Hyponatremia cause management and diagnostic approach in details with reference from harrison , davidson and uptodate
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Searching PubMed
hyponatremia diagnosis treatment guidelines
Reading File
Reading File
Loading Image
Reading File
Excellent! I now have comprehensive material from Harrison's 22e and Comprehensive Clinical Nephrology 7e covering all aspects - etiology, pathophysiology, clinical features, diagnosis, and management. I also have both diagnostic algorithm images. Let me now compose the full detailed response.
Hyponatremia: Comprehensive Review
Sources: Harrison's Principles of Internal Medicine, 22nd Edition (2025); Comprehensive Clinical Nephrology, 7th Edition; Brenner and Rector's The Kidney; recent PubMed literature
1. Definition and Epidemiology
Hyponatremia is defined as a plasma Na⁺ concentration <135 mmol/L. It is the most common electrolyte disorder, occurring in up to 22% of hospitalized patients. Severity is classified as:
| Category | Serum Na⁺ |
|---|---|
| Mild | 130-134 mmol/L |
| Moderate | 125-129 mmol/L |
| Severe | <125 mmol/L (symptomatic risk high at <120) |
(Harrison's 22e, Chapter 56; Comprehensive Clinical Nephrology 7e, Chapter 9)
2. Pathophysiology
The kidney can normally excrete up to 20-30 L of free water per day. Hyponatremia almost always reflects a defect in urinary dilution - either from:
- Increased AVP (arginine vasopressin/ADH) activity - the most common mechanism. AVP binds V2 receptors on collecting duct principal cells, inserting aquaporin-2 water channels, increasing water reabsorption.
- Reduced distal delivery of filtrate - decreased GFR or increased proximal reabsorption limits the volume of fluid reaching the diluting segment.
- Impaired NaCl transport in the thick ascending limb (TAL) or distal convoluted tubule - reduces the ability to generate dilute urine.
"Hyponatremia is almost always the result of an increase in circulating AVP and/or increased renal sensitivity to AVP, combined with an intake of free water." - Harrison's 22e
Brain adaptation: Acutely, water moves into brain cells down the osmotic gradient, causing cerebral edema. The brain compensates by extruding Na⁺, K⁺, Cl⁻ (rapid phase, minutes-hours), then organic osmolytes - creatine, betaine, glutamate, myoinositol, taurine (slower phase, complete by ~48 h). This explains why correction of chronic hyponatremia must be cautious - the depleted osmolytes cannot be quickly replenished, and rapid correction causes osmotic demyelination.
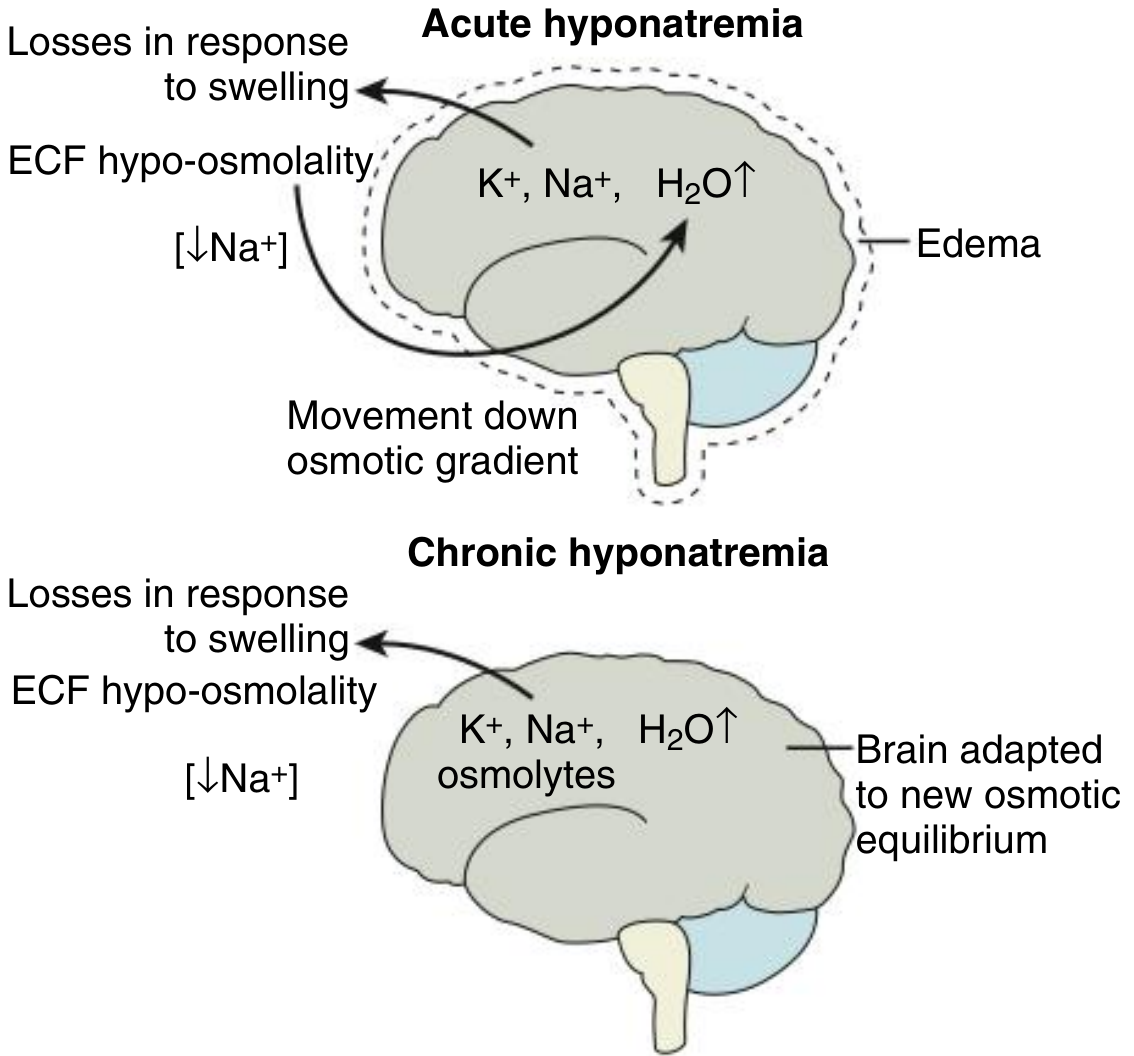
Fig: Brain volume adaptation - acute vs chronic hyponatremia (Comprehensive Clinical Nephrology 7e, Fig 9.7)
3. Classification and Causes
The cornerstone of the diagnostic approach is classifying hyponatremia by volume status (confirmed by history, physical examination, and urine Na⁺).
