Scapula fracture documentation for orthopaedic
Reading File
Finding Sources
Searching PubMed
"scapula fracture" AND classification
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative content. Let me compile the full orthopaedic documentation for scapula fractures.
Scapula Fracture - Orthopaedic Documentation
1. Epidemiology & Incidence
Scapular fractures are uncommon, representing approximately 0.4-1% of all fractures and 3-5% of shoulder girdle injuries. Due to the scapula's well-protected position (surrounded by thick musculature, mobile on the chest wall), significant energy is required to fracture it. The majority (88-94%) occur in males, with a mean age in the mid-40s. They are predominantly caused by high-energy trauma - motor vehicle accidents, falls from height, and crush injuries.
- Rockwood and Green's Fractures in Adults 10th ed 2025, Chapter 33
2. Anatomy Relevant to Fractures
The scapula has a highly uneven distribution of bony mass:
- Thickest bone: glenoid, scapular neck (including coracoid base), and lateral border
- Thinnest bone: infraspinous fossa (central biomechanical body), spinomedial angle (most common fracture site)
Two bony pillars transmit compressive forces from the glenoid:
- Lateral pillar: lateral border connecting inferior glenoid to inferior angle
- Spinal pillar: arises from glenoid, continues to the base of the scapular spine
These two pillars form the biomechanical body of the scapula (distinct from the anatomical body). The spinomedial angle - the connection between the scapular spine and the medial border - is the weakest circumferential area, and most scapular body fracture lines pass through this region.
3. Mechanisms of Injury
Scapular fractures result from four basic mechanisms:
| Mechanism | Details |
|---|---|
| Direct blow | Traffic accident, fall from height, heavy object falling onto shoulder - most common; fractures body and upper processes |
| Humeral head impact | Force transmitted through elbow to humerus → glenoid, acromion, lateral spine, or coracoid fracture |
| Glenohumeral dislocation | Anterior dislocation → anteroinferior glenoid rim fracture (most common); posterior dislocation → posterior rim fracture (rare) |
| Violent muscular contracture | Seizures, electrical injury; causes scapular body compression fractures or muscle-insertion avulsions |
Stress fractures: coracoid in overhead athletes; acromion/scapular spine with chronic rotator cuff insufficiency and proximal humeral migration.
- Rockwood and Green's Fractures in Adults 10th ed 2025, pp. 1152-1153
4. Associated Injuries
Scapular fractures are high-energy injuries - approximately 80% have associated injuries:
- Thoracic: rib fractures (most common), pneumothorax, hemothorax; pulmonary contusion in >1/3 of patients
- Vascular: subclavian/axillary artery injury (especially scapulothoracic dissociation)
- Neurological: brachial plexus injury (most commonly upper trunk)
- Ipsilateral upper extremity: clavicle fracture, glenohumeral dislocation, humeral fracture
- Head/neck injury: in high-energy mechanism
Clinical Pearl: Discovery of a scapular fracture on plain chest X-ray in a polytrauma patient should immediately prompt a thorough search for associated life-threatening injuries.
