Why ACE inhibitors reduce clearance of lithium
ACE inhibitors lithium renal clearance interaction
Why ACE Inhibitors Reduce the Renal Clearance of Lithium
How Lithium is Normally Handled by the Kidney
- ~75% is reabsorbed in the proximal tubule
- ~25% is reabsorbed in the distal tubule
- Only ~20% of the filtered load is ultimately excreted
The ACE Inhibitor Mechanism - Step by Step
- Stimulate proximal tubular Na⁺/H⁺ exchange (directly increasing proximal reabsorption)
- Stimulate aldosterone release from the adrenal cortex
Parallel Drug Classes That Cause the Same Effect
| Drug Class | Mechanism of Li⁺ Retention |
|---|---|
| ACE inhibitors | ↓ Ang II → ↓ aldosterone → volume contraction → ↑ proximal reabsorption |
| ARBs | Same net effect (block Ang II at AT1 receptor) |
| NSAIDs | ↓ Prostaglandin synthesis → ↓ renal blood flow → ↓ GFR + ↑ proximal reabsorption |
| Thiazide diuretics | Volume contraction → ↑ proximal Na⁺/Li⁺ reabsorption (also blocks distal reabsorption of Na⁺) |
| Loop diuretics | Natriuresis → volume contraction → compensatory proximal Li⁺ retention |
- Goodman & Gilman's The Pharmacological Basis of Therapeutics, Block 3
- Katzung's Basic and Clinical Pharmacology, 16th Edition, Block 13
Clinical Implications
- Lithium has a narrow therapeutic index (target: 0.6-1.25 mmol/L; toxic: >1.5 mmol/L). Even modest changes in clearance can push plasma levels into the toxic range.
- ACE inhibitors are generally avoided in lithium-treated patients. If used, lithium levels must be monitored closely and the dose reduced. - Comprehensive Clinical Nephrology, 7th Edition, p. 902
- The interaction can develop insidiously - patients can develop chronic lithium toxicity (tremor, ataxia, cognitive slowing, nephrogenic diabetes insipidus) even at "near-therapeutic" serum levels, because intracellular lithium accumulation precedes the rise in serum levels.
- The same mechanism explains why volume depletion from any cause (poor oral intake, diarrhea, fever) increases lithium toxicity risk.
Mechanism of action of ACE inhibitors and its uses
ACE inhibitors cardiovascular renal outcomes
ACE Inhibitors - Mechanism of Action and Uses
The RAAS: What ACE Does Normally
- Low renal perfusion → juxtaglomerular cells release renin
- Renin cleaves angiotensinogen → angiotensin I (inactive)
- ACE (angiotensin-converting enzyme), located mainly in the pulmonary endothelium, cleaves angiotensin I → angiotensin II (highly active)
- Angiotensin II causes:
- Powerful vasoconstriction (via AT1 receptors on vascular smooth muscle)
- Aldosterone release from the adrenal cortex → Na⁺/water retention
- Direct stimulation of proximal tubular Na⁺ reabsorption
- Sympathetic nervous system activation
- Cardiac and vascular remodeling (fibrosis, hypertrophy)
Mechanism of Action of ACE Inhibitors
| Action | Effect |
|---|---|
| ↓ Angiotensin II | Vasodilation (↓ peripheral vascular resistance), ↓ aldosterone, ↓ Na⁺/water retention |