Diagnostic Algorithm
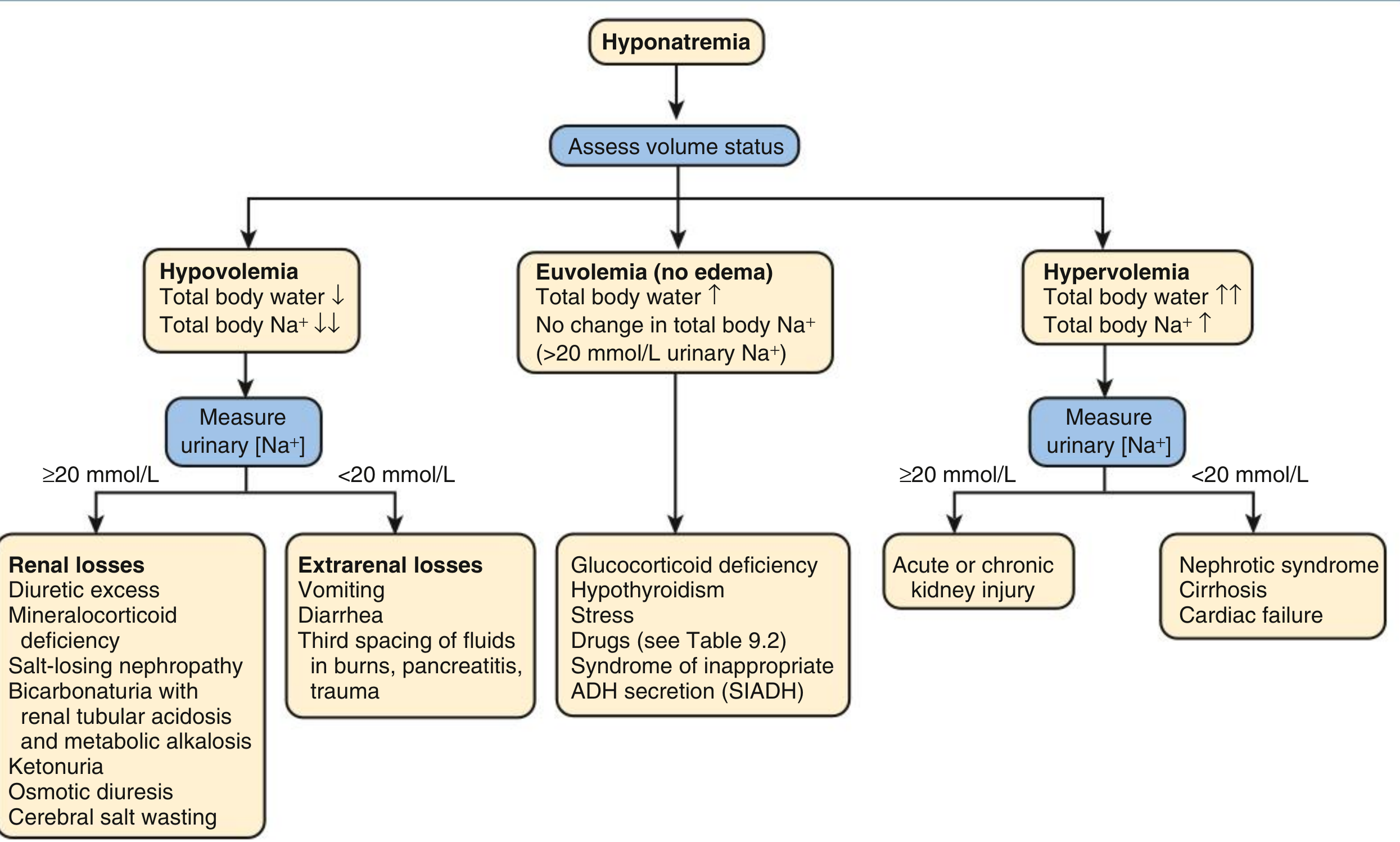
Fig 9.5: Diagnostic algorithm for hyponatremia - Comprehensive Clinical Nephrology 7e
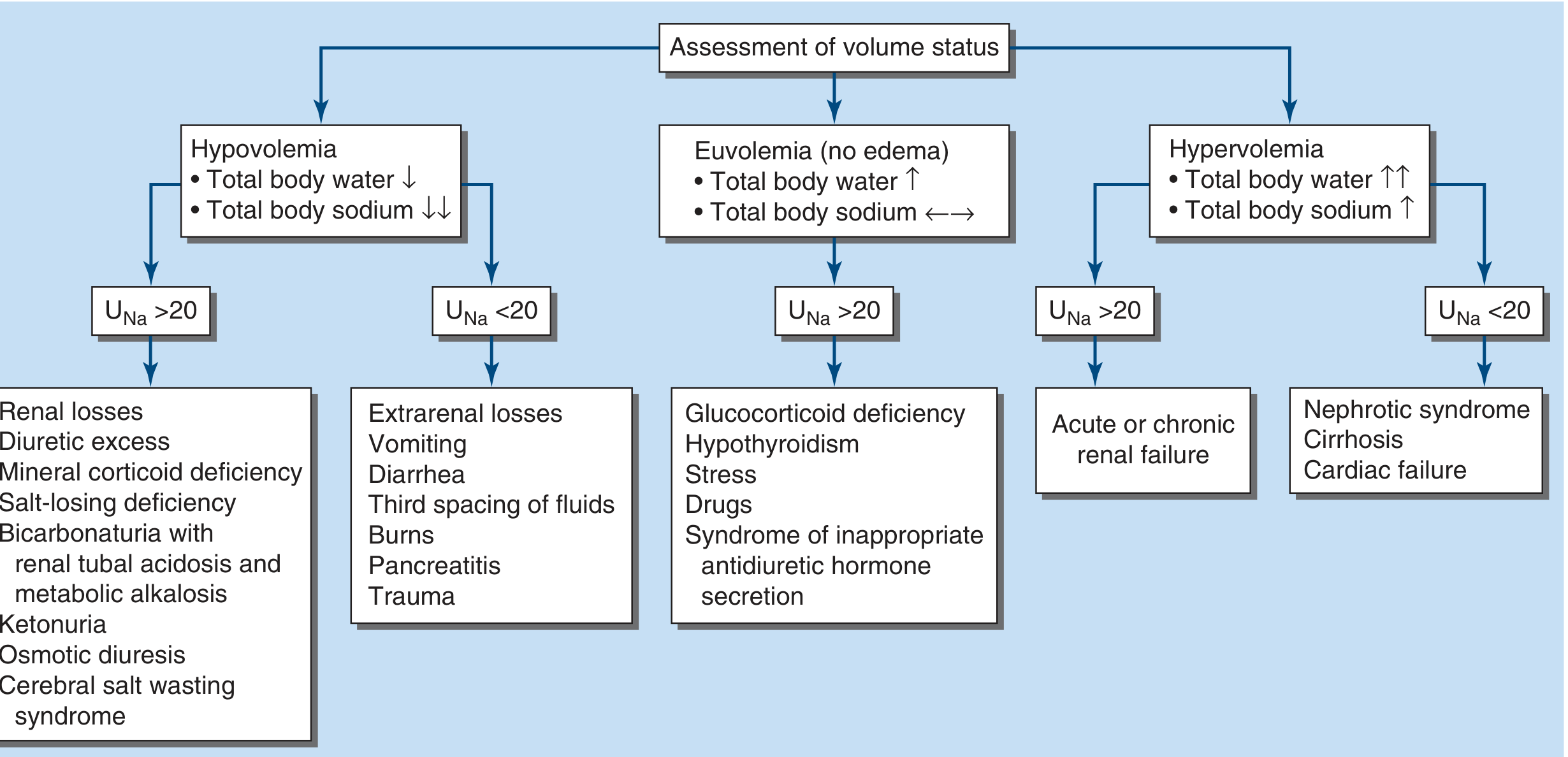
FIGURE 56-5: The diagnostic approach to hyponatremia - Harrison's 22e
A. Hypovolemic Hyponatremia
Physiology: Total body Na⁺ and water both reduced, but Na⁺ deficit exceeds water deficit. Volume depletion stimulates nonosmotic AVP release, driving water retention.