- Schwartz's Principles of Surgery 11th Edition, p. 1911
5. Classification
OTA/AO Classification (Current Standard)
The OTA/AO system classifies scapular fractures under Group 14:
| Code | Type |
|---|---|
| 14F1 | Extra-articular (body, neck, process fractures) |
| 14F2 | Intra-articular (glenoid fossa involvement) |
| 14F2.1 | Simple glenoid fossa fracture (single fracture line, two articular fragments) |
| 14F2.2 | Multifragmentary glenoid fracture (≥3 articular fragments) |
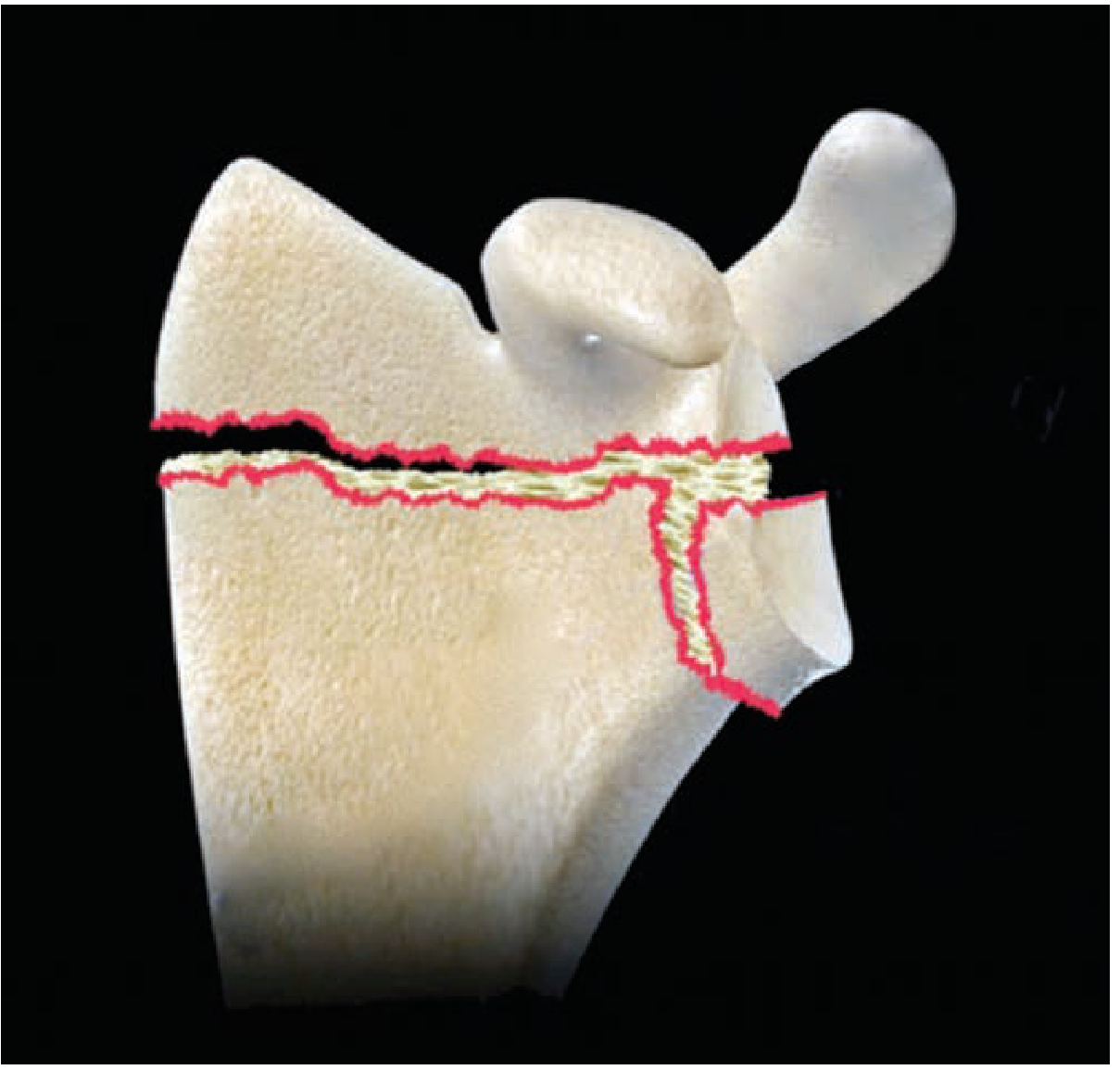
Ideberg Classification (Glenoid Fractures)
| Type | Description |
|---|---|
| I | Anterior rim fracture (IA: avulsion; IB: large fragment) |
| II | Transverse fracture through glenoid fossa extending to lateral border |
| III | Oblique fracture through glenoid extending to superior border (may involve coracoid) |
| IV | Horizontal fracture through body extending to medial border |
| V | Combination of types II + IV (T-fracture through glenoid) |
| VI | Comminuted glenoid fracture |
Ada & Miller Classification (Scapular Neck)
| Type | Description |
|---|---|
| I | Undisplaced neck fracture |
| IIA | Fracture of the surgical neck (glenoid fragment displaces as a unit) |
| IIB | Trans-spinous neck fracture |
| III | Associated with glenoid fracture |
Fracture Type Distribution (Tüček Series of 514 fractures)
