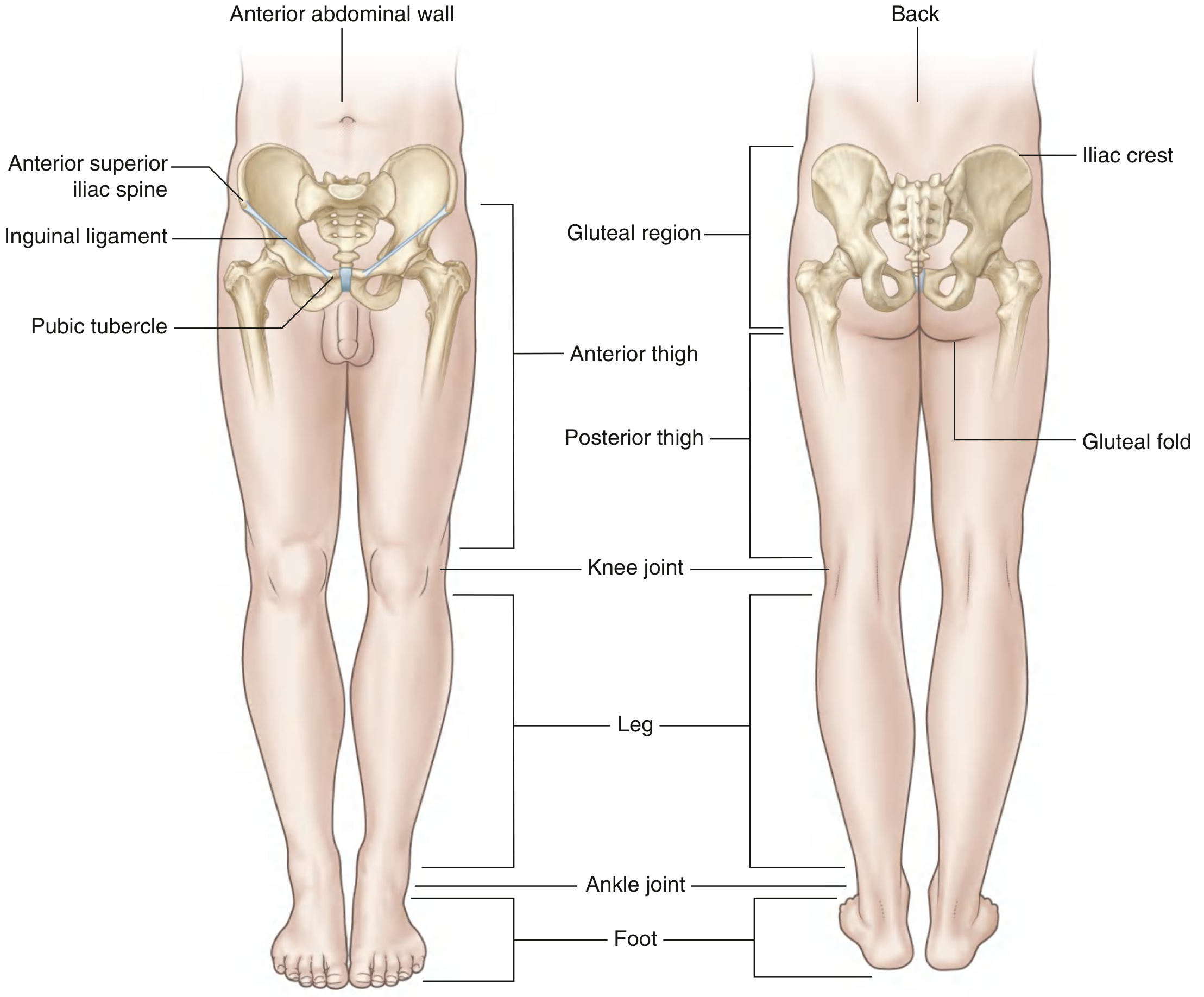
| Region | Boundaries |
|---|---|
| Gluteal region | Posterolateral; iliac crest → gluteal fold |
| Thigh | Anterior: inguinal ligament → knee; Posterior: gluteal fold → knee |
| Leg | Knee joint → ankle joint |
| Foot | Distal to ankle joint |
Key transition zones (learn these - they come up in clinicals):
- Femoral triangle - proximal thigh, below inguinal ligament; where major vessels/nerve enter the limb
- Popliteal fossa - diamond-shaped, posterior to knee; vessels/nerves pass thigh → leg
- Tarsal tunnel - posteromedial ankle; canals formed by bone + flexor retinaculum for tendons, vessels, nerves passing to the foot
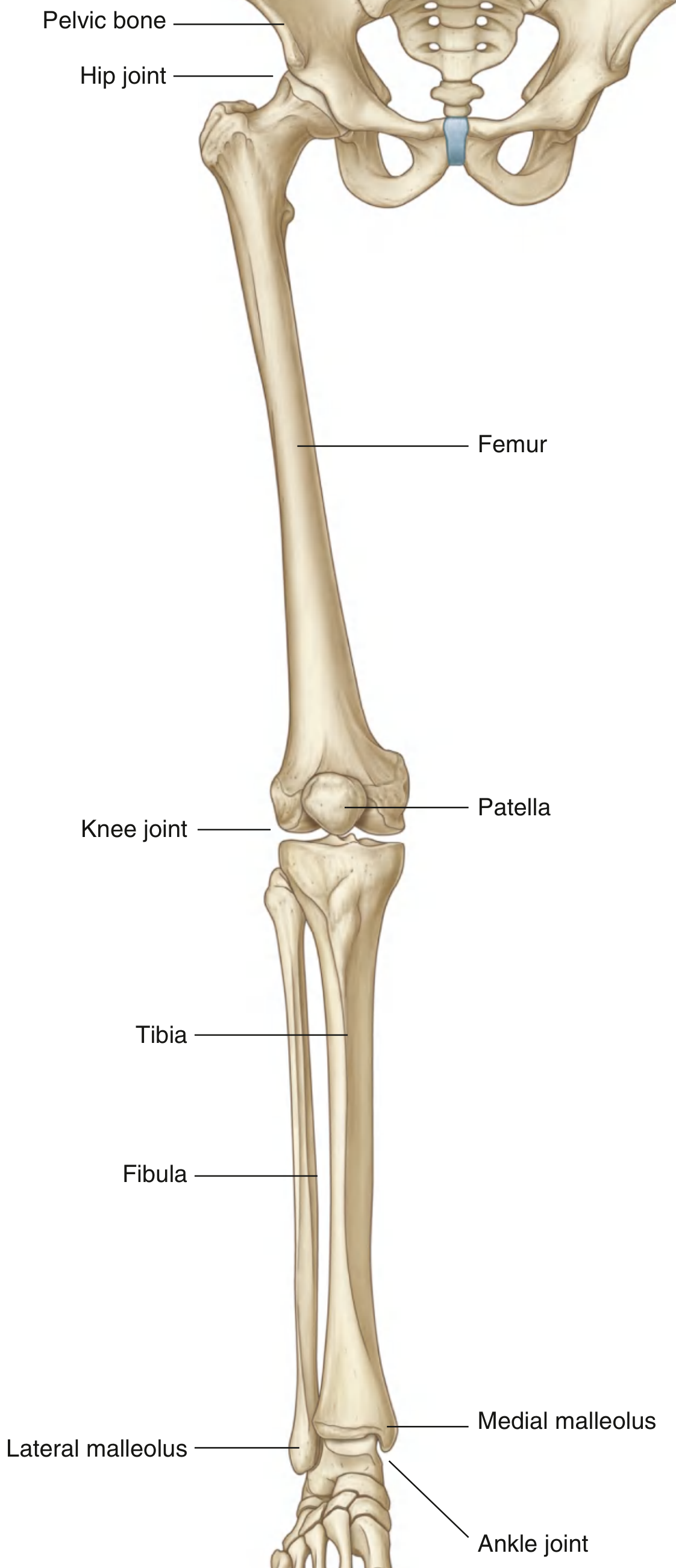
2. Bones and Joints
Pelvic Bone (three fused parts)
- Ilium - fan-shaped; iliac crest runs from ASIS (anterior superior iliac spine) → PSIS (posterior superior iliac spine)
- Ischium - includes ischial tuberosity (origin of hamstrings); greater/lesser sciatic notches
- Pubis - pubic symphysis anteriorly
Gluteal lines on the ilium (exam favourite):
- Inferior gluteal line - rectus femoris attaches between this and acetabulum margin
- Anterior gluteal line - gluteus minimus between inferior and anterior lines
- Posterior gluteal line - gluteus medius between anterior and posterior lines; gluteus maximus posterior to the posterior line
Femur
- Shaft angles 7 degrees from vertical (brings knees toward midline)
- Linea aspera - major posterior ridge; major muscle attachment site
- Proximal linea aspera divides into: pectineal line (medial) and gluteal tuberosity (lateral, for gluteus maximus)
- Greater trochanter + lesser trochanter separated by intertrochanteric line (anterior) and intertrochanteric crest (posterior, has the quadrate tubercle for quadratus femoris)
Clinic: Femoral neck fractures interrupt the arterial ring (medial + lateral circumflex femoral arteries) supplying the femoral head - risk of avascular necrosis is the key complication.
