STRUCTURE OF ALVEOLAR BONE WITH ITS FUNCTIONS ALSO TYPES AND FORMATION OF ALVEOLAR BONE ACCORDING TO ORBANS BOOK
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
alveolar bone structure types formation functions Orban's oral histology and embryology
Reading Web Page
alveolar bone structure types formation functions bundle bone supporting bone
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
alveolar bone structure histology bundle bone cribriform plate
Loading Image
Reading Web Page
alveolar bone Orban's classification types formation development functions histology
Reading Web Page
alveolar bone structure types bundle bone supporting alveolar bone proper formation development functions
I now have comprehensive information from Orban's Oral Histology (1944), the University of Anbar Oral Histology PDF, and corroborating histology textbooks. Let me compose the complete answer.
Alveolar Bone — According to Orban's Oral Histology & Embryology
Definition
The alveolar process (alveolar bone) is that part of the maxilla and mandible that forms and supports the sockets (alveoli) of the teeth. It is tooth-dependent — it develops with tooth eruption and is gradually resorbed when teeth are lost.
Structure of Alveolar Bone
Orban classifies the alveolar process into two major components:
1. Alveolar Bone Proper
The alveolar bone proper forms the inner wall of the socket and directly lines the alveolus. It has two sub-components:
A. Bundle Bone
- The portion of alveolar bone proper into which the principal fibers (Sharpey's fibers) of the periodontal ligament are anchored.
- Named "bundle bone" because the bundles of principal fibers continue directly into the bone matrix.
- Characterized by collagen fibers arranged at right angles to the Sharpey's fibers in the intercellular substance.
- Contains more calcium salts per unit area → appears as a dense radiopaque line on radiographs.
- Is the lamina dura seen on X-rays.
B. Lamellated Bone
- Lamellae arranged parallel to the surface of adjacent marrow spaces.
- Some lamellae form Haversian systems (osteons).
The alveolar bone proper is perforated by many openings (foramina) carrying branches of the interalveolar nerves and blood vessels into the periodontal ligament — hence it is also called the cribriform plate.
2. Supporting Alveolar Bone
Surrounds the alveolar bone proper and provides support to the socket. Consists of:
A. Cortical Plates (Compact Bone)
- Form the vestibular (buccal/labial) and oral (lingual/palatal) plates of the alveolar processes.
- Consist of longitudinal lamellae and Haversian systems, similar to compact bone elsewhere in the body.
- Continuous with the compact cortical layers of the maxillary and mandibular bodies.
- Thinner in the maxilla than the mandible.
- Thickest in the premolar and molar region of the lower jaw, especially on the buccal side.
- In the anterior region of both jaws, supporting bone is very thin; the cortical plate fuses directly with the alveolar bone proper — no spongy bone intervenes.
- In the maxilla, the outer cortical plate is perforated by small openings through which blood and lymph vessels pass.
B. Spongy (Cancellous) Bone
- Fills the space between the cortical plates and the alveolar bone proper.
- Composed of trabeculae (plates of bone) with marrow spaces between them.
- Marrow spaces contain: blood-forming elements, osteogenic cells, and adipose tissue.
- The maxilla (especially the molar region posterior to the maxillary sinus) is filled with marrow tissue containing immature red blood cells and leukocytes.
- In the mandibular anterior region, spongy bone may be absent entirely.
Cells of Alveolar Bone
| Cell Type | Origin | Function |
|---|---|---|
| Osteoprogenitor cells | Undifferentiated mesenchymal cells | Precursors to osteoblasts |
| Osteoblasts | Differentiated from osteoprogenitor cells | Bone matrix synthesis (osteoid), anchoring Sharpey's fibers |
| Osteocytes | Osteoblasts trapped in lacunae | Maintenance of bone matrix |
| Osteoclasts | Multinucleated; from undifferentiated mesenchymal cells | Bone resorption (produce substances dissolving organic and mineral components) |
Types of Alveolar Bone (By Texture/Microscopic Appearance)
| Type | Features |
|---|---|
| Bundle bone | Sharpey's fibers embedded; dense, calcified; lines the socket |
| Lamellated bone | Organized lamellar pattern; includes Haversian systems |
| Woven (coarse fibrillar) bone | Seen during healing — irregular osteocytes, coarse fibers, less mineral, no lamellae |
| Cortical (compact) bone | Haversian systems; forms the plates of the alveolar process |
| Cancellous (spongy) bone | Trabeculae with marrow spaces; supports the socket |
Formation of Alveolar Bone
Embryonic Origin
- The dental sac (dental follicle) is the source of all three components of the periodontium:
- Inner layer → cementoblasts → cementum
- Outer layer → intramembranous ossification → alveolar bone
- Middle layer → fibroblasts → periodontal ligament fibers
Mechanism — Intramembranous Ossification
- The alveolar process develops by intramembranous (membranous) ossification — directly from mesenchymal tissue, without a cartilage intermediate.