| Fracture Type | Frequency | Surgical Rate |
|---|---|---|
| Scapular body | 47% | 25% |
| Glenoid | 25% | 46% |
| Processes (acromion, coracoid, spine) | 23% | lower |
| Neck | 5% | 58% |
- Rockwood and Green's Fractures in Adults 10th ed 2025, pp. 1161-1162
6. Diagnosis
Clinical Presentation
- Pain, swelling, tenderness over the posterior shoulder/scapular region
- Arm held adducted and internally rotated
- Limited and painful shoulder motion
- Possible crepitus on palpation
- Localized bony tenderness over axillary border (suggests body/neck fracture)
- Always examine for associated injuries (chest, neurovascular)
Radiological Algorithm
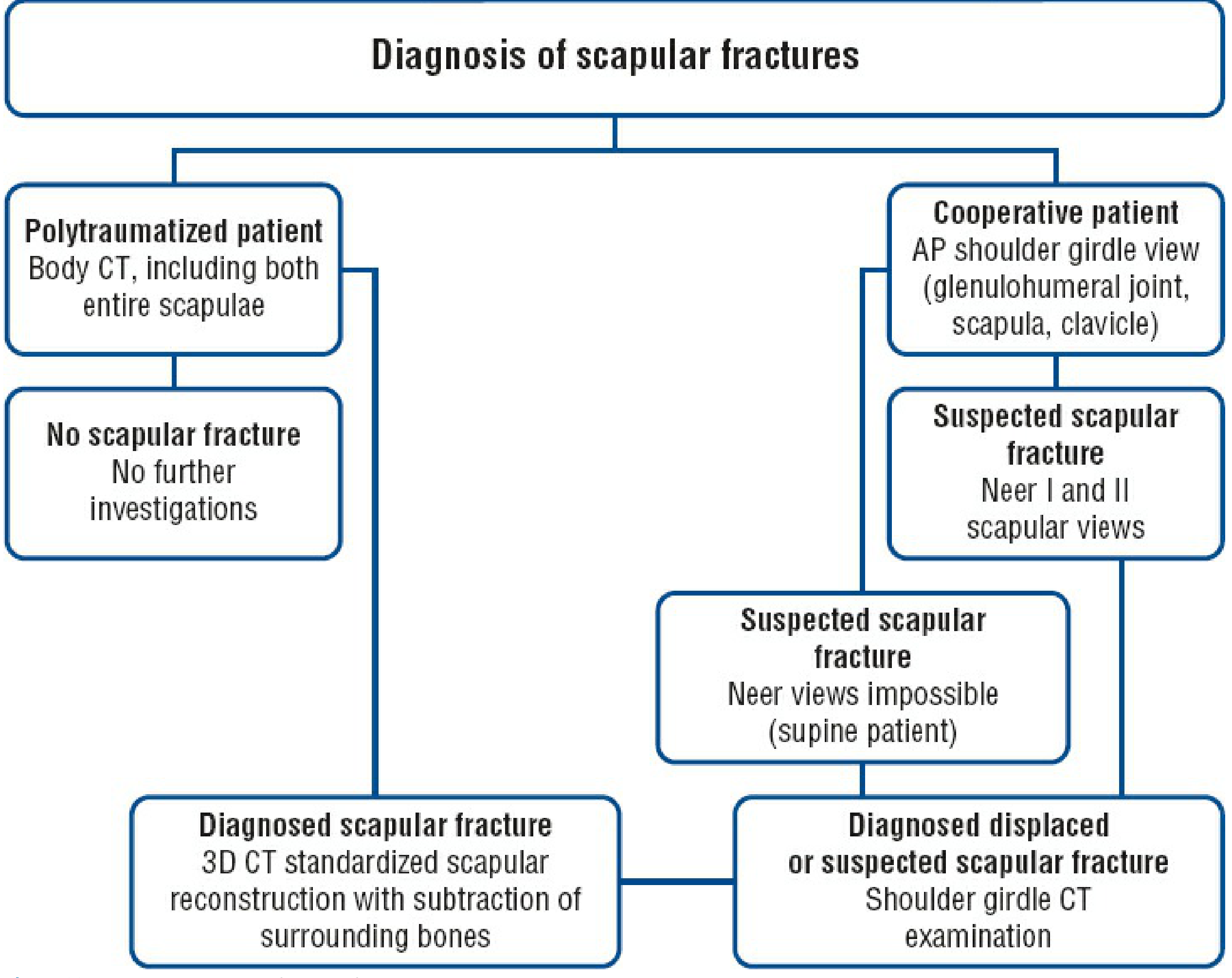
For the cooperative patient:
- AP shoulder girdle view - covers entire scapula, whole clavicle, AC/SC joints, and proximal humerus; general survey but insufficient alone to characterize displacement
- Neer I (True AP of scapula) - assesses glenohumeral joint space, glenoid displacement, and glenopolar angle (GPA)
- Neer II (Scapular Y-view / True lateral) - assesses scapular body in translation, angulation, and fragment overlap
- Axillary view - complementary for glenoid, acromion, and coracoid process fractures
For the polytrauma patient: Body CT covering both entire scapulae is first-line.
