Give me a detailed key myotome , muscle , action , dermatomes in upper limb and lower limb
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the data I need from two authoritative textbooks plus two excellent clinical diagrams. Let me compile the comprehensive answer.
Myotomes, Muscles, Actions & Dermatomes - Upper & Lower Limb
Sources: Miller's Review of Orthopaedics 9th Ed. (Table 8.2 & 8.3) | Harrison's Principles of Internal Medicine 22E (Table 19-1) | Adams & Victor's Neurology 12th Ed.
Upper Limb Neurologic Examination
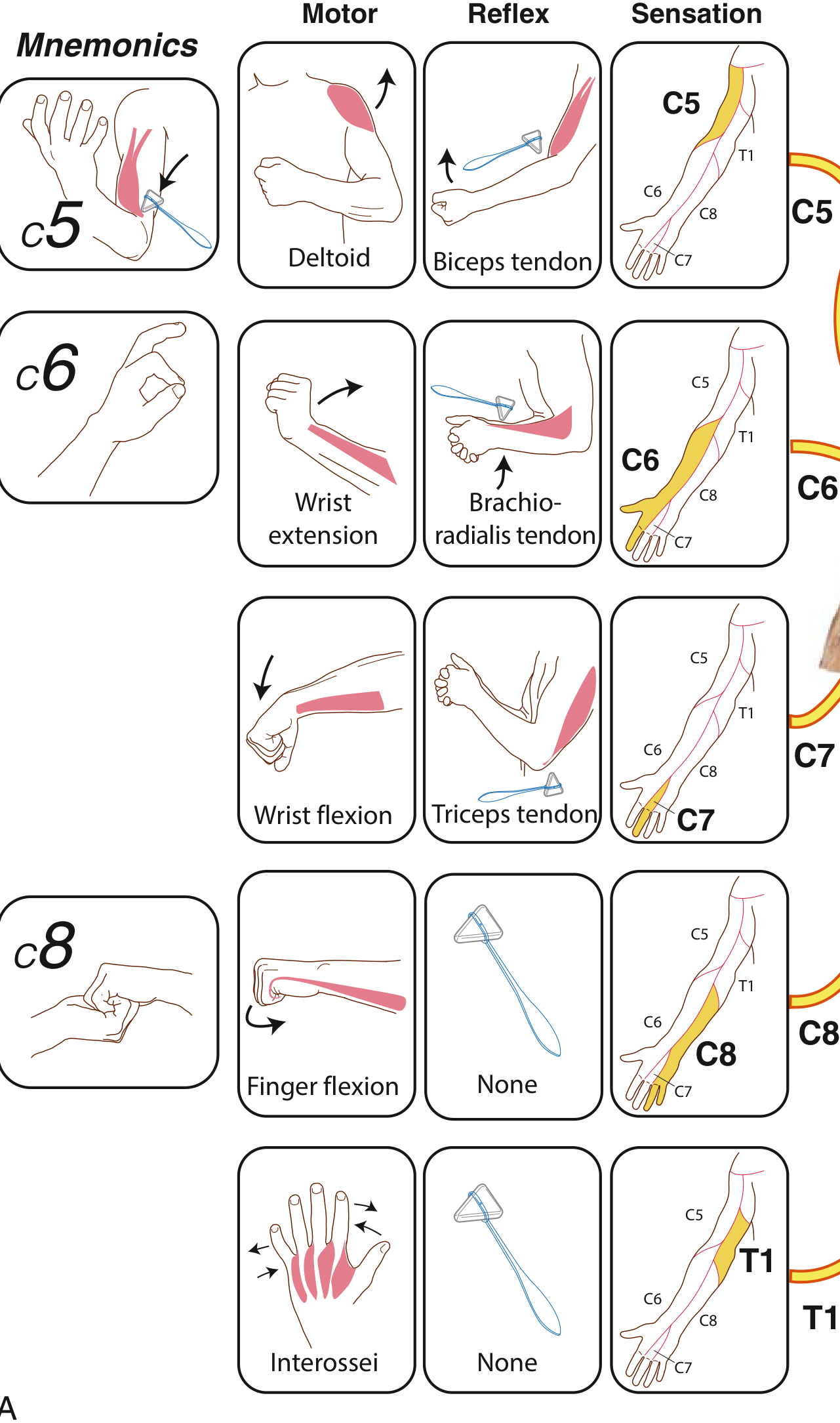
UPPER LIMB - Myotomes & Dermatomes
| Disc Level | Nerve Root | Key Muscles (Myotome) | Action to Test | Dermatome (Sensory Loss) | Reflex |
|---|---|---|---|---|---|
| C3-C4 | C4 | Trapezius, scapular elevators | Shoulder shrug | Lateral neck, shoulder cape area | None |
| C4-C5 | C5 | Deltoid, biceps, rhomboids, infraspinatus | Shoulder abduction (arm raised 30-45° laterally), elbow flexion, external rotation | Lateral arm (over deltoid) | Biceps jerk |
| C5-C6 | C6 | Biceps, brachioradialis, wrist extensors (ECRL, ECRB) | Wrist extension, elbow flexion in supination | Radial forearm, thumb, index finger (palmar) | Brachioradialis jerk |
| C6-C7 | C7 | Triceps, wrist flexors (FCR), pronator teres | Wrist flexion, elbow extension, forearm pronation | Middle finger, dorsal hand/lateral forearm | Triceps jerk |
| C7-T1 | C8 | Finger flexors (FDP, FDS), intrinsics | Finger flexion (grip) | Ulnar hand, ring finger, little finger | None |
| T1-T2 | T1 | Interossei, hypothenar muscles, lumbricals | Finger abduction/adduction | Ulnar forearm, medial arm | None |
Mnemonic Summary - Upper Limb
| Root | Quick Memory Aid |
|---|---|
| C5 | "C5 keeps the deltoid alive" - shoulder abduction |
| C6 | "C6 picks up sticks" - wrist extension, OK sign |