- In the fetal mandible, a trough develops lateral to Meckel's cartilage. Tooth germs lie in this groove along with the alveolar nerve and vessels. Bony septa develop between adjacent tooth germs, eventually separating the dental crypts from the mandibular canal.
- Alveolar bone forms with tooth development and eruption; it diminishes when teeth are lost.
Bone Deposition During Eruption and Tooth Movement
- During mesial drift (physiologic tooth migration):
- Bone is deposited on the distal wall (tension side) — distal wall is made up almost entirely of bundle bone.
- Bone is resorbed on the mesial wall (pressure side) by osteoclasts in adjacent marrow spaces.
- At the alveolar fundus (base of the socket), continual apposition of bone creates resting lines separating parallel layers of bundle bone.
- Once bundle bone reaches a certain thickness, it is partly resorbed from marrow spaces and replaced by Haversian bone or trabeculae — this is the remodeling cycle.
Bone Healing (After Extraction or Fracture)
Healing occurs by formation of coarse fibrillar (woven) bone, characterized by:
- Large, numerous, irregularly arranged osteocytes
- Coarse, irregular collagen fibers
- Reduced inorganic (mineral) substance; increased organic substance
- Absence of lamellae and resting lines
This is later replaced by mature lamellar bone.
Functions of Alveolar Bone
Orban describes alveolar bone function in the context of its adaptation to functional demands:
-
Support and fixation of teeth — provides bony sockets (alveoli) that house and stabilize the roots of teeth via the periodontal ligament.
-
Transmission and distribution of masticatory forces — masticatory loads are transmitted from teeth → periodontal ligament → alveolar bone → rest of the jaw skeleton.
-
Remodeling in response to tooth movement — bone is continuously resorbed and deposited during physiologic tooth drift and orthodontic movement, allowing the entire alveolus to shift with the teeth.
-
Functional adaptation — increased functional forces lead to formation of new bone (trabecular thickening); decreased function leads to decreased bone volume (disuse atrophy). This is clearly seen in teeth that have lost their antagonists — the spongy bone shows marked rarefaction.
-
Mineral reservoir — serves as a reservoir for calcium and phosphate, participating in systemic mineral metabolism (shared with all bones).
-
Hemopoiesis — the marrow spaces of cancellous bone contain blood-forming elements, particularly in the maxillary molar region.
-
Proprioception and sensory function — blood vessels and nerves pass through the cribriform plate perforations into the periodontal ligament, contributing to sensory (pain, pressure) and nutritive functions of the periodontium.
Radiographic Landmark
The lamina dura is the radiographic correlate of the alveolar bone proper (bundle bone). It appears as a continuous white (radiopaque) line around the root on periapical radiographs. Its continuity and density are clinical indicators of periodontal health — loss of lamina dura suggests bone resorption (e.g., periodontitis, hyperparathyroidism).