CT Examination
CT is now the standard imaging study for scapular fractures:
-
Axial CT: glenoid fossa assessment; reveals undisplaced coracoid and acromion fractures
-
2D CT reconstructions (coronal): glenoid articular surface, especially with coracoid base involvement
-
3D CT reconstructions: most accurate for spatial understanding; essential for surgical planning; subtract surrounding bones for optimal scapular visualization
-
Rockwood and Green's Fractures in Adults 10th ed 2025, pp. 1154-1155
7. Key Displacement Measurements
Four criteria quantify displacement and guide treatment decisions for scapular neck/body fractures:
| Parameter | How Measured | Surgical Threshold |
|---|---|---|
| Mediolateral displacement | Neer I or 3D CT anterior view | ≥9 mm (some use ≥2 cm) |
| Angulation | Neer II or 3D CT lateral view | ≥40-45 degrees |
| Anteroposterior translation | Neer II / lateral 3D CT | No firm consensus |
| Glenopolar Angle (GPA) | Angle between glenoid pole line and glenoid-inferior angle line on Neer I | ≤20-22 degrees |
Normal GPA: 41 degrees (range 35-51 degrees). A GPA ≤20 degrees indicates significant rotational deformity and is associated with poor functional outcomes. Note: GPA may actually increase up to 70 degrees in anatomical neck fractures, so values must be interpreted in context.
- Rockwood and Green's Fractures in Adults 10th ed 2025, pp. 1156-1157
8. Treatment
Non-Operative Treatment (Majority)
Indicated for: undisplaced or minimally displaced fractures (scapular body, neck, most process fractures)
- Sling immobilization for 3-4 weeks for comfort
- Early gentle pendulum exercises from 1-2 weeks
- Progressive range-of-motion and strengthening
- Good/excellent results in approximately 82% of patients with this approach
Surgical Indications
Absolute indications (near universal agreement):
- Displaced glenoid fractures with articular step-off >2-4 mm
- Glenoid rim fractures with glenohumeral subluxation
- Open fractures
- Fractures with associated neurovascular injury requiring exploration
Relative indications (evolving evidence):
- Glenoid medialization/lateral displacement >9 mm
- Scapular body angulation ≥40-45 degrees
- GPA ≤20-22 degrees
- Medial/lateral fragment displacement ≥2 cm
- Floating shoulder (ipsilateral clavicle + scapular neck fracture) with significant displacement
Note: Despite these criteria being widely cited, there are currently no prospective randomized studies confirming the superiority of operative over nonoperative treatment for displaced extra-articular scapular fractures. - Campbell's Operative Orthopaedics 15th Ed 2026, p. 3702
Surgical Approaches
Judet (Posterior) Approach - workhorse for scapular body/neck fractures:
- Patient in semiprone (lateral decubitus) position, injured side up
- Boomerang skin incision: from posterior acromion along scapular spine to spinomedial angle, curving distally along medial border to inferior angle
- Raise skin flap; identify posterior deltoid border
- T-shaped fascial incision along posterior deltoid edge and perpendicular across infraspinatus fascia
- Release spinal portion of deltoid from scapular spine; reflect laterodistally
- Identify and ligate scapular circumflex vessels (3-4 cm distal to inferior glenoid rim, lateral border)
- Detach infraspinatus from all borders; reflect proximally - caution re: suprascapular nerve bundle at spinoglenoid notch
- This exposes entire posterior scapular surface for fracture reduction and fixation
Limited Judet approach: Release only deltoid (not infraspinatus) to reduce dissection for selected fractures.
