Complaints of Ear mbbs 4th yr ENT
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the content needed for a comprehensive answer. Let me compile it all into a well-structured study note.
Complaints of the Ear - ENT (MBBS 4th Year)
Source: Cummings Otolaryngology Head and Neck Surgery
The standard framework for taking an otologic history organizes all ear complaints into five core categories:
Hearing loss · Tinnitus · Otalgia · Otorrhea · Vertigo
Every patient with an ear complaint should be asked about all five, even if they present with only one.
1. Hearing Loss (Hypoacusis)
Hearing loss is one of the most common reasons for presentation to an otolaryngologist. It is classified as:
| Type | Key Features |
|---|---|
| Conductive (CHL) | Hyperacusis of Willis (hears better in background noise), autophony, history of ear infections/surgery/trauma |
| Sensorineural (SNHL) | Can hear but can't understand speech; noise exposure, ototoxic drugs, family history |
| Mixed (MHL) | Features of both |
History questions to ask:
- Duration, progression (slow/sudden/fluctuating)?
- Symmetric or asymmetric?
- Associated tinnitus, vertigo, otalgia, otorrhea?
- Prior ear infection/trauma/surgery?
- Noise exposure (occupational or recreational)?
- Family history of hearing loss?
- Ototoxic medication exposure?
Red Flags in Hearing Loss History (require urgent further evaluation):
| Unilateral | Otalgia |
| Sudden onset | Accompanying cranial nerve signs |
| Fluctuating | Numbness / Diplopia |
| Rapidly progressive | Facial paresis |
| Vertigo or ataxia | Voice/swallowing changes |
| Otorrhea |
Differential Diagnosis Algorithm:
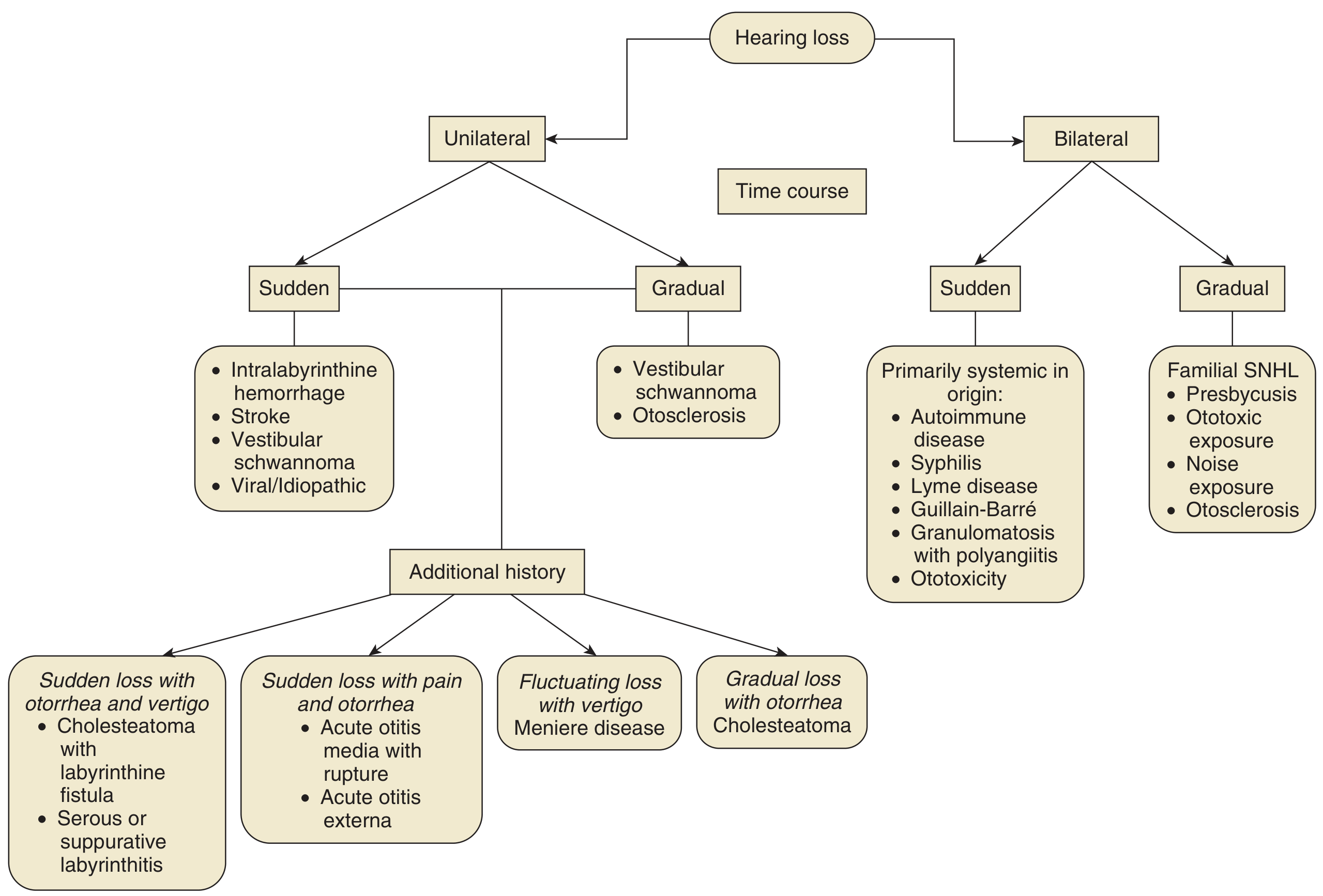
Otosclerosis is a classic cause of bilateral gradual CHL with stapedial fixation - often with a family history and normal otoscopy. Presbycusis causes bilateral gradual high-frequency SNHL in the elderly. Vestibular schwannoma presents as unilateral gradual SNHL.