| C7 | "C7 points to heaven" - elbow/wrist extension (triceps) |
| C8 | "C8 grips the plate" - finger flexion |
| T1 | "T1 spreads the bun" - finger abduction (interossei) |
Lower Limb Neurologic Examination
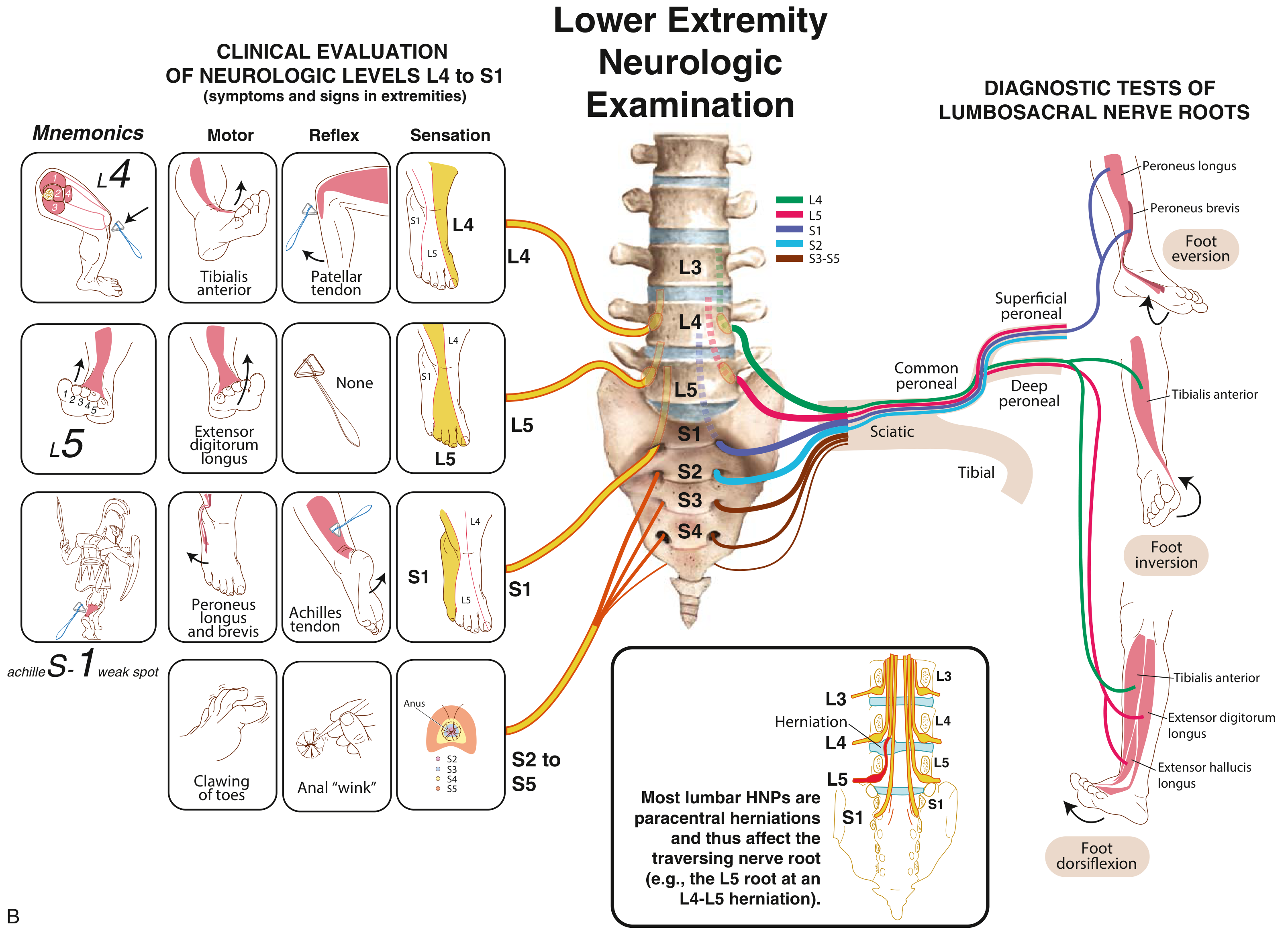
LOWER LIMB - Myotomes & Dermatomes
| Disc Level | Nerve Root | Key Muscles (Myotome) | Action to Test | Dermatome (Sensory Loss) | Reflex |
|---|---|---|---|---|---|
| L1-L3 | L2, L3 | Iliopsoas, hip adductors, sartorius | Hip flexion, hip adduction | Anterior thigh | Cremasteric |
| L3-L4 | L4 | Quadriceps femoris, tibialis anterior | Knee extension, foot dorsiflexion + inversion | Medial calf, medial leg | Knee jerk (patellar) |
| L4-L5 | L5 | Extensor digitorum longus (EDL), extensor hallucis longus (EHL), gluteus medius | Toe extension, big toe extension, foot dorsiflexion, hip abduction | Lateral calf, dorsum of foot | None (occasionally posterior tibialis) |
| L5-S1 | S1 | Gastrocnemius, soleus, peroneus longus & brevis, gluteus maximus | Plantarflexion, foot eversion, hip extension | Posterior calf, lateral foot, plantar foot | Ankle jerk (Achilles) |
| S2-S4 | S2, S3, S4 | Intrinsic foot muscles, bladder/bowel sphincters | Toe clawing, anal sphincter tone | Perianal ("saddle" area) | Bulbocavernosus |
Mnemonic Summary - Lower Limb
| Root | Quick Memory Aid |
|---|---|
| L2, L3 | Psoas (hip flexion) - "2-3 hip flexes free" |
| L4 | "L4 = floor" - foot slaps floor (tibialis anterior) - patellar reflex |
| L5 | "L5 = live" - big toe extension (EHL test), lateral calf |
| S1 | "S1 = one heel raise" - plantarflexion, Achilles reflex |
| S2-S4 | "S2-4 keeps the backdoor shut" - bowel/bladder, perianal |
Full Expanded Muscle Detail by Root
Upper Limb - Expanded
| Root | Muscles | Peripheral Nerve | Primary Action |
