Levofloxacillin in thrombocytopenia
Reading File
Finding Sources
Searching PubMed
levofloxacin thrombocytopenia
Searching the Web
levofloxacin induced thrombocytopenia mechanism clinical management
Reading File
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC4738914
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Here is a thorough, well-sourced answer:
Levofloxacin and Thrombocytopenia
Note on terminology: "Levofloxacillin" is not a real drug. The correct name is levofloxacin (Levaquin), a third-generation fluoroquinolone antibiotic. The "-cillin" suffix belongs to penicillin-class drugs.
Overview
Levofloxacin can cause thrombocytopenia through at least two distinct mechanisms:
- Drug-Induced Immune Thrombocytopenia (DIIT) - the more common mechanism
- Drug-Induced Thrombotic Thrombocytopenic Purpura (TTP) - rarer but more severe
1. Drug-Induced Immune Thrombocytopenia (DIIT)
Mechanism:
Levofloxacin, like other fluoroquinolones, shares structural similarities in its central ring with quinine, a well-established cause of immune-mediated thrombocytopenia. The proposed mechanism involves:
- The drug binds to platelet surface glycoproteins (particularly GPIIb/IIIa) and acts as a hapten or conformational inducer.
- Drug-dependent antibodies (typically IgG) form and bind to this drug-platelet complex.
- Immune-mediated platelet destruction leads to peripheral thrombocytopenia.
- In vitro analysis shows anti-glycoprotein IIb/IIIa IgG with increased binding affinity in the presence of soluble fluoroquinolone molecules.
Clinical features:
- Onset typically within days of starting the drug (a published case report describes severe thrombocytopenia after just 4 days of oral levofloxacin)
- Can occur on first exposure (no prior sensitization required in some cases)
- May present with hemoptysis, petechiae, ecchymosis, or mucosal bleeding
- Platelet counts can drop dramatically (severe thrombocytopenia)
- Patients previously tolerant of ciprofloxacin may still develop levofloxacin-induced thrombocytopenia - cross-reactivity between fluoroquinolones is not guaranteed
Management:
- Stop levofloxacin immediately - this is the single most important step
- Switch to an alternative antibiotic from a different class (e.g., cefepime, beta-lactams)
- Platelet count typically recovers within days to weeks after discontinuation
- Monitor CBC closely; transfuse platelets only if life-threatening bleeding occurs
2. Drug-Induced TTP (Thrombotic Thrombocytopenic Purpura)
Levofloxacin, along with ciprofloxacin and ofloxacin, is listed among drugs associated with TTP - a thrombotic microangiopathy. This is documented in Tintinalli's Emergency Medicine.
Mechanism:
- Triggered by autoantibody formation against ADAMTS-13 (von Willebrand factor-cleaving protease), or by direct microvascular endothelial cell injury.
- Without ADAMTS-13 function, large vWF multimers accumulate, leading to platelet microthrombi throughout the microvasculature.
- Results in the classic TTP pentad: microangiopathic hemolytic anemia, thrombocytopenia, neurologic abnormalities, renal impairment, fever
Key distinguishing features from DIIT:
| Feature | DIIT | Drug-TTP |
