Add additional information and rewrite according to text book
Mean u can add additional information for the above topic
Summarise give points wise include images and flow chart for pg orthopaeics 10 marks answer
cd /home/daytona/workspace/attachments/28ea324d-8bd7-440b-8e82-7a5874c77abd/ && …
sideswipe elbow injury management outcome
complex elbow fracture open injury management
Medical flowchart titled "Algorithmic Management of Sideswipe Elbow Injuries" showing the following decision tree: Start box "SIDESWIPE INJURY" → "TRIAGE: Secure Airway, Breathing, Circulation" → two branches: "OPEN INJURY" and "CLOSED INJURY". Open injury branch → "Gustilo-Anderson Classification" → Grade 1 & 2 → "Debridement + Inter/External Fix" → Grade 3 → "Debridement + External Fixator". Closed injury branch → "Internal Fixation". Both converge at "Assess Vascular Status" → two paths: "Vascular Injury" (→ End-to-end repair / Vein graft) and "Vessel Intact". Both converge at "Redebridement (24-48h)" → "Soft Tissue Coverage" → Split skin graft / Latissimus dorsi flap / Free tissue transfer. Then → "Secondary Procedures" → Bone grafting / Nerve repair or graft / Tendon transfer / Free fibula for bone loss >5cm. Final box: "Rehabilitation & Physiotherapy → Functional outcome assessed by Mayo Elbow Performance Score". Clean professional medical diagram with blue color scheme, white background, clear arrows and boxes.
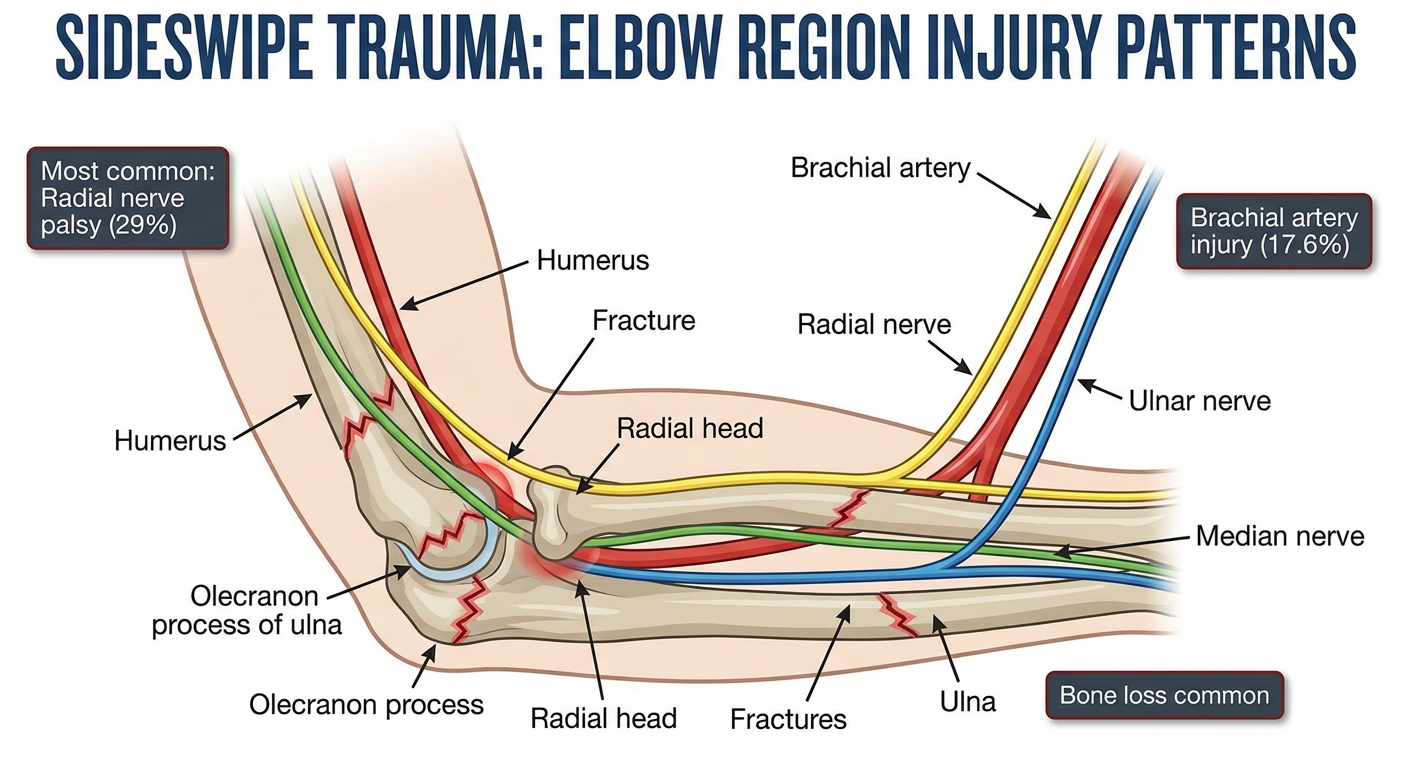
Medical anatomy diagram showing elbow region with labeled injury patterns in sideswipe trauma. Show the humerus, radius, ulna, olecranon, radial head, brachial artery, radial nerve, ulnar nerve, and median nerve. Highlight in red the common fracture sites: supracondylar humerus fracture, olecranon