Urine Na⁺ <20 mmol/L (Extrarenal losses):
- Gastrointestinal: vomiting, diarrhea, tube drainage
- Skin/insensible: burns, sweating
- Third-space sequestration: peritonitis, pancreatitis, ileus
- Exception: vomiting with metabolic alkalosis - bicarbonaturia obliges Na⁺ excretion, so urine Na⁺ may be >20 despite hypovolemia; use urine Cl⁻ instead (<10 mmol/L confirms extrarenal loss)
Urine Na⁺ >20 mmol/L (Renal losses):
- Thiazide diuretics (most common) - multiple mechanisms: polydipsia, volume depletion, direct impairment of renal dilution. Presentations mimic SIAD.
- Salt-losing nephropathies: reflux nephropathy, interstitial nephritis, post-obstructive uropathy, medullary cystic disease, recovery phase of ATN
- Primary adrenal insufficiency (Addison's) - aldosterone deficiency; hallmark is hyponatremia + hyperkalemia + hypotension + high urine Na⁺
- Bicarbonaturia: renal tubular acidosis, metabolic alkalosis
- Ketonuria (alcoholic ketoacidosis, starvation ketosis)
- Osmotic diuresis
- Cerebral salt wasting (CSW): rare, associated with SAH, TBI, craniotomy, meningitis, encephalitis. Critical to distinguish from SIAD because CSW requires aggressive Na⁺-Cl⁻ repletion (not fluid restriction).
(Harrison's 22e; Comprehensive Clinical Nephrology 7e)
B. Euvolemic Hyponatremia
Physiology: Total body water increased, total body Na⁺ normal or near-normal. No overt edema. Urine Na⁺ typically >20 mmol/L.
Causes:
- SIAD (Syndrome of Inappropriate Antidiuresis) - most common cause of euvolemic hyponatremia
- Hypothyroidism (moderate to severe)
- Secondary adrenal insufficiency (glucocorticoid deficiency - pituitary disease; in contrast to primary adrenal insufficiency which is hypovolemic)
- Stress (post-operative, pain, nausea)
- Drugs (see Table below)
SIAD - Detailed
Diagnostic Criteria (Harrison's 22e, Table 56-1):
- Plasma osmolality <275 mOsm/kg
- Urine osmolality >100 mOsm/kg (usually >300)
- Clinical euvolemia (no overt dehydration, no edema, ascites)
- Urine Na⁺ >20-30 mmol/L on normal salt/water intake
- Normal thyroid and adrenal function
- Recent diuretic therapy excluded
Causes of SIAD:
| Category | Examples |
|---|---|
| CNS | Stroke, SAH, meningitis, encephalitis, Guillain-Barre, head injury, psychosis |
| Pulmonary | Pneumonia, TB, abscess, COPD exacerbation, positive pressure ventilation, empyema |
| Malignancy | Small cell lung carcinoma, carcinoid, lymphoma, mesothelioma, GI/GU tumors (ectopic AVP production) |
| Drugs | Thiazides, SSRIs, TCAs, carbamazepine, oxcarbazepine, vincristine, cyclophosphamide, chlorpropamide, clofibrate, NSAIDs, opiates, MDMA, haloperidol |
| Endocrine | Hypothyroidism, glucocorticoid deficiency |
| Other | Postoperative state, pain, nausea, HIV/AIDS, hereditary (gain-of-function V2 receptor mutations) |
Four AVP patterns in SIAD:
- Random/erratic AVP secretion
- Reset osmostat (AVP released at lower threshold, responds normally once triggered)
- Unsuppressible low-level AVP leak
- AVP-independent water channel activation (nephrogenic SIAD)
C. Hypervolemic Hyponatremia
Physiology: Total body Na⁺ and water both increased, but water excess exceeds Na⁺ excess. "Arterial underfilling" despite volume expansion drives nonosmotic AVP release.
Urine Na⁺ <10 mmol/L:
- Congestive heart failure (CHF) - cardiac dysfunction reduces effective arterial filling
- Hepatic cirrhosis - peripheral vasodilation reduces effective arterial blood volume
- Nephrotic syndrome - hypoalbuminemia with third-space losses
Urine Na⁺ >20 mmol/L:
- Acute kidney injury (AKI)
- Chronic kidney disease (CKD) - impaired ability to dilute urine
"The degree of hyponatremia provides an indirect index of the associated neurohumoral activation and is an important prognostic indicator in hypervolemic hyponatremia." - Harrison's 22e
D. Pseudohyponatremia and Translocational Hyponatremia
Pseudohyponatremia (isotonic/hypertonic): Spuriously low Na⁺ from laboratory artifact in severe hyperlipidemia or hyperproteinemia (displacement of aqueous phase). Serum osmolality is normal.
Translocational hyponatremia (hypertonic): Osmotically active solutes (glucose, mannitol, sorbitol, glycine from TURP irrigant) draw water from cells, diluting Na⁺. For every 100 mg/dL rise in glucose above normal, Na⁺ falls ~1.6-2.4 mmol/L. True osmolality is not low.
4. Causes of Acute Hyponatremia (Harrison's Table 56-2)
| Cause |
|---|
| Postoperative hypotonic fluids (especially premenopausal women) |
| Hypotonic IV fluids with any cause of elevated AVP |
| Glycine irrigation (TURP, uterine surgery) |
| Colonoscopy preparation |
| Thiazide diuretics (recent institution) |
| Primary polydipsia |
| MDMA ("Ecstasy," "Molly") ingestion |
| Exercise-associated hyponatremia (marathons, endurance events) |
| Multifactorial (e.g., thiazide + polydipsia) |
5. Clinical Features
By Severity
| Severity | Na⁺ | Symptoms |
|---|---|---|
| Mild/asymptomatic | >125 | Usually none; subtle gait/cognitive defects may be present |
| Moderate | 120-125 | Headache, nausea, yawning, lethargy, reversible ataxia |
| Severe | <120 | Psychosis, seizures, coma, respiratory failure, brain herniation |
Acute vs Chronic
Acute hyponatremia (<48 h): Cerebral edema is the predominant danger. Neurologic symptoms develop rapidly - nausea, headache, vomiting, seizures, coma, brainstem herniation, and death. Normocapneic respiratory failure from neurogenic pulmonary edema can occur. Women (especially premenopausal) are far more susceptible - estrogen inhibits the brain's osmolyte extrusion response.
Chronic hyponatremia (>48 h): Brain has already adapted via organic osmolyte loss. Risk of cerebral edema is less. However, patients are at risk of osmotic demyelination syndrome (ODS) if corrected too rapidly. Even "asymptomatic" chronic hyponatremia causes subtle cognitive impairment, gait instability, and increased fall risk - all reversible with correction.