|---|---|---|---|
| C5 | Deltoid | Axillary nerve | Shoulder abduction |
| C5 | Biceps brachii | Musculocutaneous | Elbow flexion, forearm supination |
| C5 | Rhomboids | Dorsal scapular | Scapular retraction |
| C5, C6 | Infraspinatus | Suprascapular | External rotation of shoulder |
| C5, C6 | Supraspinatus | Suprascapular | Shoulder initiation of abduction |
| C6 | Brachioradialis | Radial nerve | Elbow flexion (mid-position) |
| C6, C7 | ECRL, ECRB | Radial nerve | Wrist extension (radial) |
| C7 | Triceps brachii | Radial nerve | Elbow extension |
| C7 | FCR (flexor carpi radialis) | Median nerve | Wrist flexion (radial) |
| C7 | Pronator teres | Median nerve | Forearm pronation |
| C7, C8 | FDP, FDS | Median/ulnar | Finger flexion |
| C8 | FCU (flexor carpi ulnaris) | Ulnar nerve | Wrist flexion (ulnar) |
| C8 | Extensor digitorum | Radial nerve | Finger extension |
| T1 | Interossei (dorsal & palmar) | Ulnar nerve | Finger abduction/adduction |
| T1 | Abductor digiti minimi | Ulnar nerve | Little finger abduction |
| T1 | Lumbricals (medial 2) | Ulnar nerve | MCP flexion + IP extension |
Lower Limb - Expanded
| Root | Muscles | Peripheral Nerve | Primary Action |
|---|---|---|---|
| L2, L3 | Iliopsoas | Femoral/direct lumbar | Hip flexion |
| L2, L3 | Hip adductors (adductor longus, magnus) | Obturator nerve | Hip adduction |
| L3, L4 | Quadriceps femoris | Femoral nerve | Knee extension |
| L4 | Tibialis anterior | Deep peroneal nerve | Foot dorsiflexion + inversion |
| L4, L5 | Tibialis posterior | Tibial nerve | Foot inversion |
| L5 | Extensor hallucis longus | Deep peroneal nerve | Big toe extension |
| L5 | Extensor digitorum longus | Deep peroneal nerve | Toe extension + dorsiflexion |
| L5 | Gluteus medius | Superior gluteal nerve | Hip abduction |