fracture, radial head dislocation, radius and ulna fractures. Also label the neurovascular structures at risk. Include small annotation boxes showing "Most common: Radial nerve palsy (29%)", "Brachial artery injury (17.6%)", "Bone loss common". Professional medical illustration style, clean white background, labeled diagram suitable for orthopedic surgery textbook.
Medical classification table diagram showing Gustilo-Anderson Classification of Open Fractures. Three rows: Grade I - wound less than 1cm, minimal contamination, simple fracture pattern; Grade II - wound 1-10cm, moderate contamination, moderate comminution; Grade III - wound more than 10cm, high contamination, severe comminution with three sub-types: IIIA (adequate soft tissue coverage), IIIB (periosteal stripping, bone exposure, requires flap), IIIC (vascular injury requiring repair). Show management implications for each grade. Professional medical table format with color coding, blue and white scheme, clean orthopedic textbook style.
Sideswipe Injuries Around the Elbow
Management and Functional Evaluation - PG Orthopaedics 10-Mark Answer
1. Definition and Mechanism
- Sideswipe injury (synonyms: "baby car injury," "traffic elbow injury") occurs when a passenger travelling in a vehicle with the elbow resting outside the window is struck by an oncoming vehicle or object.
- Almost all are high-energy, open injuries - a subgroup of complex elbow trauma.
- Most common in countries where passengers travel in open-window buses/cars.
- Patients typically present with polytrauma - commonly associated head, chest injuries.
- All injuries are sustained by road traffic accidents (100% in the reported series).
- The right (dominant) side is more commonly affected.