Leg Bones
- Tibia - weight-bearing; medial malleolus distally
- Fibula - non-weight-bearing; lateral malleolus distally
- Patella - sesamoid bone in quadriceps tendon
Foot Bones
- 7 tarsal bones (two rows + intermediate medial bone): calcaneus, talus, navicular, cuboid, 3 cuneiforms
- 5 metatarsals + phalanges (3 each, except great toe which has 2)
- Arches: longitudinal (medial higher than lateral) and transverse - maintained by ligaments, tendons, bone shape
3. Muscular Compartments
Gluteal Region Muscles (Table)
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| Gluteus maximus | Ilium (post. to posterior gluteal line), sacrum, coccyx | Gluteal tuberosity of femur + iliotibial tract | Inferior gluteal (L5-S2) | Extends + laterally rotates hip |
| Gluteus medius | Between anterior/posterior gluteal lines | Greater trochanter (lateral surface) | Superior gluteal (L4-S1) | Abducts hip; prevents pelvic drop during gait |
| Gluteus minimus | Between inferior/anterior gluteal lines | Greater trochanter (anterior surface) | Superior gluteal (L4-S1) | Abducts + medially rotates hip |
| Tensor fasciae latae | ASIS + outer iliac crest | Iliotibial tract | Superior gluteal (L4-S1) | Stabilizes knee via IT band |
| Piriformis | Anterior surface of sacrum | Superior border of greater trochanter | S1, S2 | Laterally rotates extended hip; abducts flexed hip |
| Obturator internus | Inner surface of obturator membrane | Greater trochanter (medial surface) | Nerve to OI (L5-S1) | Laterally rotates hip |
| Gemellus superior/inferior | Ischial spine / ischial tuberosity | Greater trochanter (with OI) | Nerve to OI / nerve to QF | Laterally rotates hip |
| Quadratus femoris | Ischial tuberosity | Quadrate tubercle (intertrochanteric crest) | Nerve to QF (L5-S1) | Laterally rotates hip |
Trendelenburg test: If gluteus medius is weak (superior gluteal nerve injury), the pelvis drops on the contralateral side when standing on the affected leg.
Thigh Compartments
Anterior compartment (femoral nerve, L2-L4):