Diagram — Gingiva and Alveolar Bone Relationship
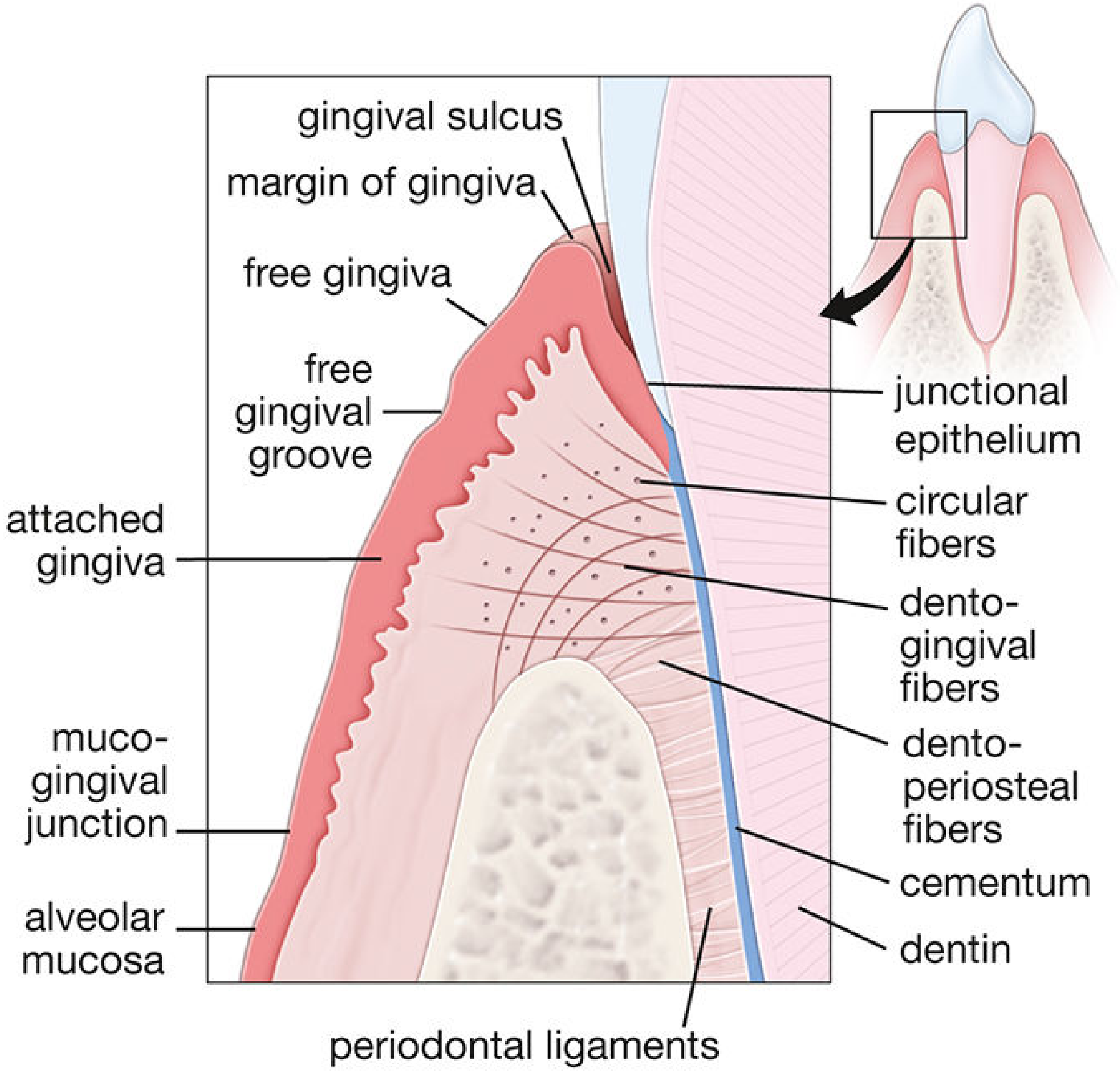
Schematic of gingival and periodontal structures — collagen fibers extend from the cementum of the tooth and from the alveolar bone crest toward the gingival epithelium. — Histology: A Text and Atlas (Pawlina), p. 1461
Sources:
- Orban's Oral Histology and Embryology (Chapter 8: Maxilla and Mandible/Alveolar Process), 1944 — via UNSW Embryology Archive
- Oral Histology lecture notes, University of Anbar Dentistry College (Orban-based curriculum)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina), p. 1460–1463
- Junqueira's Basic Histology, 17e, p. 752
- Color Atlas of Human Anatomy Vol. 2 (Thieme), p. 278–280
This is a shared conversation. Sign in to Orris to start your own chat.