|---|---|---|
| Mechanism | Drug-dependent antibodies vs. GPIIb/IIIa | ADAMTS-13 deficiency / microangiopathy |
| Hemolysis | Absent | Present (schistocytes on smear) |
| Coagulation studies | Normal | Normal (no DIC) |
| End-organ damage | Rare | CNS, renal |
| Treatment | Stop drug | Stop drug + plasma exchange |
Treatment of drug-TTP:
- Discontinue levofloxacin immediately
- Daily plasmapheresis (40 mL/kg or 1.0-1.5x plasma volume) - effective in >80% of cases
- Fresh frozen plasma if plasmapheresis cannot be started promptly
- Avoid platelet transfusions (can worsen thrombosis, cause renal failure, and death) unless life-threatening bleeding or intracranial hemorrhage
- Steroids, rituximab, cyclosporine may be added in autoimmune TTP
- Heparin is NOT beneficial in TTP
Clinical Bottom Line
| Aspect | Key Point |
|---|---|
| Incidence | Rare but well-documented; most reports are case series/reports |
| Onset | Days (DIIT) to weeks (TTP) after starting levofloxacin |
| Severity | Can be severe (platelets <20,000/mm³) |
| Diagnosis | Clinical - exclude other causes, temporal relationship to drug |
| Treatment | Stop levofloxacin + supportive care; plasma exchange if TTP suspected |
| Prognosis | Good with early drug discontinuation in DIIT; variable in TTP |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide - levofloxacin listed among drugs causing TTP via ADAMTS-13/microangiopathic mechanism
- PMC4738914 (Probable Levofloxacin-Induced Thrombocytopenia, Case Report + Literature Review) - GPIIb/IIIa antibody mechanism, ciprofloxacin structural similarity to quinine
- Polprasert & Prayongratana, JMAT - case of severe thrombocytopenia after 4 days of levofloxacin, first exposure, anti-GPIIb/IIIa antibody mechanism
Drugs causing thrombocytopenia
Finding Sources
Searching PubMed
"drug-induced thrombocytopenia"[MeSH Terms] AND mechanisms
Searching the Web
drugs causing thrombocytopenia mechanisms classification list 2024
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a comprehensive, well-structured overview of drugs causing thrombocytopenia, drawn from multiple major textbooks:
Drugs Causing Thrombocytopenia
Drug-induced thrombocytopenia (DIT) is one of the most frequent causes of cytopenias evaluated clinically. Over 70 drugs have been documented to cause thrombocytopenia. Understanding the mechanism is essential for correct diagnosis and management.
Mechanisms of Drug-Induced Thrombocytopenia
1. Immune-Mediated (Most Common)
The drug or its metabolite interacts with platelet surface glycoproteins, triggering antibody-mediated platelet destruction. Three sub-types:
| Sub-type | Mechanism | Example Drugs |
|---|---|---|
| Drug-dependent antibody (hapten model) | Drug binds platelet protein, alters its conformation; antibody forms against drug-protein complex. In absence of drug, neoantigen disappears and platelet count recovers. | Quinine, quinidine, vancomycin, beta-lactams, rifampin |
| Drug-adsorption model | Drug is directly deposited on the platelet surface; antidrug IgG leads to accelerated splenic clearance | Penicillin, cephalosporins |