- Quadriceps femoris: rectus femoris + vastus lateralis, medialis, intermedius → extend knee; rectus also flexes hip
- Sartorius: longest muscle in body; ASIS → medial tibia (pes anserinus); flexes/abducts/laterally rotates hip + flexes knee
Medial compartment (obturator nerve, L2-L4):
- Adductors: adductor longus, adductor brevis, adductor magnus (partially sciatic), gracilis, pectineus
- Main action: adduction of thigh
- Adductor magnus has a hiatus (adductor hiatus) through which the femoral vessels pass to become popliteal vessels
Posterior compartment - Hamstrings (sciatic nerve, L5-S2):
- Biceps femoris (long + short head), semimembranosus, semitendinosus
- Origin: ischial tuberosity (except short head of biceps)
- Action: extend hip, flex knee
- Exception: the hamstring part of adductor magnus originates from ischium and is innervated by the sciatic nerve
4. Major Nerves
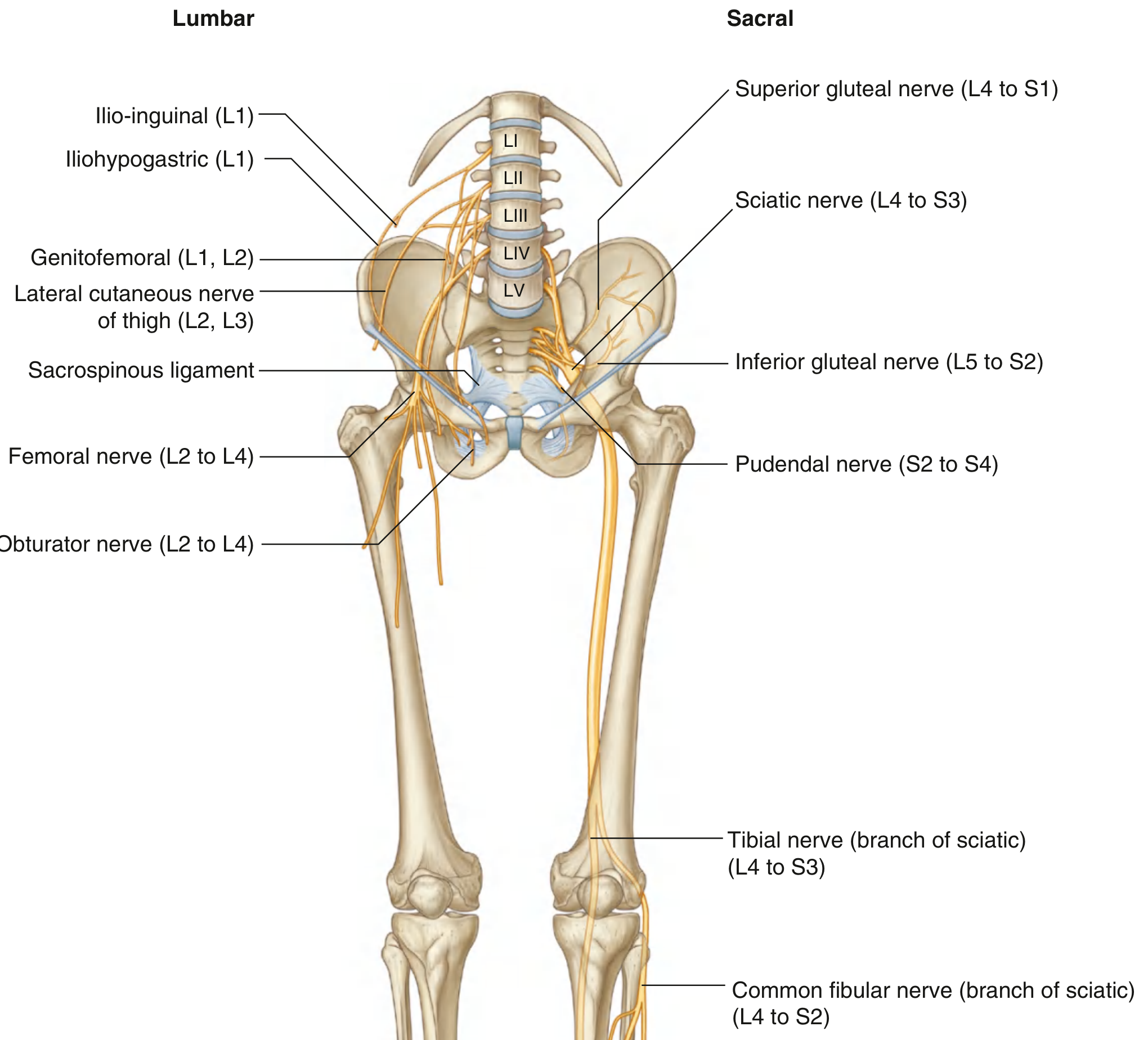
Femoral Nerve (L2-L4)
- Emerges from lateral side of psoas major
- Passes under inguinal ligament lateral to the femoral artery (remember: NAVEL from lateral to medial in femoral triangle = Nerve, Artery, Vein, Empty space [femoral canal], Lymphatics)
- Innervates: quadriceps, sartorius, pectineus; skin of anterior/medial thigh and medial leg (via saphenous nerve)
Obturator Nerve (L2-L4)
- Passes through the obturator canal
- Innervates: medial compartment of thigh (adductors), skin on medial thigh
Sciatic Nerve (L4-S3) - largest nerve in the body
- Exits pelvis via greater sciatic foramen, inferior to piriformis
- Passes through gluteal region → posterior thigh → divides (usually at popliteal fossa) into:
- Tibial nerve (L4-S3) - anterior divisions
- Common fibular nerve (L4-S2) - posterior divisions
- Innervates: all posterior thigh muscles, all leg + foot muscles, lateral leg skin and lateral/plantar foot skin
Exam tip: The common fibular nerve is the most commonly injured nerve in the lower limb - it wraps around the fibular neck and is vulnerable to fracture or compression. Results in foot drop (can't dorsiflex).