Anterior (Coracoid/Deltopectoral) approach: For anterior glenoid rim fractures.
- Rockwood and Green's Fractures in Adults 10th ed 2025, pp. 1171-1173
Fixation Methods
- Anatomic locking plates and reconstruction plates along lateral border and/or body
- Lag screws for simple glenoid fractures
- Plate and screw constructs for complex intra-articular glenoid fractures (inferior approach, anterior approach, or combined)
- For glenoid fractures: reduction and fixation aims at restoring congruence and stability
9. Special Patterns
Floating Shoulder
Defined as an ipsilateral fracture of the scapular neck + ipsilateral clavicle fracture that disrupts the Superior Shoulder Suspensory Complex (SSSC) at two points, creating an unstable situation. First described by Ganz & Noesberger; popularized by Herscovici et al.
SSSC components: glenoid, coracoid, CC ligament, lateral clavicle, AC joint, AC ligament, acromion - an osseofibrous ring with two bony struts (middle clavicle; lateral scapular body/spine junction).
Management is controversial; most agree that severely displaced floating shoulders benefit from clavicle fixation to restore SSSC stability, after which the scapular component often reduces acceptably.
Scapulothoracic Dissociation
A lateral displacement of the scapula from the thorax, caused by massive traction force on the upper extremity. Associated with very high rates of brachial plexus injury and subclavian/axillary vessel disruption. Can be identified on AP chest X-ray by asymmetric scapular position. A limb-threatening emergency.
Stress Fractures Post-Reverse Total Shoulder Arthroplasty
Acromial and scapular spine stress fractures are a recognized complication of reverse shoulder arthroplasty (RSA). A 2023 systematic review with meta-analysis (PMID: 37573934) found conservative treatment achieves acceptable outcomes in selected cases.
10. Outcomes & Prognosis
- Non-operative: Good/excellent results in ~82% of patients for undisplaced/minimally displaced fractures
- Operative glenoid fractures: 80% treated surgically with good-to-excellent results in 82%
- Displaced body/neck fractures treated non-operatively: Increasing evidence of unsatisfactory long-term outcomes (pain, limited range of motion, rotator cuff dysfunction) when significant displacement is present
- Scapular malunion: Corrective osteotomy through Judet approach is feasible - Cole et al. reported all five malunion patients became pain-free and returned to their preinjury occupations
Outcome Scores Used:
- Constant-Murley Score (joint-specific)
- DASH / QuickDASH (patient-oriented, upper extremity)
- ASES Score
- Short Form-36 (general health)
Note: No scapula-specific outcome score exists.
11. Complications
| Complication | Notes |
|---|---|
| Malunion | Most common after displaced fractures treated non-operatively; causes rotator cuff impingement, pain, restricted motion |
| Nonunion | Rare for body fractures; more common for process fractures (acromion) |
| Shoulder stiffness | Adhesive capsulitis; prevented by early mobilization |
| Brachial plexus injury | From initial trauma or iatrogenic during Judet approach (suprascapular nerve) |
| Wound complications | Related to posterior approach; relatively low in experienced hands |
| Implant failure | Thin cortex in scapular body limits screw purchase |
Sources:
- Rockwood and Green's Fractures in Adults, 10th Ed (2025), Chapter 33 - Scapular Fractures
- Campbell's Operative Orthopaedics, 15th Ed (2026), Section on Scapula
- Schwartz's Principles of Surgery, 11th Ed, Chapter 43
- S Das: A Manual on Clinical Surgery, 13th Ed
- PMID 37573934: Cui H et al. (2023) - Outcomes of conservative treatment of acromial/scapular spine stress fractures post-RSA
Documentation for casesheet . Examination documentation
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I have everything needed to produce a comprehensive, clinically structured case sheet examination template. Here it is:
SCAPULA FRACTURE - ORTHOPAEDIC CASE SHEET