| ↑ Bradykinin | Further vasodilation via NO and prostacyclin release |
-
Blood pressure falls via reduced afterload (peripheral resistance) and reduced preload (less aldosterone/fluid retention)
-
Cardiac output and heart rate are not significantly changed - no reflex tachycardia (unlike direct vasodilators), because baroreceptors reset and vagal tone is enhanced
-
In the kidney: reduced efferent arteriolar resistance lowers intraglomerular capillary pressure → reduces proteinuria
-
Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 278-279
Individual Drug Notes
Clinical Uses
- First-line agents, especially effective in high-renin states and in combination with diuretics or calcium channel blockers
- Lower BP without reflex tachycardia - safe in ischemic heart disease
- Class I indication - overwhelming trial evidence shows reduction in mortality, hospitalization, and improvement in symptoms
- Reduce both preload (less aldosterone → less Na⁺ retention) and afterload (vasodilation)
- Attenuate and reverse adverse cardiac remodeling (LV hypertrophy, fibrosis)
- Key trials: CONSENSUS, SOLVD, SAVE - Braunwald's Heart Disease, 2-Vol Set
- Started within hours of MI in patients with LV dysfunction (EF <40%) or signs of HF
- Reduce mortality, prevent post-MI LV remodeling, and reduce progression to overt HF
- Reduce intraglomerular capillary pressure by dilating the efferent arteriole
- Decrease proteinuria and slow progression of CKD - recommended even without hypertension in diabetics with microalbuminuria
- Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 278
- Reduce proteinuria and stabilize GFR by lowering glomerular capillary pressure
- Renoprotective independent of BP lowering
- The HOPE trial showed ramipril reduced MI, stroke, and cardiovascular death in high-risk patients without HF
- Evidence suggests ACE inhibitors also reduce the incidence of new-onset diabetes
- Cause regression of LVH - superior to some other antihypertensives in this regard
Adverse Effects
| Side Effect | Mechanism |
|---|---|
| Dry cough (~10-15%) | ↑ Bradykinin and substance P accumulation in airways |
| Angioedema (rare but dangerous) | ↑ Bradykinin causing submucosal/subdermal edema |
| Hyperkalemia | ↓ Aldosterone → ↓ urinary K⁺ excretion; worse in CKD/diabetes |
| Acute renal failure | Bilateral renal artery stenosis - removing efferent arteriole tone drops GFR catastrophically |
| First-dose hypotension | Especially in hypovolemic or high-renin states |
| Fetotoxicity | Contraindicated in pregnancy (2nd/3rd trimester): fetal hypotension, anuria, renal failure |
| Taste disturbance / rash | Captopril's sulfhydryl group (less with other ACEIs) |
- Katzung's Basic and Clinical Pharmacology, 16th Edition, p. 279
Contraindications
- Pregnancy (2nd and 3rd trimester - absolute; 1st trimester - relative)
- Bilateral renal artery stenosis (or stenosis of solitary kidney)
- Prior ACE inhibitor-induced angioedema
- Hyperkalemia (K⁺ >5.5 mEq/L)