| L5, S1 | Peroneus longus & brevis | Superficial peroneal | Foot eversion |
| S1 | Gastrocnemius | Tibial nerve | Plantarflexion (knee straight) |
| S1 | Soleus | Tibial nerve | Plantarflexion (knee bent) |
| S1, S2 | Gluteus maximus | Inferior gluteal nerve | Hip extension |
| S2, S3 | Intrinsic foot muscles | Medial/lateral plantar | Toe movements |
Key Reflexes Summary
| Reflex | Root | Peripheral Nerve |
|---|---|---|
| Biceps jerk | C5 (C6) | Musculocutaneous |
| Brachioradialis jerk | C6 | Radial |
| Triceps jerk | C7 | Radial |
| Finger jerk | C8 | Median/ulnar |
| Patellar (knee jerk) | L3, L4 | Femoral |
| Achilles (ankle jerk) | S1 | Tibial |
| Cremasteric | L1, L2 | Genitofemoral |
| Bulbocavernosus | S2-S4 | Pudendal |
Clinical Tip - Root vs. Peripheral Nerve Lesions
A key teaching point from Adams & Victor's Neurology: a single peripheral nerve usually supplies the complete motor innervation of a muscle, while a single nerve root is shared across multiple peripheral nerves. This means:
- L5 root lesion - weakness of both foot dorsiflexion (deep peroneal) AND foot inversion (tibial), because L5 contributes to both nerves
- Common peroneal nerve lesion - foot dorsiflexion weakness but foot inversion is SPARED, since tibialis posterior (invertor) is supplied via the tibial nerve
This distinction is critical when localizing lesions clinically.
Is tibialis posterior supports foot inversion ?
Finding Sources
Reading File
Reading File
Yes - confirmed by multiple textbooks. Here is the full picture:
Tibialis Posterior and Foot Inversion
Yes, tibialis posterior is the primary invertor of the foot. It is confirmed explicitly in multiple authoritative sources:
"Tibialis posterior (L4-L5) - a plantar flexor and invertor of the foot."
- Localization in Clinical Neurology, 8th Ed.