"Even patients who are judged 'asymptomatic' can manifest subtle gait and cognitive defects that reverse with correction of hyponatremia." - Harrison's 22e
Osmotic Demyelination Syndrome (ODS) / Central Pontine Myelinolysis (CPM)
- Results from too-rapid correction of chronic hyponatremia
- Brain cells depleted of osmolytes cannot rapidly reaccumulate them; osmotic stress causes myelin destruction
- Symptoms: dysarthria, dysphagia, spastic quadriparesis, pseudobulbar palsy, "locked-in" syndrome, coma
- Risk factors: serum Na⁺ <105 mmol/L, alcoholism, malnutrition, liver disease, hypokalemia, burns
- MRI shows characteristic T2 hyperintensity in pons (+/- extrapontine)
- Not uniformly fatal - some neurologic recovery possible
6. Diagnostic Approach
Step 1: Confirm True Hyponatremia
- Measure serum osmolality
- Low (<275 mOsm/kg): true hypotonic hyponatremia (proceed to Step 2)
- Normal (275-290): pseudohyponatremia (lipemia, paraproteinemia) - check with direct ion-selective electrode
- High (>290): translocational (hyperglycemia, mannitol, sorbitol, glycine)
Step 2: Assess Volume Status
Clinical examination:
- Hypovolemia: dry mucous membranes, skin turgor reduced, tachycardia, orthostatic hypotension, flat neck veins, recent vomiting/diarrhea/diuretic use
- Euvolemia: no edema, no signs of dehydration
- Hypervolemia: edema, ascites, elevated JVP, S3 gallop, crackles in lungs
Step 3: Urine Studies
- Urine osmolality: >100 mOsm/kg suggests AVP-mediated water retention (SIAD, heart failure, etc.); <100 mOsm/kg suggests primary polydipsia or low solute intake
- Urine Na⁺ concentration:
| Urine Na⁺ | Interpretation |
|---|---|
| <10-20 mmol/L | Extrarenal Na⁺ loss or Na⁺-avid hypervolemic state (CHF, cirrhosis, nephrotic syndrome) |
| >20-40 mmol/L | Renal Na⁺ loss, SIAD, hypothyroidism, adrenal insufficiency, AKI/CKD |
- Note: Vomiting with metabolic alkalosis - use urine Cl⁻ instead (urine Cl⁻ <10 mmol/L = extrarenal volume depletion despite high urine Na⁺ from bicarbonaturia)
Step 4: Additional Tests (to find cause)
- Serum glucose, BUN, creatinine, lipids, protein (exclude pseudo/translocational)
- Thyroid function tests (TSH, free T4) - exclude hypothyroidism
- Morning cortisol or ACTH stimulation test - exclude adrenal insufficiency
- Serum potassium (hyperkalemia suggests Addison's)
- Serum uric acid (low in SIAD; high or normal in CSW, hypovolemia)
- Liver function tests, albumin, proBNP/BNP
- Chest X-ray, CT chest/abdomen (if SIAD - to find malignancy, pulmonary cause)
- Fractional excretion of urate (FEUA): elevated in SIAD (>12%), helps distinguish from CSW
SIAD vs Cerebral Salt Wasting - Key Distinction (Bradley & Daroff's Neurology)
| Parameter | SIAD | CSW |
|---|---|---|
| ECF volume | Increased/euvolemic | Decreased |
| Body weight | Increased | Decreased |
| Fluid balance | Positive | Negative |
| Urine volume | Normal or decreased | Normal or increased |
| Tachycardia | Absent | Present |
| Hematocrit | Normal | Increased |
| Albumin | Normal | Increased |
| Serum bicarbonate | Normal or low | Increased |
| BUN | Normal or low | Increased |
| Serum uric acid | Low | Normal or low |
| Urinary Na⁺ | High | High |
| CVP/PCWP | Normal or slightly high | Low |
Treatment implication: SIAD - fluid restriction; CSW - aggressive NaCl repletion. Confusing the two is dangerous.
7. Management
General Principles (Harrison's 22e)
The rate of correction depends on:
- Acuity (acute <48 h vs chronic >48 h)
- Severity of symptoms
- Risk factors for ODS
Safe correction limits (UpToDate / European Guidelines):
- Maximum correction: 10-12 mmol/L per 24 hours (conservative 8-10 mmol/L/24h if high ODS risk)
- Maximum in first 24 hours: 10 mmol/L
- Do not exceed 18 mmol/L in 48 hours
- In highest ODS-risk patients (Na⁺ <105, alcoholism, malnutrition, liver disease): target ≤8 mmol/L/24h
A. Acute Symptomatic Hyponatremia (Seizures, Coma)
This is a medical emergency. The risk of acute cerebral edema exceeds the risk of ODS.
Treatment (Comprehensive Clinical Nephrology 7e / Harrison's 22e):
- 3% NaCl (hypertonic saline)
- Initial: 1-2 mL/kg IV over 60 minutes, OR
- 100 mL IV bolus over 10 minutes, repeated up to 3 times if symptoms persist
- If severe neurological symptoms (seizures, coma): 4-6 mL/kg/hr
- Target: Rapid increment of 4-6 mmol/L in the first 6 hours - sufficient to reverse acute cerebral edema; correction to normal is not necessary
- Add furosemide (loop diuretic) to enhance free water excretion
- Monitor serum electrolytes every 2 hours
- Monitor neurological and pulmonary status closely
Formula for estimating Na⁺ change from 1L infusate (Adrogué-Madias):
ΔNa⁺ = (Infusate Na⁺ - Serum Na⁺) / (Total body water + 1)
- 3% NaCl contains ~513 mmol/L Na⁺
- 0.9% NaCl contains ~154 mmol/L Na⁺
B. Chronic Symptomatic Hyponatremia
If duration >48 h or unknown - correction must be cautious (see Fig 9.8 from Nephrology text).
Management algorithm:
- Moderate symptoms (nausea, confusion, headache without seizures):
- 3% NaCl at low rate (0.5-1 mL/kg/hr)
- Target: raise Na⁺ by 1-2 mmol/L/hour until symptoms improve
- Stop or slow once Na⁺ increases by 8-10 mmol/L or reaches 125-130 mmol/L, whichever comes first
- No acute symptoms:
- Treat underlying cause first
- Fluid restriction, salt supplementation per etiology
If overcorrection occurs ("rescue"):
- Stop all hypertonic saline
- Give DDAVP 2-4 mcg IV to clamp further correction
- Give D5W (5% dextrose in water) to relower Na⁺ back to safe range
- Re-lower Na⁺ to 8-10 mmol/L below the overcorrected level
(A 2026 systematic review, PMID 41652262, confirms that sodium overcorrection in chronic hyponatremia is associated with adverse neurological outcomes and higher mortality, reinforcing strict limits.)