Superior Gluteal Nerve (L4-S1)
- Exits above piriformis
- Supplies: gluteus medius, gluteus minimus, tensor fasciae latae
Inferior Gluteal Nerve (L5-S2)
- Exits below piriformis
- Supplies: gluteus maximus only
Memory aid for gluteal nerve exits:
"Superior = Super above piriformis; Inferior = Inferior below piriformis"
5. Dermatomes
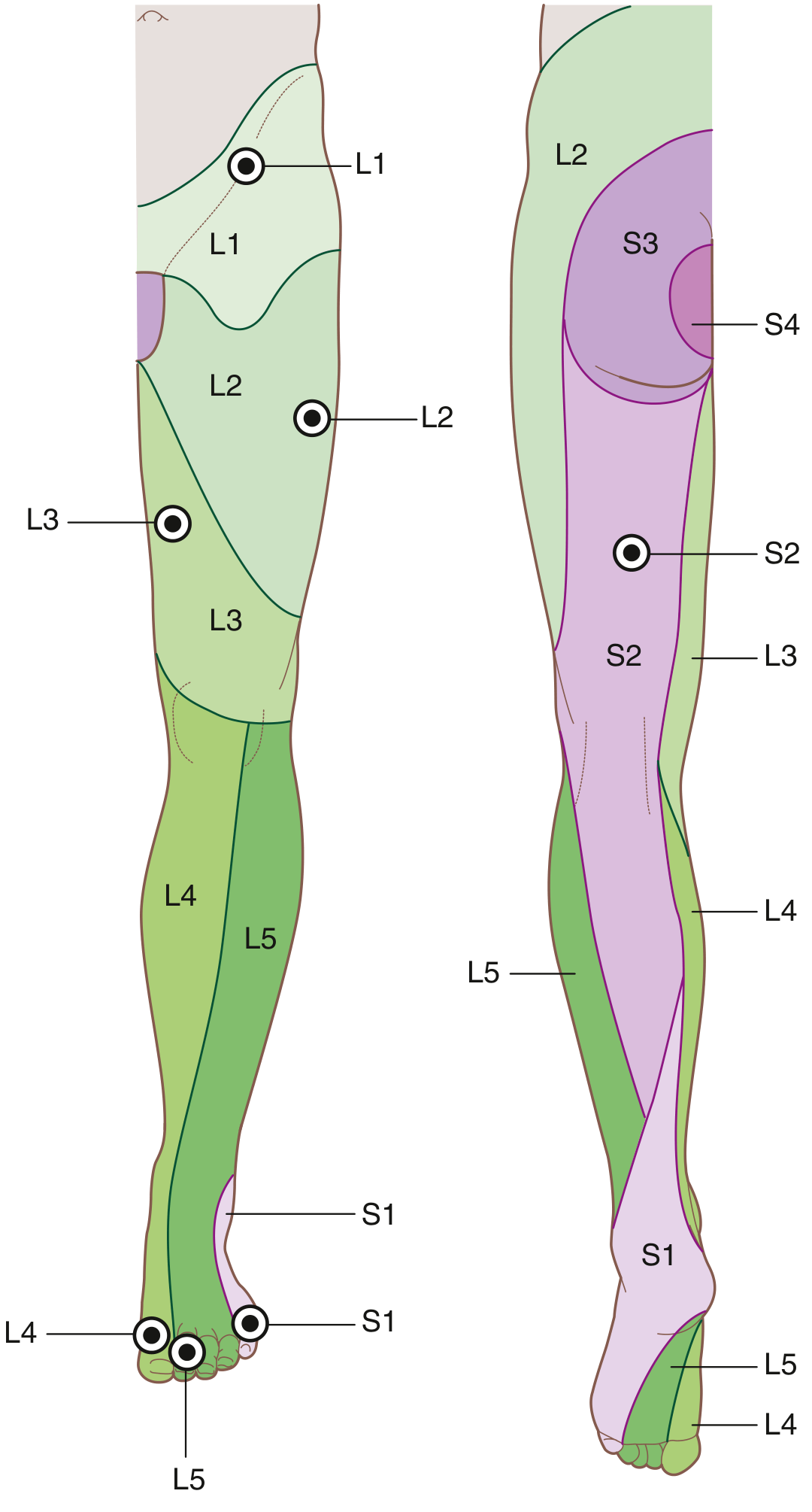
Key testable autonomous zones (minimal overlap):
| Dermatome | Test Area |
|---|---|
| L1 | Over inguinal ligament |
| L2 | Lateral thigh |
| L3 | Lower medial thigh |
| L4 | Medial side of great toe |
| L5 | Medial side of digit II (index toe) |
| S1 | Little toe (digit V) |
| S2 | Back of thigh |
| S3 | Skin over gluteal fold |
Myotomes for Reflexes
| Test | Level |
|---|---|
| Hip flexion | L1, L2 |
| Knee extension | L3, L4 |
| Knee flexion | L5, S1, S2 |
| Plantarflexion | S1, S2 |
| Patellar (knee jerk) reflex | L3, L4 |
| Achilles (ankle jerk) reflex | S1, S2 |
6. The Femoral Triangle
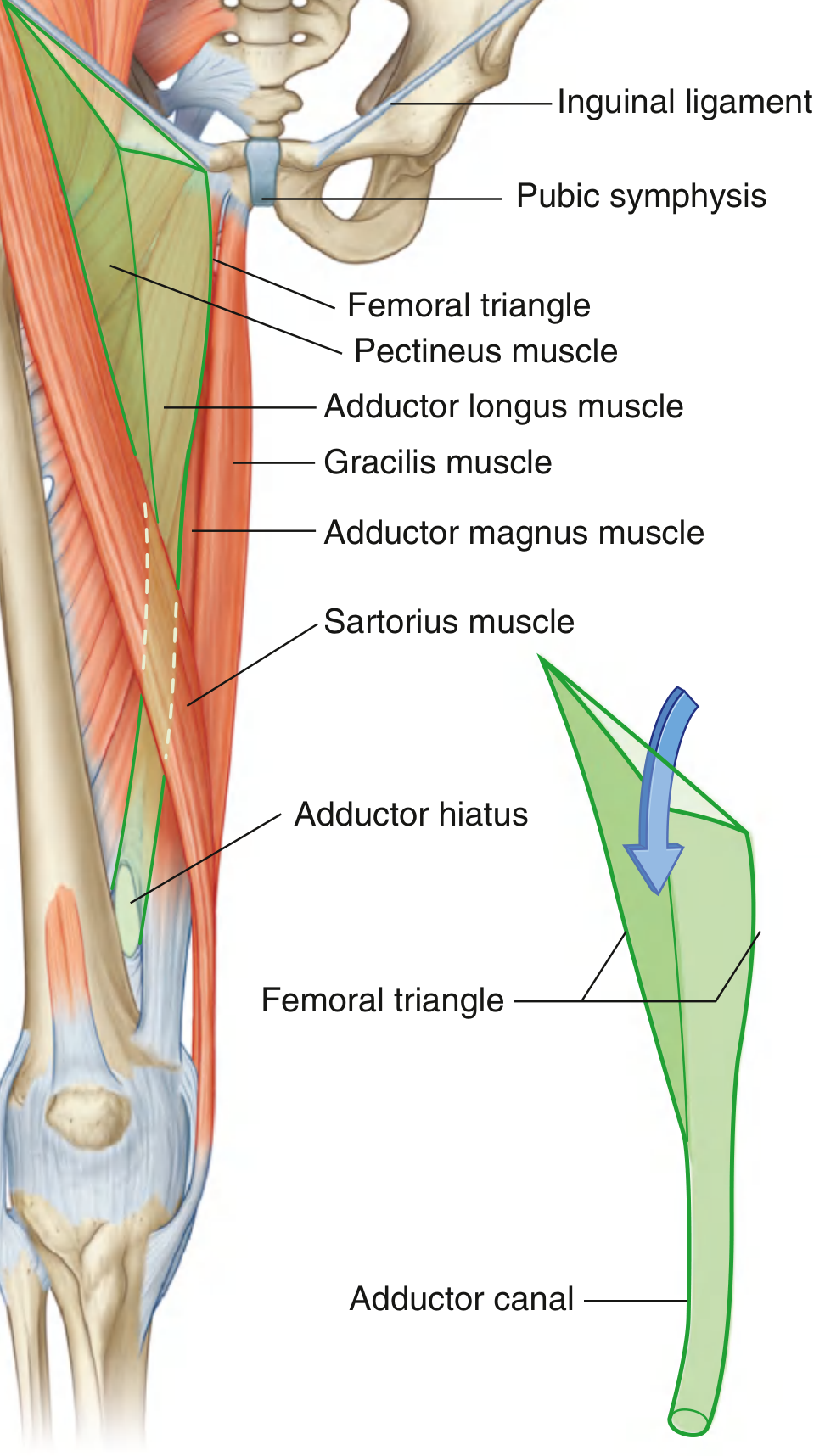
Boundaries:
- Base (roof): Inguinal ligament
- Lateral border: Medial margin of sartorius
- Medial border: Medial margin of adductor longus
- Floor: Iliopsoas (lateral) + pectineus (medial) + adductor longus
Contents (lateral to medial) - NAVEL:
- Nerve (femoral)
- Artery (femoral)
- Vein (femoral)
- Empty space (femoral canal - site of femoral hernias)
- Lymphatics