"Inversion of foot - Roots: L4, L5 - Nerve: Tibial - Muscle: Tibialis posterior"
- Adams & Victor's Principles of Neurology, 12th Ed. (Table 43-1)
Actions of Tibialis Posterior
| Action | Detail |
|---|---|
| Foot inversion | Primary invertor - pulls the sole medially |
| Plantarflexion | Secondary action - assists pointing the foot downward |
| Arch support | Maintains the medial longitudinal arch |
- Root: L4, L5
- Nerve: Tibial nerve (posterior compartment)
- Testing: Ask patient to invert the foot against resistance with the foot in full plantarflexion - this eliminates the contribution of tibialis anterior (which also inverts but is a dorsiflexor)
Why This Distinction Matters Clinically
Both tibialis anterior (deep peroneal nerve, L4) and tibialis posterior (tibial nerve, L4-L5) contribute to inversion, but via different nerves:
| Muscle | Nerve | Root | Also Does |
|---|---|---|---|
| Tibialis anterior | Deep peroneal | L4 | Dorsiflexion + inversion |
| Tibialis posterior | Tibial | L4, L5 | Plantarflexion + inversion |
This is exactly why the L5 root vs. common peroneal nerve distinction mentioned earlier holds up:
- L5 root lesion - weakness of both dorsiflexion (deep peroneal/tibialis anterior) AND inversion (tibial/tibialis posterior) - because L5 feeds both nerves
- Common peroneal lesion - foot drop (dorsiflexion lost) but inversion is preserved - because tibialis posterior runs through the tibial nerve, which is unaffected
Tibialis Posterior Tendon Rupture (Clinical Pearl)
From [Rosen's Emergency Medicine]: when the tibialis posterior tendon ruptures, the peroneus brevis (its antagonist) becomes unopposed, causing:
- Loss of medial arch support
- Valgus deformity of the hindfoot (flat foot / pes planus)
- Classic sign: "too many toes" visible from behind
Where is knee flexion v
Finding Sources
Reading File
Reading File
Finding Sources
Confirmed from multiple textbooks. Here is the complete answer:
Knee Flexion - Nerve Root, Muscles & Nerve
Root Level: L5, S1 (primarily S1)
| Detail | Value |
|---|---|
| Primary roots | L5, S1 (S1 dominant) |
| Muscles | Biceps femoris, semitendinosus, semimembranosus (the hamstrings) |
| Peripheral nerve | Sciatic nerve (tibial division for semi-muscles; common peroneal division for biceps femoris short head) |
| Reflex | Hamstring reflex (medial = L5, lateral = S1) |
The Hamstring Group
| Muscle | Root | Nerve Division | Also Does |
|---|---|---|---|
| Biceps femoris (long head) | L5, S1 | Common peroneal division of sciatic | Hip extension, lateral knee rotation |
| Biceps femoris (short head) | L5, S1 | Common peroneal division of sciatic | Knee flexion only |
| Semitendinosus | L5, S1 | Tibial division of sciatic | Hip extension, medial knee rotation |
| Semimembranosus | L5, S1 | Tibial division of sciatic | Hip extension, medial knee rotation |
Where It Fits in the Full Lower Limb Root Map
| Root | Motor Action |
|---|---|
| L2, L3 | Hip flexion (iliopsoas) |
| L3, L4 | Knee extension (quadriceps) |
| L4 | Foot dorsiflexion + inversion (tibialis anterior) |
| L5, S1 | Knee flexion (hamstrings) |
| S1 | Plantarflexion (gastrocnemius/soleus), foot eversion |
| S1, S2 | Hip extension (gluteus maximus) |
As confirmed by [Goldman-Cecil Medicine]: "L5-S1 - foot plantar flexion, toe flexion, knee flexion, hip extension - Ankle and hamstring reflexes."
Key Clinical Point
- Knee extension = L3, L4 (quadriceps, femoral nerve) - tested by patellar reflex
- Knee flexion = L5, S1 (hamstrings, sciatic nerve) - tested by hamstring reflex
So when you see a patient who cannot flex the knee against resistance, think L5-S1 root lesion or sciatic nerve injury, not femoral nerve.