Examination Documentation
PATIENT DETAILS
| Field | Entry |
|---|---|
| Name | |
| Age / Sex | |
| IP No. / OP No. | |
| Date of Admission | |
| Date of Injury | |
| Mode of Transport | Walk-in / Ambulance / Referred |
| Referred From | |
| Surgeon / Resident |
CHIEF COMPLAINT
Pain / swelling / deformity / inability to move right/left shoulder following __________ [nature of injury] __________ [duration]
HISTORY OF PRESENTING ILLNESS
Onset: Sudden / Gradual
Mode of Injury:
- Road traffic accident (driver / pillion / pedestrian)
- Fall from height (height: ________ feet)
- Direct blow to shoulder
- Fall on outstretched hand (FOOSH)
- Sports injury
- Seizure / electrical injury
- Other: ______________
Details of injury: (direction of force, position of arm at time of injury, speed if RTA)
Dominant hand: Right / Left
Symptoms since injury:
- Pain: Location __________, Severity (/10) __________, constant / intermittent
- Swelling over: scapular region / posterior shoulder / axilla
- Deformity: Yes / No
- Inability to move shoulder: Yes / No
- Numbness / tingling: __________ (distribution)
- Weakness of arm: Yes / No
- Shortness of breath / chest pain: Yes / No
- Any LOC / head injury: Yes / No
Treatment before presentation:
- Sling / splint applied: Yes / No
- Analgesics given: Yes / No
PAST HISTORY
- Previous shoulder problems (rotator cuff, OA, instability): Yes / No - details: __________
- Previous fractures or surgery to same shoulder: Yes / No
- Diabetes / Hypertension / Cardiac disease / Bleeding disorder: Yes / No - details: __________
- Drug history / Allergy: __________
- Rheumatoid arthritis / metabolic bone disease / tumor: Yes / No
- Tetanus immunization status: __________
GENERAL EXAMINATION
| Parameter | Finding |
|---|---|
| Pulse | ________ /min, regular/irregular |
| BP | _________ mmHg (both arms if vascular injury suspected) |
| RR | ________ /min |
| SpO2 | ________% |
| Temperature | ________ °F |
| GCS | E__ V__ M__ = ____/15 |
| Build / Nutrition | |
| Pallor / Icterus / Cyanosis |
LOCAL EXAMINATION
Patient stripped to waist, standing against good daylight, comparing both sides
A. INSPECTION
1. Attitude / Posture on entry
- Arm held: adducted and internally rotated / supported by opposite hand
- Drooping of the affected shoulder: Present / Absent
- Head tilted / neck guarded: Yes / No
2. Look
| Feature | Findings |
|---|---|
| Skin abrasion / contusion | Location: __________ (indicates site of impact) |
| Laceration / open wound | |
| Swelling | Diffuse / Localized - over: posterior shoulder / scapular region / axilla |
| Ecchymosis | Present / Absent - location: __________ |
| Deformity | Flattening / prominence - __________ |
| Muscle wasting | Deltoid / supraspinatus / infraspinatus / other |
| Scapular position | Symmetrical / elevated / laterally displaced (vs. normal side) |
| Chest wall | Visible rib deformity / paradoxical movement |
B. PALPATION
Systematic palpation of the entire shoulder girdle - always compare with the uninjured side
1. Temperature / Tenderness
| Structure | Tender | Swelling | Crepitus |
|---|---|---|---|
| Sternoclavicular (SC) joint | |||
| Clavicle (medial 1/3, middle, lateral 1/3) | |||
| Acromioclavicular (AC) joint | |||
| Acromion process | |||
| Scapular spine | |||
| Spinomedial angle of scapula | |||
| Medial (vertebral) border of scapula | |||
| Inferior angle of scapula | |||
| Axillary (lateral) border of scapula | |||
| Coracoid process (½ inch below clavicle at junction of medial 2/3 and lateral 1/3) | |||
| Glenoid / scapular neck (palpate medial to glenoid cavity) | |||
| Greater tuberosity of humerus | |||
| Bicipital groove | |||
| Axilla and adjacent chest wall |
Key sign: Tenderness and swelling on the axillary border suggests scapular body/neck fracture. In fracture of the neck of scapula: tenderness medial to glenoid + drooping of shoulder + crepitus on axial pressure through flexed elbow (distinguishes from fracture of upper end of humerus).