The femoral artery is palpable just inferior to the inguinal ligament, midway between ASIS and pubic symphysis - this is the mid-inguinal point.
Adductor canal (Hunter's canal): The apex of the femoral triangle continues into this fascial tunnel running down the medial thigh. Femoral artery and vein (+ saphenous nerve) pass through it. At the adductor hiatus (gap in adductor magnus), vessels become the popliteal artery and vein.
7. Blood Supply
Arteries
- Femoral artery = continuation of external iliac below inguinal ligament
- Main branch: Profunda femoris (deep femoral artery) - gives medial and lateral circumflex femoral arteries (form the arterial ring around femoral neck)
- Femoral artery → adductor hiatus → popliteal artery → divides below knee into anterior tibial and posterior tibial arteries
- Obturator artery (from internal iliac) supplies medial compartment
Veins
Superficial veins:
- Great saphenous vein - medial side of dorsal venous arch → medial leg → medial thigh → joins femoral vein just below inguinal ligament at the saphenous opening
- Small saphenous vein - lateral side of dorsal venous arch → posterior leg → joins popliteal vein behind knee
Clinic: Varicose veins occur when venous valves become incompetent, causing reflux and raised pressure in superficial veins. More common in women; aggravated by pregnancy. Great saphenous vein is used as a bypass graft in coronary artery surgery.
8. High-Yield Clinical Correlations