- Avoid combining with ARBs or aliskiren (dual RAAS blockade - increased toxicity without added benefit in clinical trials)
ACE Inhibitors vs. ARBs - Key Distinction
Drug treatment plan of diabetes mellitus 2 in flowchart
ADA 2025 type 2 diabetes treatment algorithm flowchart guidelines
https://www.guidelinecentral.com/guideline/14119
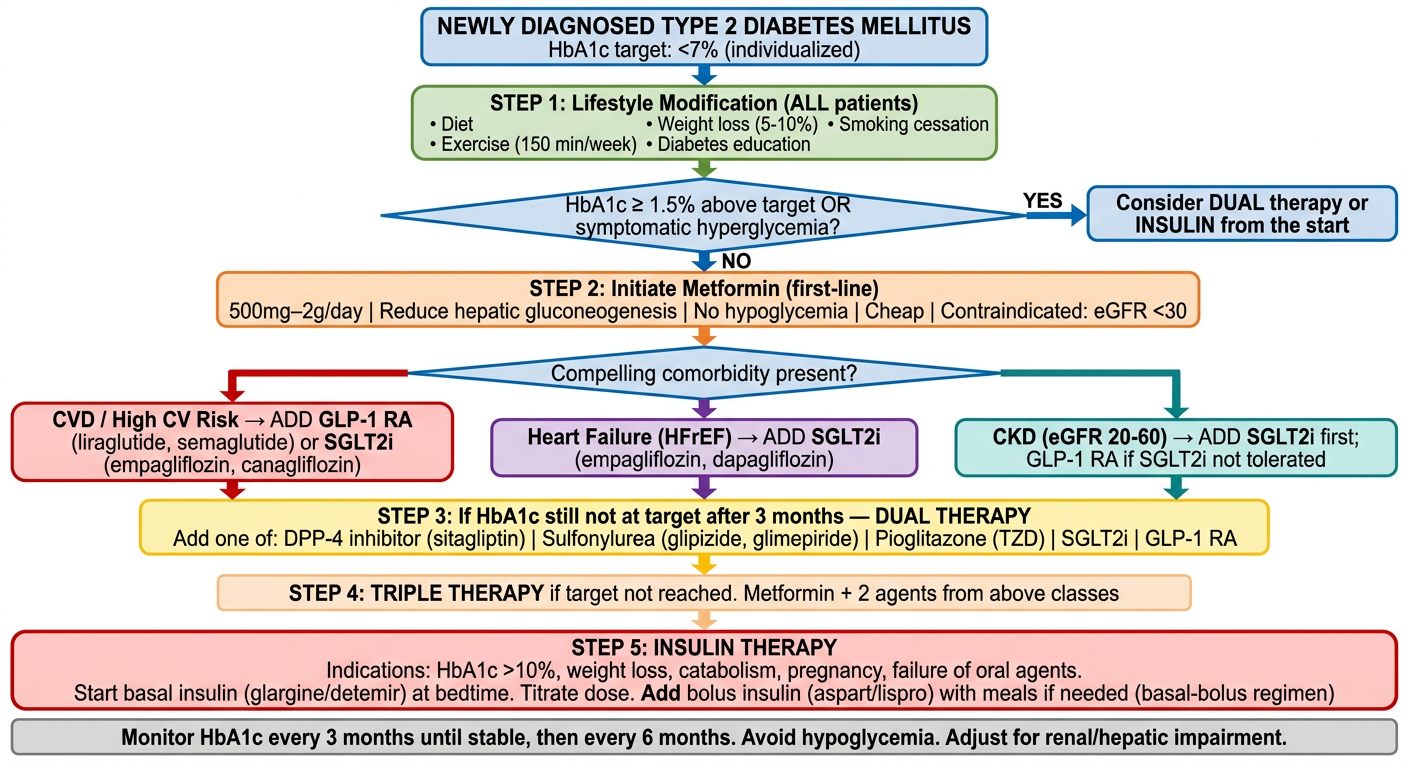
A detailed clinical flowchart for Type 2 Diabetes Mellitus drug treatment plan based on ADA 2026 guidelines. The flowchart flows top to bottom with clear decision boxes and arrows. Include these steps in order: 1. TOP BOX (blue): "NEWLY DIAGNOSED TYPE 2 DIABETES MELLITUS" with sub-note "HbA1c target: <7% (individualized)" 2. FIRST STEP (green): "STEP 1: Lifestyle Modification (ALL patients)" bullet points: Diet, Exercise (150 min/week), Weight loss (5-10%), Diabetes education, Smoking cessation 3. DECISION DIAMOND: "HbA1c ≥ 1.5% above target OR symptomatic hyperglycemia?" - YES arrow leads to: "Consider DUAL therapy or INSULIN from the start" - NO arrow leads to: STEP 2 4. STEP 2 (orange): "STEP 2: Initiate Metformin (first-line)" notes: "500mg–2g/day | Reduce hepatic gluconeogenesis | No hypoglycemia | Cheap | Contraindicated: eGFR <30" 5. DECISION DIAMOND: "Compelling comorbidity present?" Arrow branches to THREE boxes side by side: - BOX A (red): "CVD / High CV Risk → ADD GLP-1 RA (liraglutide, semaglutide) or SGLT2i (empagliflozin, canagliflozin)" - BOX B (purple): "Heart Failure (HFrEF) → ADD SGLT2i (empagliflozin, dapagliflozin)" - BOX C (teal): "CKD (eGFR 20-60) → ADD SGLT2i first; GLP-1 RA if SGLT2i not tolerated" 6. STEP 3 (yellow): "STEP 3: If HbA1c still not at target after 3 months — DUAL THERAPY" Add one of: DPP-4 inhibitor (sitagliptin) | Sulfonylurea (glipizide, glimepiride) | Pioglitazone (TZD) | SGLT2i | GLP-1 RA 7. STEP 4 (light orange): "STEP 4: TRIPLE THERAPY" if target not reached. Metformin + 2 agents from above classes 8. STEP 5 (red box): "STEP 5: INSULIN THERAPY" Indications: HbA1c >10%, weight loss, catabolism, pregnancy, failure of oral agents. Start basal insulin (glargine/detemir) at bedtime. Titrate dose. Add bolus insulin (aspart/lispro) with meals if needed (basal-bolus regimen) 9. BOTTOM NOTE BOX (grey): "Monitor HbA1c every 3 months until stable, then every 6 months. Avoid hypoglycemia. Adjust for renal/hepatic impairment." Use color-coded boxes, clear arrows, clean medical diagram style, readable font size, white background.
Type 2 Diabetes Mellitus - Drug Treatment Plan
Step-by-Step Explanation
STEP 1 - Lifestyle Modification (ALL patients, at diagnosis)
- Diet: Caloric restriction, low glycemic index foods, Mediterranean or low-carb diet
- Exercise: ≥150 min/week of moderate aerobic activity + resistance training
- Weight loss: Target 5-10% body weight reduction
- Diabetes education and self-monitoring of glucose
- Smoking cessation
DECISION POINT 1: Is HbA1c ≥1.5% above target OR is the patient symptomatic?