C. Hypovolemic Hyponatremia
- Isotonic saline (0.9% NaCl) is the primary treatment
- Volume repletion suppresses AVP, leading to a water diuresis and Na⁺ correction
- Warning: In patients with urine Na⁺ <20 and AVP-driven hyponatremia, normal saline can cause rapid overcorrection as AVP drops precipitously - monitor closely
D. Hypervolemic Hyponatremia (CHF, Cirrhosis, Nephrotic)
- Treat the underlying disease (optimize heart failure therapy, manage cirrhosis)
- Fluid restriction (1-1.5 L/day)
- Loop diuretics (furosemide) - increase free water excretion
- Vasopressin V2 receptor antagonists (Vaptans):
- Tolvaptan (oral) or Conivaptan (IV)
- Block AVP effect on collecting duct, causing selective aquaresis (electrolyte-free water excretion)
- Approved for hypervolemic and euvolemic hyponatremia
- Contraindicated in: hypovolemic hyponatremia, liver disease (tolvaptan carries hepatotoxicity risk - avoid in cirrhosis), urgent need for rapid correction
- Avoid fluid restriction during vaptan therapy
- Risk of overcorrection - initiate in hospital with monitoring
E. Euvolemic Hyponatremia - SIAD Management
Step 1: Treat the underlying cause
- Withdraw causative drugs
- Treat infection, malignancy, CNS disease
Step 2: Fluid restriction
- First-line: restrict fluid to <800-1000 mL/day
- Success depends on urine osmolality - if urine Osm >500 or urine Osm > 2× serum Osm, fluid restriction alone is often insufficient
Step 3: Additional measures (when fluid restriction fails)
- Salt tablets + loop diuretic (furosemide): increases solute excretion, effective for long-term management
- Urea (oral): 15-60 g/day in water - increases renal free water excretion; European guidelines rate this highly; inexpensive
- Demeclocycline: induces nephrogenic DI; slow onset (days-weeks); nephrotoxic - rarely used now
- Tolvaptan: effective but caution re: overcorrection, cost, and liver toxicity - not for routine use in cirrhosis-associated SIAD
F. Special Situations
Hypothyroidism: Correct thyroid hormone - Na⁺ normalizes with treatment (avoid overly aggressive Na⁺ correction while awaiting thyroid hormone effect)
Adrenal insufficiency:
- Primary (Addison's): hydrocortisone + fludrocortisone; saline repletion
- Secondary: hydrocortisone replacement alone; Na⁺ rapidly improves
Beer potomania / low solute intake hyponatremia:
- Massive fluid intake with very low solute diet (beer has little Na⁺ or protein)
- Kidney cannot excrete sufficient free water due to lack of solute
- Treatment: increase dietary solute intake; stop excessive fluid intake; sodium/urea supplementation
Exercise-associated hyponatremia:
- Caused by excess free water intake during endurance events + nonosmotic AVP
- Prevention: drink only to thirst; avoid plain water in favor of electrolyte drinks
- Severe cases: 3% NaCl
8. Summary Table: Quick Reference
| Parameter | Hypovolemic | Euvolemic | Hypervolemic |
|---|---|---|---|
| Total body water | ↓ | ↑ | ↑↑ |
| Total body Na⁺ | ↓↓ | Normal | ↑ |
| Urine Na⁺ | <20 (extrarenal) / >20 (renal) | >20 | <10 (CHF/cirrhosis) / >20 (AKI/CKD) |
| Urine Osm | High | High | Variable |
| Typical causes | Diarrhea, vomiting, burns, diuretics, Addison's | SIAD, hypothyroid, sec. adrenal insuff | CHF, cirrhosis, nephrotic, AKI/CKD |
| Treatment | IV NS (0.9%), correct cause | Fluid restriction, treat cause, vaptans/urea | Fluid restriction, diuretics, vaptans, treat cause |
9. Recent Evidence (2024-2026)
- [PMID 41652262] - A 2026 systematic review and meta-analysis confirmed that sodium overcorrection in chronic hyponatremia is associated with significantly worse neurological outcomes and mortality, validating strict 10 mmol/L/24h correction limits.
- [PMID 41058069] - A 2026 systematic review in pediatric neurological illness found that fractional excretion of urate (FEUA), urinary phosphate, and BNP are useful biomarkers for distinguishing CSW from SIAD, reducing reliance on volume assessment alone.
Note on Davidson's: Davidson's Principles and Practice of Medicine is not in the current textbook library. The content above draws from Harrison's 22e (2025), Comprehensive Clinical Nephrology 7e, and Bradley & Daroff's Neurology, which cover SIAD and hyponatremia in equivalent or greater depth. For UpToDate-specific content, the management thresholds (10 mmol/L/24h cap, vaptan use, urea therapy in SIAD) cited above align with current UpToDate recommendations per the European Clinical Practice Guideline framework (Spasovski et al., 2014, Eur J Endocrinol).
Make in pdf form , note like
Reading File
Running Command
ls /home/daytona/workspace/ 2>/dev/null || mkdir -p /home/daytona/workspace/hypo…
Running Command
mkdir -p /home/daytona/workspace/hyponatremia-notes && python3 -c "import report…
Writing File
~/hyponatremia-notes/build_pdf.py
"""
Hyponatremia Medical Notes PDF Generator
Styled like clinical study notes: colored headers, tables, boxes, icons
"""
from reportlab.lib.pagesizes import A4
from reportlab.lib import colors
from reportlab.lib.units import cm, mm
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.platypus.flowables import Flowable
from reportlab.pdfgen import canvas
from reportlab.lib.colors import HexColor
import io
# ── Colour palette ────────────────────────────────────────────────────────────
C_NAVY = HexColor("#1A3A5C")
C_BLUE = HexColor("#2563EB")
C_LIGHT_BLUE= HexColor("#DBEAFE")
C_TEAL = HexColor("#0F766E")
C_TEAL_LIGHT= HexColor("#CCFBF1")
C_ORANGE = HexColor("#EA580C")
C_ORANGE_LT = HexColor("#FFF7ED")
C_RED = HexColor("#DC2626")
C_RED_LIGHT = HexColor("#FEF2F2")
C_GREEN = HexColor("#16A34A")
C_GREEN_LT = HexColor("#F0FDF4")
C_YELLOW = HexColor("#CA8A04")
C_YELLOW_LT = HexColor("#FEFCE8")
C_PURPLE = HexColor("#7C3AED")
C_PURPLE_LT = HexColor("#F5F3FF")
C_GREY = HexColor("#64748B")
C_GREY_LT = HexColor("#F8FAFC")
C_GREY_MED = HexColor("#E2E8F0")
C_WHITE = colors.white
C_BLACK = HexColor("#0F172A")
# ── Custom flowables ──────────────────────────────────────────────────────────
class ColorBox(Flowable):
"""A colored background box with left accent bar."""
def __init__(self, content_paragraphs, bg_color, bar_color, width=None, pad=8):
Flowable.__init__(self)
self.content = content_paragraphs
self.bg = bg_color
self.bar = bar_color
self.w = width or (A4[0] - 3.5*cm)
self.pad = pad
self._h = None
def wrap(self, avail_w, avail_h):
self.w = avail_w
inner_w = self.w - 6 - self.pad*2
total_h = self.pad
for p in self.content:
_, ph = p.wrap(inner_w, avail_h)
total_h += ph + 2
total_h += self.pad
self._h = total_h
return self.w, self._h
def draw(self):
c = self.canv
# background
c.setFillColor(self.bg)
c.roundRect(0, 0, self.w, self._h, 4, fill=1, stroke=0)
# left bar
c.setFillColor(self.bar)
c.rect(0, 0, 5, self._h, fill=1, stroke=0)
# content
inner_w = self.w - 6 - self.pad*2
y = self._h - self.pad
for p in self.content:
_, ph = p.wrap(inner_w, self._h)
y -= ph
p.drawOn(c, 6 + self.pad, y)
y -= 2
c.setFillColor(C_BLACK)
class SectionHeader(Flowable):
"""Full-width colored section header bar."""
def __init__(self, text, bg=C_NAVY, fg=C_WHITE, height=22, icon=""):
Flowable.__init__(self)
self.text = icon + " " + text if icon else text
self.bg = bg
self.fg = fg
self.h = height
def wrap(self, aw, ah):
self.w = aw
return aw, self.h
def draw(self):
c = self.canv
c.setFillColor(self.bg)
c.roundRect(0, 0, self.w, self.h, 5, fill=1, stroke=0)
c.setFillColor(self.fg)
c.setFont("Helvetica-Bold", 11)
c.drawString(10, 6, self.text)
class SubHeader(Flowable):
"""Smaller sub-section header."""