| Clinical Scenario | Anatomical Basis |
|---|---|
| Femoral hernia | Through femoral canal (most medial compartment of femoral sheath); more common in women due to wider pelvis |
| Femoral neck fracture | Disrupts arterial ring → avascular necrosis of femoral head |
| L4/L5 disc herniation | Pain/paresthesia in dermatome of L4 (medial great toe) or L5 (dorsum foot) |
| Foot drop | Common fibular nerve injury at fibular neck (plantarflexion preserved, dorsiflexion lost) |
| Trendelenburg gait | Superior gluteal nerve or gluteus medius weakness |
| Sciatic nerve injury | Posterior to hip joint; posterior thigh + all muscles below knee affected |
| Absent patellar reflex | L3/L4 lesion (femoral nerve) |
| Absent ankle jerk | S1/S2 lesion (tibial nerve) |
Study Sequence Recommendation
Work through the lower limb in this order:
- Bones - identify all landmarks on a skeleton or diagram
- Compartments + muscles - group by compartment, learn nerve per compartment
- Nerves - trace each nerve from its spinal root through its course to what it supplies
- Dermatomes + reflexes - practice on the diagram above
- Clinical correlations - for each nerve, know what a lesion looks like
Want me to go deeper on any specific area - like the leg and foot compartments, hip joint anatomy, knee joint ligaments, or specific nerve injuries?
This is a shared conversation. Sign in to Orris to start your own chat.