- YES → Start with dual therapy or insulin immediately (don't wait for monotherapy to fail)
- NO → Proceed to Step 2
STEP 2 - First-Line: METFORMIN
| Feature | Detail |
|---|---|
| Dose | 500-2000 mg/day (with meals) |
| Mechanism | ↓ Hepatic gluconeogenesis, ↑ insulin sensitivity |
| HbA1c reduction | ~1.0-1.5% |
| Advantages | No hypoglycemia, cheap, weight-neutral, cardioprotective |
| Contraindications | eGFR <30 mL/min; hold before contrast; active liver disease |
DECISION POINT 2: Compelling Comorbidity?
| Comorbidity | Preferred Add-On Drug | Reason |
|---|---|---|
| ASCVD / High CV Risk | GLP-1 RA (semaglutide, liraglutide) or SGLT2i (empagliflozin, canagliflozin) | Proven MACE reduction in EMPA-REG, LEADER, SUSTAIN-6 trials |
| Heart Failure (HFrEF) | SGLT2i (empagliflozin, dapagliflozin) | Reduce HF hospitalizations, mortality |
| CKD (eGFR 20-60) | SGLT2i first choice; GLP-1 RA if SGLT2i not tolerated | Reduce proteinuria, slow CKD progression |
| Obesity / Weight loss needed | GLP-1 RA (semaglutide, tirzepatide) | Significant weight loss (5-15%) |
| Hypoglycemia risk | DPP-4 inhibitor (sitagliptin, saxagliptin) | No hypoglycemia |
| Cost concern | Sulfonylurea (glimepiride, glipizide) | Very cheap; but risk of hypoglycemia + weight gain |
STEP 3 - Dual Therapy (if HbA1c not at target after 3 months)
| Drug Class | Examples | HbA1c ↓ | Key Notes |
|---|---|---|---|
| SGLT2 inhibitor | Empagliflozin, dapagliflozin, canagliflozin | 0.5-1.0% | Glucosuria, UTI risk, genital infections; do NOT use if eGFR <30 |
| GLP-1 receptor agonist | Semaglutide, liraglutide, dulaglutide | 0.8-1.5% | Injectable or oral (semaglutide); nausea; weight loss |
| DPP-4 inhibitor | Sitagliptin, saxagliptin, alogliptin | 0.5-0.8% | Well tolerated; no hypoglycemia; no weight change |
| Sulfonylurea | Glimepiride, glipizide, glyburide | 1.0-1.5% | Hypoglycemia risk; weight gain; cheap |
| TZD (Pioglitazone) | Pioglitazone | 0.5-1.4% | Edema, weight gain, fracture risk; avoid in HF |
| GIP/GLP-1 dual agonist | Tirzepatide (Mounjaro) | 1.5-2.5% | Powerful weight loss; newest class |
STEP 4 - Triple Therapy (if HbA1c still not at target)
STEP 5 - Insulin Therapy
- HbA1c >10% at diagnosis
- Symptomatic hyperglycemia (polyuria, polydipsia, weight loss)
- Failure of 3+ oral agents
- Acute illness, surgery, pregnancy
- Catabolism, significant weight loss
Start: Basal insulin (glargine, detemir, degludec)
→ 10 units/night OR 0.1-0.2 units/kg at bedtime
→ Titrate by 2 units every 3 days until fasting glucose 80-130 mg/dL
If postprandial glucose still high:
→ Add bolus insulin (lispro, aspart, glulisine) before largest meal
→ Progress to full basal-bolus regimen (4 injections/day)
Monitoring Throughout All Steps
| Parameter | Frequency |
|---|---|
| HbA1c | Every 3 months until stable, then every 6 months |
| Fasting glucose / CGM | Daily or as needed |
| Renal function (eGFR, creatinine) | Annually (more often if CKD) |
| Urine albumin:creatinine ratio | Annually |
| Blood pressure | Every visit |
| Lipid panel | Annually |
| Ophthalmology | Annually (or at diagnosis, then every 2 years if normal) |
| Foot exam | Every visit |
Key 2026 ADA Updates (vs. older guidelines)
- Early combination therapy is now actively encouraged rather than stepwise monotherapy escalation
- GLP-1 RAs and SGLT2i are preferred add-ons regardless of HbA1c when CV/renal comorbidities exist
- Tirzepatide (dual GIP/GLP-1) recognized as highly effective for both glycemia and weight
- Avoid combining ACE inhibitor + ARB; avoid dual RAAS blockade
- Metformin + SGLT2i is now often recommended as a starting combination in many high-risk patients