| Autoantibody induction | Drug stimulates true autoantibodies independent of drug presence (drug does not need to be present for antibody to bind platelets) | Gold salts, procainamide, checkpoint inhibitors (anti-PD1, anti-CTLA4) |
| GPIIb/IIIa conformational change | Drug binds GPIIb/IIIa, induces a new immunogenic epitope; IgG antibodies form against this altered conformation | Abciximab, tirofiban, eptifibatide (GPIIb/IIIa inhibitors) |
Quinine is the classic prototype. Even quinine in tonic water can trigger severe, life-threatening thrombocytopenia ("gin and tonic purpura") - the reaction is not dose-dependent.
2. Heparin-Induced Thrombocytopenia (HIT) - Special Category
HIT is the most clinically important drug-induced thrombocytopenia because it causes thrombosis, not just bleeding.
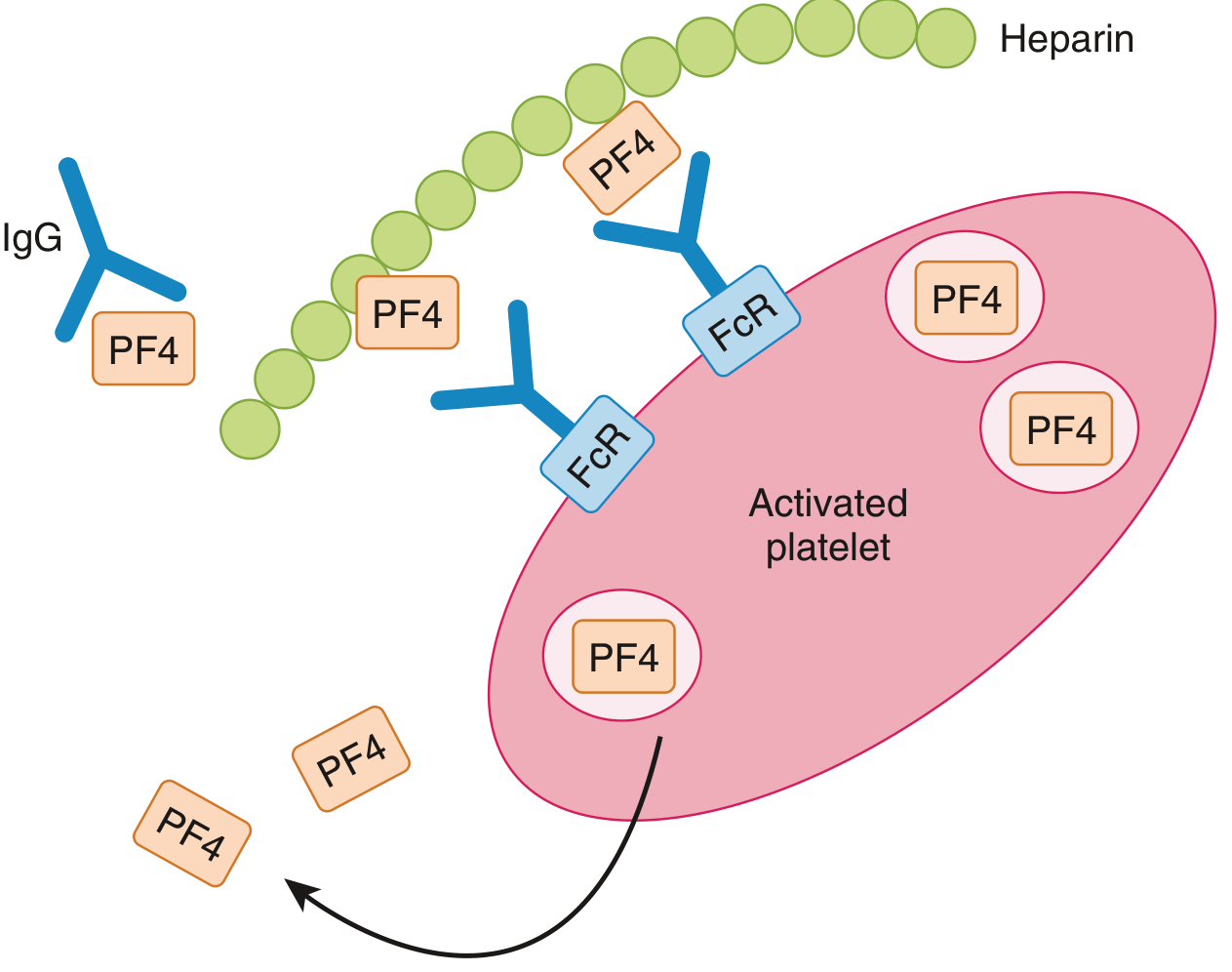
Pathophysiology of HIT: PF4 secreted from platelet granules binds heparin. This PF4-heparin complex becomes immunogenic in susceptible patients, generating IgG antibodies. Large IgG-heparin-PF4 complexes accumulate on platelet surfaces, activating platelets via their FcγRII receptor - leading to further PF4 release and a self-perpetuating thrombotic cascade. (Goldman-Cecil Medicine)
| Feature | Type I HIT | Type II HIT |
|---|---|---|
| Onset | Shortly after starting heparin | Days 5-14 (or sooner with re-exposure) |
| Mechanism | Direct platelet aggregation by heparin | IgG antibody against PF4-heparin complex |
| Severity | Mild, often self-limiting | Severe - life-threatening thrombosis |
| Consequence | Rarely clinically significant | Venous and arterial thrombosis; limb loss risk |
| Frequency | More common | Less common (2-5% with UFH, 0.7% with LMWH) |
| Management | Continue or stop heparin | Immediately stop ALL heparin; start non-heparin anticoagulant |
- UFH carries higher HIT risk than LMWH
- Fondaparinux: virtually no HIT risk
- Once Type II HIT develops, even LMWH must be avoided
3. Myelosuppression (Decreased Production)
Drugs that suppress the bone marrow directly reduce megakaryocyte production, resulting in thrombocytopenia (often with concurrent anemia and leukopenia):
- Cytotoxic chemotherapy (most agents)
- Radiation therapy
- Ethanol (chronic use)
- Ganciclovir, valganciclovir
- Linezolid (with prolonged use)
- Chloramphenicol
4. TTP (Thrombotic Microangiopathy)
Some drugs trigger TTP by inducing anti-ADAMTS-13 autoantibodies or direct microvascular endothelial injury. Results in platelet consumption within microthrombi:
- Fluoroquinolones: ciprofloxacin, ofloxacin, levofloxacin
- Quinine
- Clopidogrel, ticlopidine
- Cyclosporine, sirolimus (especially in combination)
- Mitomycin
- Valacyclovir
- Risperidone, lansoprazole, infliximab
Drugs Strongly Associated with Thrombocytopenia (by class)
From Goldman-Cecil Medicine (Table 158-3):
Antibiotics and Antivirals
| Drug | Notes |
|---|---|
| Quinine / Quinidine | Prototype; drug-dependent Ab against GPIb/IX and GPIIIa; even small amounts in tonic water can trigger it |
| Vancomycin | Drug-dependent antibody; can be severe |
| Penicillin | Hapten-type mechanism |
| Cephalosporins | Drug-adsorption; ceftriaxone well-documented |
| Trimethoprim-sulfamethoxazole | Immune-mediated |