Superficial reflexes
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Excellent - comprehensive data from Harrison's and Neuroanatomy through Clinical Cases. Here is the full answer:
Superficial Reflexes
Superficial reflexes are cutaneous (skin) reflexes - elicited by stroking or scratching the skin, NOT by tendon tap. They are polysynaptic and require an intact corticospinal tract - they are absent or diminished in UMN lesions (opposite to deep tendon reflexes which are exaggerated in UMN lesions).
Source: Harrison's Principles of Internal Medicine 22E | Neuroanatomy through Clinical Cases 3rd Ed.
Complete Table of Superficial Reflexes
| Reflex | Stimulus | Normal Response | Spinal Segment | Nerve |
|---|---|---|---|---|
| Plantar (Babinski) | Stroke lateral sole heel → ball → big toe | Toe plantarflexion (toes curl down) | S1, S2 | Tibial nerve |
| Upper abdominal | Stroke skin diagonally toward umbilicus (upper quadrant) | Umbilicus pulls toward stimulus | T8, T9, T10 | Intercostal nerves |
| Lower abdominal | Stroke skin diagonally toward umbilicus (lower quadrant) | Umbilicus pulls toward stimulus | T10, T11, T12 | Intercostal nerves |
| Cremasteric | Stroke medial thigh (in males) | Ipsilateral testis elevates | L1, L2 | Genitofemoral nerve |
| Anal (anal wink) | Scratch perianal skin | Contraction of external anal sphincter | S2, S3, S4 | Pudendal nerve |
| Bulbocavernosus | Squeeze glans penis / tug Foley catheter | Anal sphincter contracts | S2, S3, S4 | Pudendal nerve |
| Corneal | Touch cornea with wisp of cotton | Bilateral eye blink | CN V (afferent), CN VII (efferent) | Trigeminal / Facial |
| Palatal (gag) | Touch posterior pharynx | Palate elevation + gag | CN IX (afferent), CN X (efferent) | Glossopharyngeal / Vagus |
The Plantar Response (Babinski) in Detail
| Finding | Meaning |
|---|---|
| Toes flex downward (plantarflexion) | Normal in adults - intact corticospinal tract |
| Big toe extends UP + other toes fan out | Babinski sign = UMN lesion (corticospinal tract damage) |
| Toes silent (no movement) | Treat as abnormal if other side is clearly downgoing |
| Babinski in infants < 1 year | Normal - corticospinal tract not yet myelinated |
"The presence of Babinski's sign in an adult is always abnormal" - Neuroanatomy through Clinical Cases, 3rd Ed.
Abdominal Reflexes - Segmental Localisation
Upper abdominal reflex → T8, T9, T10
Lower abdominal reflex → T10, T11, T12
Clinical use: If upper abdominal reflex is present but lower is absent, the spinal cord lesion lies between T9 and T12 - a very useful localising sign from [Harrison's 22E].
Why Superficial Reflexes Are Absent in UMN Lesions
| Reflex Type | UMN Lesion | LMN Lesion |
|---|---|---|
| Deep tendon reflexes (DTRs) | Exaggerated / hyperreflexia | Absent / diminished |
| Superficial reflexes | Absent | Absent |
| Plantar response | Extensor (Babinski +ve) | Absent or flexor |
Superficial reflexes require an intact corticospinal inhibitory pathway to be expressed. A UMN lesion removes this descending facilitation, so the reflex disappears - while simultaneously releasing DTRs from inhibition (hence hyperreflexia).
Primitive Reflexes (Frontal Release Signs)
These superficial reflexes reappear in adults with frontal lobe disease:
| Reflex | Stimulus | Response |
|---|---|---|
| Grasp reflex | Touch palm between thumb and index finger | Forced grip of examiner's hand |
| Suck reflex | Touch centre of lips | Sucking movement |
| Root reflex | Touch corner of lips | Lips move toward stimulus |
| Palmomental | Stroke thenar eminence | Ipsilateral chin muscle contraction |
| Glabellar tap | Tap glabella repeatedly | Persistent blinking (normally habituates) |
This is a shared conversation. Sign in to Orris to start your own chat.