2. Tinnitus
Tinnitus may be the chief complaint or an incidental symptom. Always explore it thoroughly.
History questions to ask:
- Duration, progression?
- Pulsatile or non-pulsatile?
- How does it sound (ringing, roaring, whistling)?
- Fluctuating / intermittent or constant?
- Symmetric or asymmetric (unilateral vs bilateral)?
- Mitigating factors? Prior therapies tried?
- Associated hearing loss, vertigo, otalgia, otorrhea?
- Caffeine / stimulant use?
Pulsatile tinnitus is a separate line of inquiry - it may signal a serious cerebrovascular problem. Ask about headaches, vision changes, cranial nerve deficits, prior head/neck trauma, cardiac/vascular history.
Also assess the patient's emotional state - tinnitus can cause severe psychological distress, occasionally with suicidal ideation.
Tinnitus Differential Diagnosis Algorithm:
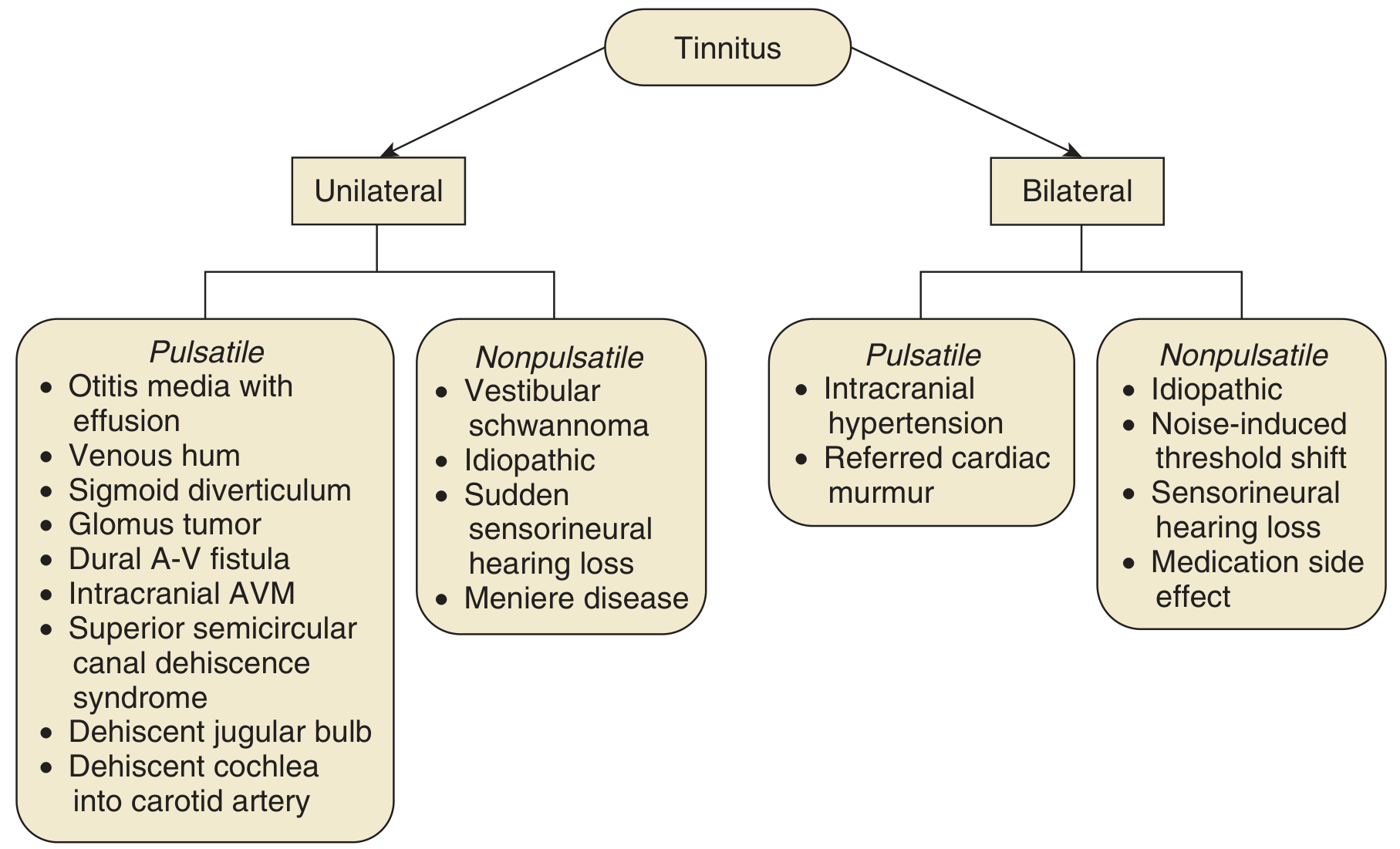
| Unilateral Pulsatile | Unilateral Nonpulsatile | Bilateral Nonpulsatile |
|---|---|---|
| Glomus tumor | Vestibular schwannoma | Noise-induced SNHL |
| Sigmoid diverticulum | Sudden SNHL | Presbycusis |
| Dural A-V fistula | Meniere disease | Medication side effect |
| Superior semicircular canal dehiscence | Idiopathic | Idiopathic |
In Meniere disease: tinnitus is non-pulsatile, often described as roaring or whistling. It tends to begin, get louder, or change pitch as an attack approaches.
3. Otalgia (Ear Pain)
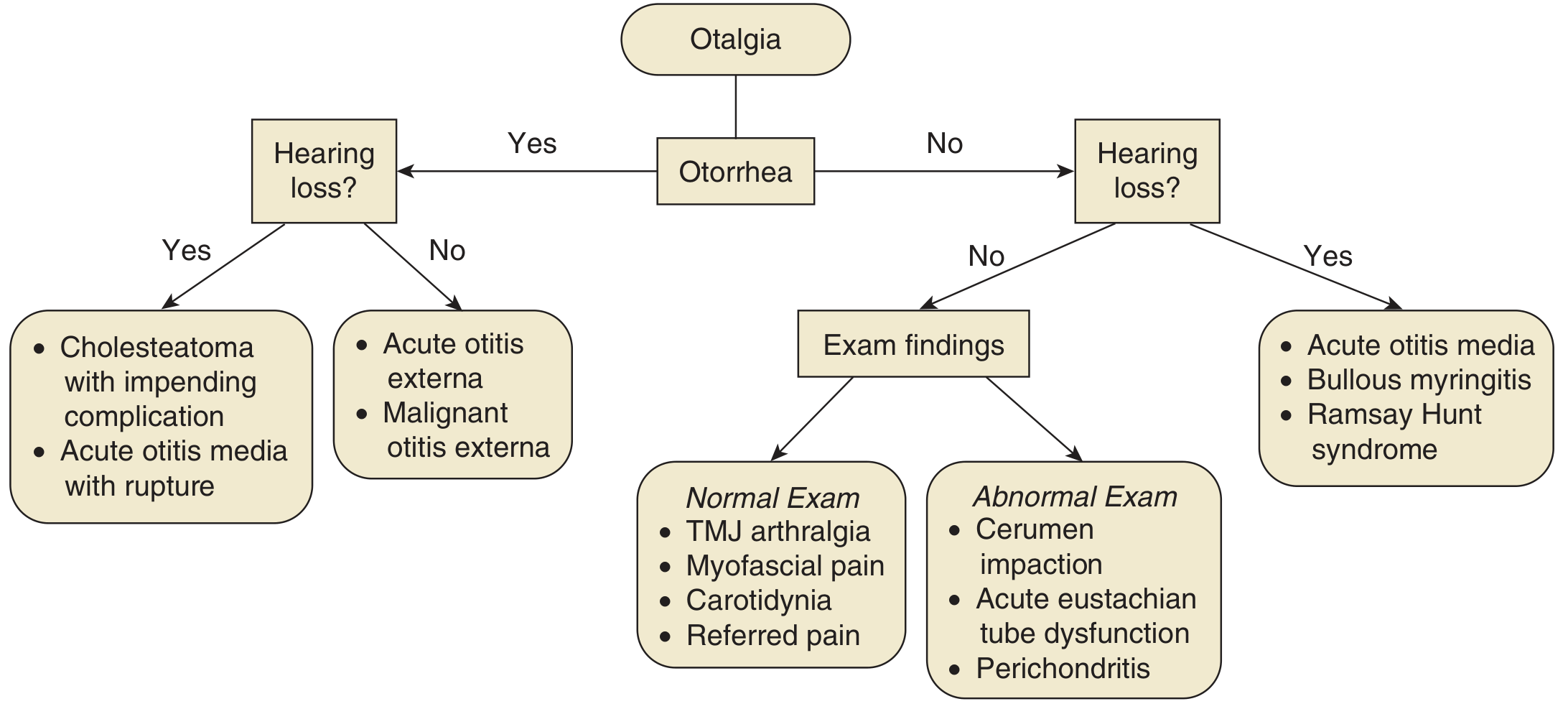
Otalgia is classified as primary (originating from the ear) or referred (from nearby structures via shared innervation).