2. Epidemiology (Kharbanda et al., IJO 2013 - Series of 34 patients)
| Parameter | Finding |
|---|---|
| Male : Female | 32 : 2 |
| Age range | 8-48 years (mean 30 years) |
| Right side affected | 20/34 |
| Open injuries | 22/34 (Gustilo-Anderson classified) |
| Closed injuries | 12/34 |
| Average Injury Severity Score | 24 |
| Mean follow-up | 74 months (range 15-94 months) |
3. Injury Pattern - What Makes it "Complex"?
- Comminuted supracondylar fracture of humerus with intraarticular extension
- Fracture of olecranon at coronoid level
- Anterior dislocation of radial head
- Fracture of radius and ulna (both bones forearm)
- Fracture shaft of humerus
- All accompanied by variable degree of bone loss
- Concomitant elbow dislocation (3 patients)
| Nerve/Vessel | n | Type | Procedure |
|---|---|---|---|
| Radial nerve | 10 | Neuropraxia (2), Division (2), Segmental loss (6) | Observe / End-to-end / Tendon transfer |
| Ulnar nerve | 2 | Neuropraxia | Observation |
| Median nerve | 4 | Division (2 nerve graft, 2 end-to-end repair) | Graft / Repair |
| Brachial artery | 6 | Contusion (1), Division (2), Avulsion/Segmental loss (3) | Observe / Resection + Vein graft |
- Radial nerve palsy is the most common nerve injury (29%) - not ulnar, as in some series
- Vascular injury in 17.6% of patients
- Brachial plexus injury: nil in this series
4. Management Algorithm (Staged, Multispecialty Protocol)
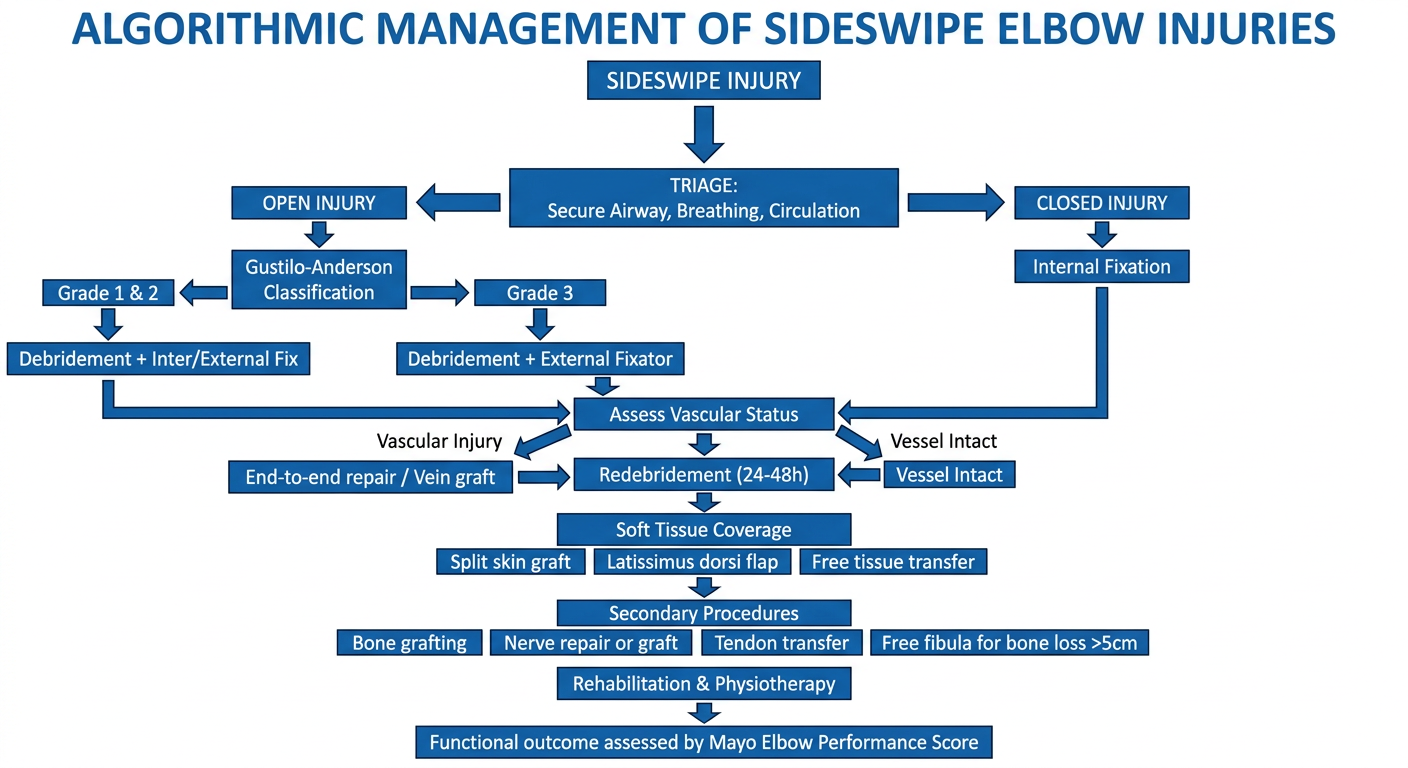
Step-by-Step Protocol:
- Secure airway, breathing, circulation
- ATLS guidelines followed
- IV antibiotics started at arrival
- Joint assessment by all three specialties in triage
- Decision on salvageability of limb
- Thorough wound lavage with 4-5 L normal saline in all open fractures