def __init__(self, text, bg=C_BLUE, fg=C_WHITE, height=18):
Flowable.__init__(self)
self.text = text
self.bg = bg
self.fg = fg
self.h = height
def wrap(self, aw, ah):
self.w = aw
return aw, self.h
def draw(self):
c = self.canv
c.setFillColor(self.bg)
c.roundRect(0, 0, self.w, self.h, 3, fill=1, stroke=0)
c.setFillColor(self.fg)
c.setFont("Helvetica-Bold", 9.5)
c.drawString(8, 5, self.text)
class TwoColLayout(Flowable):
"""Two-column layout for compact side-by-side content."""
def __init__(self, left_items, right_items, col_headers=("",""), h_bg=(C_TEAL, C_ORANGE)):
Flowable.__init__(self)
self.left = left_items
self.right = right_items
self.col_headers = col_headers
self.h_bg = h_bg
# ── Page template ─────────────────────────────────────────────────────────────
def make_header_footer(canvas_obj, doc):
"""Running header/footer on every page."""
canvas_obj.saveState()
w, h = A4
# Top bar
canvas_obj.setFillColor(C_NAVY)
canvas_obj.rect(0, h-1.1*cm, w, 1.1*cm, fill=1, stroke=0)
canvas_obj.setFillColor(C_WHITE)
canvas_obj.setFont("Helvetica-Bold", 9)
canvas_obj.drawString(1*cm, h-0.75*cm, "HYPONATREMIA — Clinical Study Notes")
canvas_obj.setFont("Helvetica", 8)
canvas_obj.drawRightString(w-1*cm, h-0.75*cm,
"Harrison's 22e | Comprehensive Nephrology 7e | UpToDate")
# Bottom bar
canvas_obj.setFillColor(C_GREY_MED)
canvas_obj.rect(0, 0, w, 0.8*cm, fill=1, stroke=0)
canvas_obj.setFillColor(C_GREY)
canvas_obj.setFont("Helvetica", 7.5)
canvas_obj.drawString(1*cm, 0.25*cm,
"For educational use only | Orris AI Medical Notes | July 2026")
canvas_obj.drawRightString(w-1*cm, 0.25*cm, f"Page {doc.page}")
canvas_obj.restoreState()
# ── Style helpers ─────────────────────────────────────────────────────────────
def styles():
base = getSampleStyleSheet()
S = {}
S['body'] = ParagraphStyle('body',
fontName='Helvetica', fontSize=8.5, leading=13,
textColor=C_BLACK, spaceAfter=3, spaceBefore=2)
S['body_sm'] = ParagraphStyle('body_sm',
fontName='Helvetica', fontSize=7.8, leading=11.5,
textColor=C_BLACK, spaceAfter=2)
S['bold'] = ParagraphStyle('bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_BLACK)
S['blue_bold'] = ParagraphStyle('blue_bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_BLUE)
S['red_bold'] = ParagraphStyle('red_bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_RED)
S['teal_bold'] = ParagraphStyle('teal_bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_TEAL)
S['orange_bold'] = ParagraphStyle('orange_bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_ORANGE)
S['purple_bold'] = ParagraphStyle('purple_bold',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_PURPLE)
S['title_main'] = ParagraphStyle('title_main',
fontName='Helvetica-Bold', fontSize=26, leading=32,
textColor=C_WHITE, alignment=TA_CENTER)
S['title_sub'] = ParagraphStyle('title_sub',
fontName='Helvetica', fontSize=11, leading=16,
textColor=HexColor("#BFDBFE"), alignment=TA_CENTER)
S['quote'] = ParagraphStyle('quote',
fontName='Helvetica-Oblique', fontSize=8, leading=12,
textColor=C_TEAL, leftIndent=6)
S['bullet'] = ParagraphStyle('bullet',
fontName='Helvetica', fontSize=8.5, leading=13,
textColor=C_BLACK, leftIndent=12, firstLineIndent=-8,
spaceAfter=2)
S['bullet_sm'] = ParagraphStyle('bullet_sm',
fontName='Helvetica', fontSize=7.8, leading=11,
textColor=C_BLACK, leftIndent=12, firstLineIndent=-8,
spaceAfter=1)
S['table_hdr'] = ParagraphStyle('table_hdr',
fontName='Helvetica-Bold', fontSize=8, leading=11,
textColor=C_WHITE, alignment=TA_CENTER)
S['table_cell'] = ParagraphStyle('table_cell',
fontName='Helvetica', fontSize=7.8, leading=11,
textColor=C_BLACK)
S['table_cell_b'] = ParagraphStyle('table_cell_b',
fontName='Helvetica-Bold', fontSize=7.8, leading=11,
textColor=C_BLACK)
S['warn'] = ParagraphStyle('warn',
fontName='Helvetica-Bold', fontSize=8.5, leading=13,
textColor=C_RED)
S['center'] = ParagraphStyle('center',
fontName='Helvetica', fontSize=8.5, leading=13,
textColor=C_BLACK, alignment=TA_CENTER)
return S
# ── Table helper ──────────────────────────────────────────────────────────────
def make_table(data, col_widths, hdr_bg=C_NAVY, alt_row=True, fontsize=7.8):
"""Build a styled reportlab Table."""
S = styles()
# Convert strings to Paragraphs
table_data = []
for ri, row in enumerate(data):
p_row = []
for ci, cell in enumerate(row):
if ri == 0:
st = S['table_hdr']
else:
st = S['table_cell']
p_row.append(Paragraph(str(cell), st))
table_data.append(p_row)
t = Table(table_data, colWidths=col_widths, repeatRows=1)
style_cmds = [
('BACKGROUND', (0,0), (-1,0), hdr_bg),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 8),
('GRID', (0,0), (-1,-1), 0.4, C_GREY_MED),
('ROWBACKGROUNDS', (0,1), (-1,-1),
[C_WHITE, HexColor("#F1F5F9")] if alt_row else [C_WHITE]),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
('RIGHTPADDING', (0,0), (-1,-1), 5),
('ROWBACKGROUNDS', (0,0), (-1,0), [hdr_bg]),
]
t.setStyle(TableStyle(style_cmds))
return t
def bullet(text, style_key='bullet', s=None):
if s is None: s = styles()
return Paragraph(f"• {text}", s[style_key])
def sp(n=4):
return Spacer(1, n)
# ── COVER PAGE ────────────────────────────────────────────────────────────────
def cover_page(story, S):
# Spacer to push down
story.append(Spacer(1, 2.5*cm))
# Title card (manual drawing via canvas-like table trick)
title_data = [[Paragraph("HYPONATREMIA", S['title_main'])]]
t = Table(title_data, colWidths=[17*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), C_NAVY),
('ROUNDEDCORNERS', [8]),
('TOPPADDING', (0,0), (-1,-1), 22),
('BOTTOMPADDING', (0,0), (-1,-1), 8),
('LEFTPADDING', (0,0), (-1,-1), 10),
]))
story.append(t)
sub_data = [[Paragraph(
"Cause • Diagnostic Approach • Management", S['title_sub'])]]
t2 = Table(sub_data, colWidths=[17*cm])
t2.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), C_BLUE),
('TOPPADDING', (0,0), (-1,-1), 10),
('BOTTOMPADDING', (0,0), (-1,-1), 14),
]))
story.append(t2)