2. Bony Relationships - Three Bony Point Assessment
(Compare with normal side)
| Relationship | Normal | Affected Side |
|---|---|---|
| Tip of coracoid → acromial end of clavicle | __________ cm | __________ cm |
| Acromial end of clavicle → greater tuberosity | __________ cm | __________ cm |
| Coracoid → greater tuberosity | __________ cm | __________ cm |
In AC dislocation: acromial end of clavicle becomes prominent; coracoid-to-clavicle distance increases. Normal relationships here help confirm isolated scapular injury.
3. Axillary artery pulse: Palpable / Absent / Diminished
4. Scapulothoracic dissociation screening: Asymmetric scapular position vs. contralateral side: Yes / No
C. MEASUREMENTS
1. Arm length (Angle of acromion to lateral epicondyle of humerus)
| Side | Length |
|---|---|
| Normal side | __________ cm |
| Affected side | __________ cm |
| Difference | __________ cm |
Arm length is increased in fracture neck of scapula and subglenoid dislocation (vs. shortened in fracture neck of humerus and anterior dislocation).
2. Vertical circumference of axilla (Bryant's test)
| Side | Measurement |
|---|---|
| Normal | __________ cm |
| Affected | __________ cm |
Increased in dislocation, fracture of upper humerus, and fracture neck of scapula.
3. Hamilton's ruler test:
- Place a straight ruler along lateral arm touching acromion and lateral epicondyle
- Normal: Ruler cannot touch both (greater tuberosity pushes it away)
- Positive (abnormal): Ruler touches both - suggests medial displacement of greater tuberosity (dislocation / significant displacement)
- Result: Positive / Negative
D. MOVEMENTS
Examination of active ROM is often limited by pain; attempt carefully. Passive ROM of glenohumeral joint assessed gently. Stabilize the scapula during glenohumeral ROM assessment.
| Movement | Active (degrees) | Passive (degrees) | Normal |
|---|---|---|---|
| Forward flexion | 0-180° | ||
| Extension | 0-60° | ||
| Abduction | 0-180° | ||
| Adduction | 0-50° | ||
| Internal rotation (behind back level) | T8-T12 | ||
| External rotation (at side) | 0-60° | ||
| Cross-body adduction |
Scapulothoracic rhythm: Normal / Abnormal (early scapular shrug = suggests painful glenohumeral restriction)
Dugas' test:
- Patient attempts to touch opposite shoulder with hand of affected side while keeping arm in contact with chest
- Result: Positive (cannot) / Negative (can) - positive suggests dislocation
E. NEUROVASCULAR EXAMINATION
Critical in all scapular fractures - high energy = high risk of associated nerve/vessel injury
Axillary nerve (most commonly injured in shoulder trauma)
- Sensation over regimental badge area (lower deltoid): Intact / Reduced / Absent
- Deltoid contraction (isometric abduction): Present / Absent
Note: Asking patient to actively abduct shoulder to test axillary nerve is unreliable in acute fracture due to pain. Test the cutaneous territory only.