- Aseptic dressing and splintage
- Primary thorough debridement
- Team redrapes and rescrubs before fixation
- External fixator used in open fractures, marked comminution, bone loss, extensive soft tissue damage, and multiple injury (damage control orthopaedics)
- Used in 20/34 patients (18/22 open + 2 closed)
- Internal fixation preferred in closed fractures and clean Grade I & II open fractures
- Used in 16/34 patients (12 closed + 4 open)
- External fixator is converted to internal fixation after wound coverage
- Transfixation of elbow joint NOT used in this series (though used by Morrey et al. in severe comminution)
- After bony fixation, vascular status is reassessed
- End-to-end anastomosis or vein graft performed (5 cases)
- Compartment syndrome: not seen in this series
- Carried out after vascular repair to achieve bleeding margins
- Repeat after 24-48 hours before any soft tissue cover
- Early coverage prevents tissue necrosis and bone death
- Authors advocate early split skin grafting as biological dressing
5. Gustilo-Anderson Classification of Open Fractures
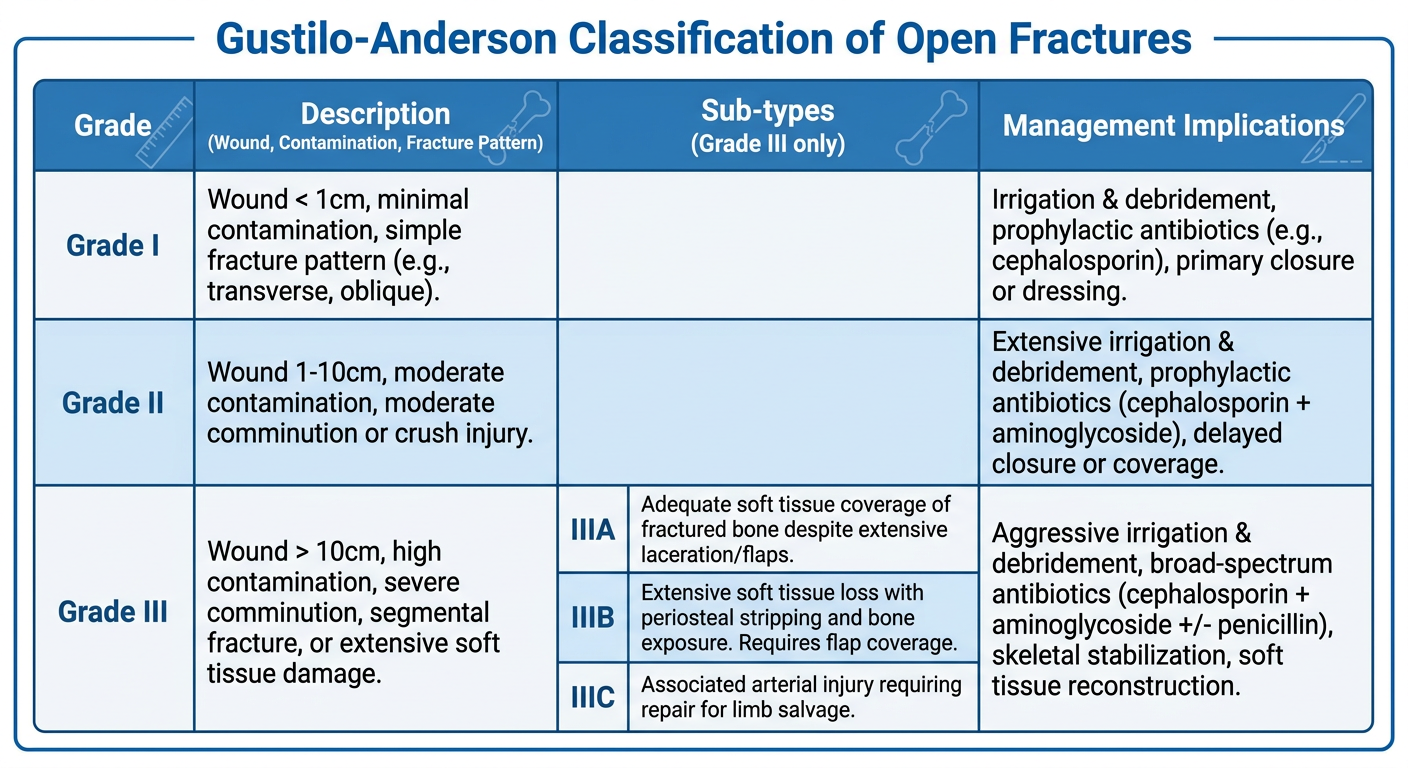
- Grade I & II: Internal fixation preferred
- Grade III: External fixation - staged approach
6. Soft Tissue Coverage Options
| Defect | Procedure |
|---|---|
| Skin loss | VAC / Split skin graft |
| Skin + muscle loss | Muscle transposition + skin grafting |
| Large defects | Latissimus dorsi myocutaneous flap |
| Bone + tissue loss | Free tissue transfer |
| Nonunion | Plating + bone grafting |
| Bone loss < 5 cm (humerus) | Docking technique |
| Bone loss > 5 cm (humerus) | Free fibular transfer + plate fixation |
- Pedicled latissimus dorsi flaps used for defects not extending more than 8 cm below elbow (Stevanovic et al.)