story.append(sp(12))
# Source badge row
badge_data = [[
Paragraph("<b>Harrison's 22e</b><br/>(2025)", S['center']),
Paragraph("<b>Comp. Nephrology 7e</b>", S['center']),
Paragraph("<b>UpToDate 2026</b>", S['center']),
Paragraph("<b>PubMed Evidence</b>", S['center']),
]]
badge_t = Table(badge_data, colWidths=[4.25*cm]*4)
badge_t.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), C_TEAL),
('BACKGROUND', (1,0), (1,0), C_BLUE),
('BACKGROUND', (2,0), (2,0), C_ORANGE),
('BACKGROUND', (3,0), (3,0), C_PURPLE),
('TEXTCOLOR', (0,0), (-1,-1), C_WHITE),
('FONTNAME', (0,0), (-1,-1), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 9),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 10),
('BOTTOMPADDING', (0,0), (-1,-1), 10),
('GRID', (0,0), (-1,-1), 1, C_WHITE),
('ROUNDEDCORNERS', [4]),
]))
story.append(badge_t)
story.append(sp(14))
# Quick summary box
summary_items = [
Paragraph("<b>DEFINITION:</b> Plasma Na⁺ < 135 mmol/L | Most common electrolyte disorder", S['body']),
Paragraph("<b>PREVALENCE:</b> Up to 22% of hospitalized patients", S['body']),
Paragraph("<b>KEY MECHANISM:</b> Excess AVP activity + free water intake (>90% of cases)", S['body']),
Paragraph("<b>CLASSIFICATION:</b> Hypovolemic | Euvolemic | Hypervolemic (by volume status)", S['body']),
Paragraph("<b>DANGER:</b> Acute → cerebral edema | Rapid correction → osmotic demyelination", S['body']),
]
story.append(ColorBox(summary_items, C_LIGHT_BLUE, C_BLUE))
story.append(sp(10))
# Date/Author row
meta = [[ Paragraph("Prepared: July 2026", S['body_sm']),
Paragraph("Orris AI Medical Notes", S['body_sm']),
Paragraph("Educational Use Only", S['body_sm']) ]]
mt = Table(meta, colWidths=[5.67*cm]*3)
mt.setStyle(TableStyle([
('TEXTCOLOR', (0,0), (-1,-1), C_GREY),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('GRID', (0,0), (-1,-1), 0.3, C_GREY_MED),
('TOPPADDING', (0,0), (-1,-1), 5),
('BOTTOMPADDING', (0,0), (-1,-1), 5),
]))
story.append(mt)
story.append(PageBreak())
# ── SECTION 1: DEFINITION & PATHOPHYSIOLOGY ──────────────────────────────────
def section_patho(story, S):
story.append(SectionHeader("1. DEFINITION, EPIDEMIOLOGY & PATHOPHYSIOLOGY", C_NAVY, icon="📌"))
story.append(sp(6))
# Severity table
story.append(SubHeader("Severity Classification", C_TEAL))
story.append(sp(4))
sev_data = [
["Category", "Serum Na⁺", "Clinical Risk"],
["Mild", "130–134 mmol/L", "Usually asymptomatic; subtle cognitive/gait defects"],
["Moderate", "125–129 mmol/L", "Headache, nausea, lethargy, ataxia"],
["Severe", "< 125 mmol/L", "Seizures, coma, brain herniation, death"],
]
story.append(make_table(sev_data, [4*cm, 4.5*cm, 8.5*cm], hdr_bg=C_TEAL))
story.append(sp(8))
# Pathophysiology
story.append(SubHeader("Pathophysiology — Why Does Hyponatremia Develop?", C_BLUE))
story.append(sp(4))
patho_box = [
Paragraph("<b>Core mechanism:</b> Impaired urinary dilution → water retention → dilution of serum Na⁺", S['body']),
Paragraph("Three mechanisms (Comprehensive Nephrology 7e, Ch.9):", S['bold']),
Paragraph("1. <b>Nonosmotic AVP release</b> — volume depletion, pain, nausea, drugs → V2 receptor activation → AQP-2 insertion → water retention (most common)", S['body']),
Paragraph("2. <b>Reduced distal delivery</b> — low GFR or increased proximal tubule reabsorption limits diluting segment flow", S['body']),
Paragraph("3. <b>Impaired NaCl transport</b> — thick ascending limb (TAL) / distal convoluted tubule dysfunction (e.g., thiazides)", S['body']),
]
story.append(ColorBox(patho_box, C_LIGHT_BLUE, C_BLUE))
story.append(sp(6))
# Brain adaptation table
story.append(SubHeader("Brain Adaptation: Acute vs Chronic", C_PURPLE))
story.append(sp(4))
brain_data = [
["Phase", "Timing", "Mechanism", "Clinical Implication"],
["Acute", "Minutes–Hours", "ECF→ICF water shift; Na⁺/K⁺/Cl⁻ exit from brain cells", "Cerebral edema → herniation risk"],
["Chronic", "Hours–48h", "Organic osmolyte extrusion (creatine, betaine, myoinositol, taurine, glutamate)", "Brain re-adapts; volume near normal"],
["Correction risk", "> 48h duration", "Brain depleted of osmolytes; cannot rapidly reaccumulate", "Rapid correction → osmotic demyelination (ODS)"],
]
story.append(make_table(brain_data, [2.5*cm, 3*cm, 6*cm, 5.5*cm], hdr_bg=C_PURPLE))
story.append(sp(6))
quote_box = [
Paragraph(
'"Hyponatremia is almost always the result of an increase in circulating AVP '
'and/or increased renal sensitivity to AVP, combined with an intake of free water."',
S['quote']),
Paragraph("— Harrison's Principles of Internal Medicine, 22nd Edition (2025), Ch.56", S['body_sm']),
]
story.append(ColorBox(quote_box, C_TEAL_LIGHT, C_TEAL))
story.append(sp(8))
# ── SECTION 2: CLASSIFICATION & CAUSES ───────────────────────────────────────
def section_causes(story, S):
story.append(SectionHeader("2. CLASSIFICATION & CAUSES", C_NAVY, icon="🗂"))
story.append(sp(6))
# The 3-group overview
overview_data = [
["HYPOVOLEMIC", "EUVOLEMIC", "HYPERVOLEMIC"],
["Total body water ↓\nTotal body Na⁺ ↓↓",
"Total body water ↑\nTotal body Na⁺ → (normal)",
"Total body water ↑↑\nTotal body Na⁺ ↑"],
["Urine Na⁺ <20 → extrarenal\nUrine Na⁺ >20 → renal",
"Urine Na⁺ >20 (usually)",
"Urine Na⁺ <10 (CHF/cirrhosis)\nUrine Na⁺ >20 (AKI/CKD)"],
]
t_ov = Table(overview_data, colWidths=[5.67*cm]*3)
t_ov.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), C_ORANGE),
('BACKGROUND', (1,0), (1,0), C_TEAL),
('BACKGROUND', (2,0), (2,0), C_BLUE),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8.5),
('ALIGN', (0,0), (-1,-1), 'CENTER'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('GRID', (0,0), (-1,-1), 0.5, C_WHITE),
('ROWBACKGROUNDS', (0,1), (-1,-1), [C_ORANGE_LT, HexColor("#F0FDF4")]),
('TOPPADDING', (0,0), (-1,-1), 7),
('BOTTOMPADDING', (0,0), (-1,-1), 7),
]))
story.append(t_ov)
story.append(sp(8))
# ── 2A Hypovolemic ──
story.append(SubHeader("A. Hypovolemic Hyponatremia", C_ORANGE))
story.append(sp(4))
hypo_data = [