Brachial plexus screening
| Nerve/Root | Motor Test | Sensation | Result |
|---|---|---|---|
| C5 (axillary + musculocutaneous) | Shoulder abduction, elbow flexion | Lateral arm / lateral forearm | |
| C6 (musculocutaneous / radial) | Wrist extension | Thumb and index finger | |
| C7 (radial) | Finger extension | Middle finger | |
| C8 (ulnar) | Finger abduction | Little finger | |
| T1 (ulnar) | Intrinsic hand muscles | Medial forearm |
Radial pulse: Present / Absent / Diminished
Capillary refill (fingertips): < 2 sec / > 2 sec
Ulnar + radial pulses compared bilaterally: Symmetrical / Asymmetrical
F. CHEST / ASSOCIATED INJURY EXAMINATION
(Mandatory in all high-energy scapular fractures)
| System | Findings |
|---|---|
| Chest auscultation | Air entry: bilateral / reduced on ________ side |
| Percussion | Resonant / Dull / Hyperresonant |
| Rib tenderness | __________ ribs |
| Paradoxical chest movement | Yes / No |
| Tracheal deviation | Central / Deviated to __________ |
| Jugular venous distension | Present / Absent |
| Abdominal tenderness | Yes / No |
| Head / GCS | __________ |
| Contralateral limb injuries | __________ |
INVESTIGATIONS
Radiology
| Imaging | Ordered | Findings |
|---|---|---|
| AP shoulder girdle (entire scapula + clavicle + proximal humerus) | Yes / No | |
| Neer I - True AP of scapula (assess GPA, glenoid displacement) | Yes / No | |
| Neer II - Scapular Y-view / True lateral (angulation, translation, fragment overlap) | Yes / No | |
| Axillary view (glenoid, acromion, coracoid) | Yes / No | |
| AP chest X-ray | Yes / No | |
| CT shoulder + 3D reconstruction (standard for all displaced fractures) | Yes / No | |
| CT chest (polytrauma) | Yes / No |
Glenopolar Angle (GPA) Measurement
(On Neer I view or 3D CT - angle between glenoid pole line and glenoid-to-inferior scapular angle line)
| Parameter | Value |
|---|---|
| Glenopolar Angle (GPA) | ________ degrees (Normal: 35-51°, mean 41°) |
| Mediolateral displacement | ________ mm |
| Angulation on Y-view | ________ degrees |
| Articular step-off (glenoid) | ________ mm |
Lab Investigations
| Test | Result |
|---|---|
| CBC | |
| Blood group & Rh type | |
| RBS | |
| Serum electrolytes | |
| Coagulation profile (PT/INR, aPTT) | |
| Renal function (if operative plan) | |
| ECG | |
| Chest X-ray (PA) |
DIAGNOSIS
Fracture type:
- Scapular body fracture - Undisplaced / Displaced
- Scapular neck fracture - Anatomical / Surgical / Trans-spinous (Ada & Miller type: ______)
- Glenoid fracture - Ideberg type: ______ / OTA type: ______
- Acromion fracture
- Coracoid process fracture
- Scapular spine fracture
- Complex fracture (intra-articular / extra-articular)
- Floating shoulder (ipsilateral clavicle fracture + scapular neck fracture)
- Scapulothoracic dissociation
Side: Right / Left
Open / Closed
Associated injuries:
- Rib fractures: ________
- Pneumothorax / Hemothorax
- Clavicle fracture
- Glenohumeral dislocation
- Humeral fracture
- Brachial plexus injury (level: ________)
- Axillary artery injury
- Other: __________
MANAGEMENT PLAN
Non-operative:
- Sling immobilization (duration: __________)
- Analgesics: __________
- Pendulum exercises from: __________
- Active ROM exercises from: __________
- Physiotherapy referral
Operative indications met:
- Glenoid articular step-off ≥ ________ mm
- GPA ≤ 20-22 degrees (measured: ________)
- Mediolateral displacement ≥ 9 mm (measured: ________)
- Angulation ≥ 40-45 degrees (measured: ________)
- Floating shoulder with significant displacement
- Open fracture
- Associated neurovascular injury
Planned surgical approach:
- Judet (posterior) approach
- Anterior (deltopectoral/coracoid) approach
- Combined approach
- Fixation method: __________ (plates / lag screws / reconstruction plate)
Consent: Obtained / Pending
Pre-op anesthesia review: Done / Pending
Optimization required: __________
OUTCOME SCORE (BASELINE)
(Document at admission; repeat at 6 weeks, 3 months, 6 months, 1 year)
| Score | Baseline | 6 weeks | 3 months | 6 months | 1 year |
|---|---|---|---|---|---|
| Constant-Murley | |||||
| DASH / QuickDASH | |||||
| ASES | |||||
| VAS Pain |
TREATING CLINICIAN SIGNATURE
Name: ________________________
Designation: __________________
Date / Time: __________________
Sources:
- Rockwood and Green's Fractures in Adults, 10th Ed (2025) - Chapter 33 (Signs, Symptoms & Clinical Examination of Scapular Fractures)
- S Das: Manual on Clinical Surgery, 13th Ed - Examination of Injuries About the Shoulder
- Miller's Review of Orthopaedics, 9th Ed - Physical Examination, Shoulder
- Campbell's Operative Orthopaedics, 15th Ed (2026)
This is a shared conversation. Sign in to Orris to start your own chat.