- Free tissue transfer done in 4 patients
7. Elbow Anatomy and Injury Diagram
8. Secondary (Delayed) Procedures
| Procedure | n | Indication |
|---|---|---|
| Bone grafting | 8 | Nonunion |
| Tendon transfer (Modified Jones) | 6 | Radial nerve segmental loss, Volkmann's ischemic contracture |
| Free fibular transfer | 4 | Bone loss > 5 cm |
| Extensor mechanism repair | 1 | Extensor disruption |
- Brachioradialis → Flexor pollicis longus
- Extensor carpi radialis → Flexor digitorum profundus
- Done at average 6 months after injury
- All regained good hand function (writing, holding glass, tying buttons)
- Primary nerve repair in 4 cases (2 radial + 2 median)
- Segmental nerve loss: grafting deferred until soft tissue healing complete
- All ulnar nerve neuropraxias: recovered with observation (3-6 months)
9. Complications
| Complication | n | Management |
|---|---|---|
| Pin tract infection | Common | Wound lavage + IV antibiotics |
| Infection (deep) | 2 | Debridement + IV antibiotics 6 weeks + VAC |
| Blow out of repaired artery | 2 | Vein graft |
| Devascularization of forearm muscles | 2 | Debridement |
| Volkmann's ischemic contracture | 2 | Tendon transfer |
| Nonunion (most common late complication) | 8 | Autogenous corticocancellous bone grafting |
| Ankylosis of elbow | 2 | None / Accepted |
| Arthrodesis (in free fibula cases) | 4 | Planned outcome |
| Amputation (above elbow) | 2 | Failed limb salvage |
10. Results - Mayo Elbow Performance Score (MEPS)
| Score | Category | % of Patients |
|---|---|---|
| > 90 | Excellent | 30% (9 patients) |
| 75-89 | Good | 33% (10 patients) |
| 60-74 | Fair | - |
| < 60 | Poor | 6 patients (fused elbows) |
- Average MEPS = 70 (fair-to-good range)
- Limb salvage: 32/34 (94%) - 2 required above-elbow amputation
- Average elbow ROM in best outcomes: 30-130° (functional range)
- Open fractures
- Associated nerve injuries (most significant - Seekamp et al.)
- Soft tissue loss
- Bone loss
- External fixation as primary stabilization
- Poor rehabilitation
11. Key Teaching Points (PG Exam Mnemonics)
Debridement → Vascular repair → Redebridement → Soft tissue cover → Secondary procedures → Closure/Rehab
- Open fracture with contamination
- Marked comminution
- Bone loss
- Extensive soft tissue damage
- Polytrauma / damage control
Open fracture + Nerve injury + Bone loss = Poor functional outcome
12. Conclusion
- Sideswipe injuries are complex, high-energy, open elbow injuries requiring a multispecialty algorithmic approach
- Limb salvage is achievable in ~94% of cases with timely, aggressive management
- A staged surgical protocol is mandatory: debridement → stabilization → vascular repair → soft tissue cover → delayed secondary procedures
- Radial nerve palsy is the most common neural complication; nonunion is the most common late complication
- Nerve injury is the single most important predictor of poor functional outcome
- Average MEPS of 70 reflects the inherent severity of these injuries despite optimal management