Primary otalgia is frequently accompanied by hearing loss and otorrhea:
- Otitis externa, otitis media
- Mastoiditis, cholesteatoma
- Skull base osteomyelitis (malignant otitis externa)
- Primary otologic malignancy
Referred otalgia - no hearing loss or otorrhea typically present. Common sources:
- Dental/TMJ - periodontal disease, dental abscesses, bruxism, TMJ arthralgia (most common source)
- Head and neck malignancy - critical not to miss; look for voice/swallowing changes, weight loss, neck mass, tobacco/alcohol history
- Cervical spine pathology
- Post-herpetic neuralgia
Ear fullness: A vague sensation - "underwater," "clogged," or pressure. Consider Eustachian tube dysfunction, chronic otitis media, hidden hearing loss, TMJ dysfunction.
Otalgia Differential Diagnosis Algorithm:
4. Otorrhea (Ear Discharge)
Otorrhea always suggests primary otologic pathology.
Differential by type of discharge:
| Discharge Type | Likely Diagnosis |
|---|---|
| Scanty, purulent, painful | Acute otitis externa (most common cause) |
| Mucopurulent, via tympanostomy tube/perforation | Otitis media (acute or chronic) |
| Chronic, painless, offensive-smelling | Cholesteatoma (key red flag) |
| Chronic, secondary | Chronic otitis externa |
| Clear watery fluid | CSF otorrhea (post-trauma - suspect temporal bone fracture) |
Key point: Chronic painless otorrhea = cholesteatoma until proven otherwise.
CSF otorrhea can result from temporal bone fracture - the clear fluid will be positive for beta-2 transferrin. Always ask about head trauma.
5. Vertigo (Dizziness)
Vertigo is a hallucination of movement - either the environment is spinning or the patient is spinning. It is important to distinguish labyrinthine (peripheral) from central vertigo.
Key history elements:
- Duration of each episode (seconds, minutes, hours, days)?
- Triggers (position change, loud sounds, Valsalva)?
- Associated hearing loss, tinnitus, ear fullness?
- Nausea/vomiting (autonomic symptoms = true labyrinthine vertigo)?
Peripheral (labyrinthine) vertigo features:
- Episodic, short-lived or long episodes depending on cause
- Accompanied by nausea/vomiting
- No neurological symptoms (headache, visual aura, photophobia, weakness, numbness, diplopia)
- No loss of consciousness
Central vertigo red flags (NOT labyrinthine origin):
- Headache, visual aura, photophobia/phonophobia
- Extremity weakness or numbness
- Other cranial nerve deficits
- Diplopia
- Loss of consciousness / syncope
| Disease | Episode Duration | Associated Features |
|---|---|---|
| BPPV | Seconds (10-60 sec) | Triggered by position change |
| Meniere disease | 20 min - 24 hours | Hearing loss, tinnitus, ear fullness (triad) |
| Vestibular neuritis | Days | No hearing loss |
| Labyrinthitis | Days | With hearing loss |
| Posterior circulation stroke | Variable | Central signs |
In Meniere disease: SNHL is typically fluctuating, low-frequency initially; characteristic "peaked" audiogram at 2 kHz. Only 1-2% progress to profound deafness. Diplacusis (different pitch perception in each ear) occurs in ~44% of patients.
Summary Table - The 5 Core Otologic Complaints
| Complaint | Key Distinguishing Features | Important DDx |
|---|---|---|
| Hearing loss | CHL vs SNHL; unilateral vs bilateral; sudden vs gradual | Otosclerosis, presbycusis, schwannoma |
| Tinnitus | Pulsatile vs non-pulsatile; unilateral vs bilateral | Glomus tumor, Meniere, SNHL |
| Otalgia | Primary vs referred; with/without otorrhea | Otitis, TMJ, H&N malignancy |
| Otorrhea | Acute painful vs chronic painless; type of discharge | OE, OM, cholesteatoma, CSF leak |
| Vertigo | Peripheral vs central; duration; triggers | BPPV, Meniere, vestibular neuritis |
Cummings Otolaryngology Head and Neck Surgery, Chapter 137 - "The complete otologic history includes five components: hearing loss, tinnitus, otalgia, otorrhoea, and vertigo, followed by occupational history, family history, surgical history, and co-existing medical conditions."
This is a shared conversation. Sign in to Orris to start your own chat.