| Sulfonamides / sulfonylureas | Notorious for severe thrombocytopenia |
| Rifampin | Drug-dependent antibody |
| Linezolid | Myelosuppression with prolonged use |
| Valacyclovir | TTP mechanism |
| Ganciclovir | Myelosuppression |
| Indinavir | Immune-mediated |
| Fluoroquinolones (levofloxacin, ciprofloxacin) | Immune-mediated + TTP |
Cardiovascular Drugs
| Drug | Notes |
|---|---|
| Heparin | HIT - most important |
| Abciximab, tirofiban, eptifibatide | GPIIb/IIIa inhibitors; conformational neoepitope |
| Aspirin / salicylates | Platelet functional inhibition + immune |
| Digoxin | Immune-mediated |
| Furosemide | Immune-mediated |
Neurological / Psychiatric
| Drug | Notes |
|---|---|
| Valproate | Dose-dependent, usually mild |
| Phenytoin | Immune-mediated |
| Carbamazepine | Myelosuppression / immune |
Oncology / Immunology
| Drug | Notes |
|---|---|
| Cytotoxic chemotherapy (all classes) | Myelosuppression - predictable and dose-dependent |
| Oxaliplatin | Drug-dependent antibody |
| Interferon | Myelosuppression |
| Checkpoint inhibitors (anti-PD1, anti-CTLA4) | True autoantibody induction |
| Anti-CD47 monoclonal antibodies | Direct platelet effect |
GI / Other
| Drug | Notes |
|---|---|
| Cimetidine, ranitidine, famotidine | Immune-mediated |
| Gold salts | Autoantibody (drug-independent) |
| Procainamide | Autoantibody (drug-independent) |
DIIT vs. ITP: Key Distinguishing Features
| Feature | DIIT | ITP |
|---|---|---|
| Onset | Acute, days to weeks after new drug | Gradual over months-years |
| Drug history | Clear temporal relationship | No new drug exposure |
| Recovery after drug stop | Within 1-7 days (most cases) | Persists without treatment |
| Bone marrow | Normal megakaryocytes | Increased megakaryocytes |
| Re-challenge | Confirms diagnosis (rarely done) | Not applicable |
General Management
- Stop all suspected offending drugs - single most important step
- Platelet count typically recovers within days to 1 week after stopping (longer for drugs with long half-lives)
- Platelet transfusion if platelets <10,000-15,000/μL or active bleeding
- If ITP cannot be excluded and thrombocytopenia is life-threatening: consider corticosteroids or IVIG
- For HIT: immediately stop ALL heparin forms; start a direct thrombin inhibitor (argatroban, bivalirudin) or fondaparinux; avoid warfarin until platelets recover; avoid platelet transfusions
- For drug-TTP: stop offending drug + plasma exchange; avoid platelet transfusions
Important exception: Unlike most DIT (which causes bleeding), HIT causes thrombosis - platelet transfusions in HIT are relatively contraindicated as they can fuel further clot formation.
Sources:
- Goldman-Cecil Medicine, International Edition - Table 158-3 and drug-induced thrombocytopenia section
- Robbins, Cotran & Kumar Pathologic Basis of Disease - GPIIb/IIIa conformational change mechanism, HIT pathophysiology
- Rosen's Emergency Medicine - "innocent bystander" mechanism, HIT 4Ts scoring
- Henry's Clinical Diagnosis and Management by Laboratory Methods - drug-dependent vs. drug-independent antibodies
This is a shared conversation. Sign in to Orris to start your own chat.