["Urine Na⁺ < 20 mmol/L (Extrarenal Losses)", "Urine Na⁺ > 20 mmol/L (Renal Losses)"],
[
"• Vomiting / diarrhea / tube drainage\n• Burns\n• Excessive sweating\n"
"• Third-space: peritonitis, pancreatitis, ileus\n"
"⚠ Exception: vomiting + metabolic alkalosis → urine Na⁺ may be >20\n → use urine Cl⁻ (<10 = extrarenal)",
"• Thiazide diuretics (most common)\n• Primary adrenal insufficiency (Addison's)\n"
"• Salt-losing nephropathy (reflux, interstitial, medullary cystic)\n"
"• Renal tubular acidosis / metabolic alkalosis (bicarbonaturia)\n"
"• Ketonuria (alcoholic / starvation)\n• Osmotic diuresis\n"
"• Cerebral salt wasting (SAH, TBI, meningitis)"
],
]
t_hypo = Table(hypo_data, colWidths=[8.5*cm, 8.5*cm])
t_hypo.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), C_ORANGE),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8),
('GRID', (0,0), (-1,-1), 0.4, C_GREY_MED),
('BACKGROUND', (0,1), (0,1), C_ORANGE_LT),
('BACKGROUND', (1,1), (1,1), HexColor("#FFF7F0")),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 6),
('ALIGN', (0,0), (-1,0), 'CENTER'),
]))
story.append(t_hypo)
story.append(sp(8))
# Addison's callout
add_items = [
Paragraph("<b>⚠ Addison's Disease Clue:</b> Hyponatremia + Hyperkalemia + Hypotension + High Urine Na⁺", S['warn']),
Paragraph("→ Suggest primary adrenal insufficiency; confirm with AM cortisol / ACTH stimulation test", S['body']),
]
story.append(ColorBox(add_items, C_RED_LIGHT, C_RED))
story.append(sp(8))
# ── 2B Euvolemic ──
story.append(SubHeader("B. Euvolemic Hyponatremia", C_TEAL))
story.append(sp(4))
# SIAD criteria box
siad_items = [
Paragraph("<b>SIAD Diagnostic Criteria (Harrison's 22e, Table 56-1):</b>", S['teal_bold']),
Paragraph("1. Plasma osmolality < 275 mOsm/kg", S['body']),
Paragraph("2. Urine osmolality > 100 mOsm/kg (usually >300 mOsm/kg)", S['body']),
Paragraph("3. Clinical euvolemia (no dehydration, no edema/ascites)", S['body']),
Paragraph("4. Urine Na⁺ > 20–30 mmol/L on normal salt/water intake", S['body']),
Paragraph("5. Normal thyroid (TSH) and adrenal (cortisol) function", S['body']),
Paragraph("6. No recent diuretic therapy", S['body']),
]
story.append(ColorBox(siad_items, C_TEAL_LIGHT, C_TEAL))
story.append(sp(6))
# SIAD causes table
siad_cause_data = [
["Category", "Examples"],
["CNS", "Stroke, SAH, meningitis, encephalitis, Guillain-Barré, TBI, psychosis"],
["Pulmonary", "Pneumonia, TB, lung abscess, COPD exacerbation, PPV, empyema"],
["Malignancy", "Small cell lung Ca, carcinoid, lymphoma, mesothelioma, GI/GU tumors (ectopic AVP)"],
["Drugs", "SSRIs, TCAs, carbamazepine, oxcarbazepine, vincristine, cyclophosphamide,\nchlorpropamide, NSAIDs, opiates, MDMA, haloperidol, thiazides"],
["Other", "Post-operative, pain, nausea, HIV/AIDS, hereditary (V2 gain-of-function)"],
["Endocrine", "Hypothyroidism, secondary glucocorticoid deficiency"],
]
story.append(make_table(siad_cause_data, [3.5*cm, 13.5*cm], hdr_bg=C_TEAL))
story.append(sp(6))
# Other euvolemic causes
eu_other = [
Paragraph("<b>Other Euvolemic Causes:</b>", S['body']),
Paragraph("• <b>Hypothyroidism</b> — moderate to severe; corrects with thyroid hormone replacement", S['body']),
Paragraph("• <b>Secondary adrenal insufficiency</b> (pituitary disease) — glucocorticoid deficiency → loss of AVP inhibition; Note: no hyperkalemia (aldosterone intact)", S['body']),
Paragraph("• <b>Beer potomania / Low solute intake</b> — massive hypotonic fluid intake + insufficient dietary solute → insufficient osmole excretion to drive free water loss", S['body']),
]
story.append(ColorBox(eu_other, C_TEAL_LIGHT, C_TEAL))
story.append(sp(8))
# ── 2C Hypervolemic ──
story.append(SubHeader("C. Hypervolemic Hyponatremia", C_BLUE))
story.append(sp(4))
hyper_data = [
["Urine Na⁺ < 10 mmol/L", "Urine Na⁺ > 20 mmol/L"],
["• Congestive heart failure (CHF)\n — cardiac dysfunction → arterial underfilling\n"
"• Hepatic cirrhosis\n — peripheral vasodilation → reduced arterial filling\n"
"• Nephrotic syndrome\n — hypoalbuminemia → third-space losses",
"• Acute kidney injury (AKI)\n• Chronic kidney disease (CKD)\n — impaired free water excretion\n\n"
"Note: Na⁺-avid state in CHF/cirrhosis may be\nmasked by diuretic therapy"],
]
t_hyper = Table(hyper_data, colWidths=[8.5*cm, 8.5*cm])
t_hyper.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), C_BLUE),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8),
('GRID', (0,0), (-1,-1), 0.4, C_GREY_MED),
('BACKGROUND', (0,1), (0,1), C_LIGHT_BLUE),
('BACKGROUND', (1,1), (1,1), HexColor("#EFF6FF")),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 6),
('ALIGN', (0,0), (-1,0), 'CENTER'),
]))
story.append(t_hyper)
story.append(sp(8))
# ── 2D Pseudo / Translocational ──
story.append(SubHeader("D. Pseudohyponatremia & Translocational Hyponatremia", C_GREY))
story.append(sp(4))
pseudo_data = [
["Type", "Serum Osmolality", "Cause", "Action"],
["Pseudohyponatremia", "Normal (275–290)", "Severe hyperlipidemia, hyperproteinemia\n(lab artifact — water displacement)", "Remeasure with direct ISE; no treatment"],
["Translocational", "HIGH (>290)", "Hyperglycemia, mannitol, sorbitol, glycine (TURP)\n(osmotic water shift from ICF)", "Correct glucose; Na⁺ corrects automatically\n(1.6–2.4 mmol/L per 100 mg/dL glucose rise)"],
]
story.append(make_table(pseudo_data, [3.5*cm, 3.5*cm, 5.5*cm, 4.5*cm], hdr_bg=C_GREY))
story.append(sp(8))
# ── SECTION 3: CLINICAL FEATURES ─────────────────────────────────────────────
def section_clinical(story, S):
story.append(SectionHeader("3. CLINICAL FEATURES", C_NAVY, icon="🩺"))
story.append(sp(6))
# Symptoms by severity
sym_data = [
["Na⁺ Level", "Symptoms"],
["> 130 mmol/L", "Usually none; subtle gait instability, mild cognitive slowing (often unrecognized)"],
["125–130 mmol/L", "Nausea, headache, yawning, lethargy, fatigue"],
["120–125 mmol/L", "Confusion, disorientation, reversible ataxia, psychosis"],
["< 120 mmol/L", "Seizures, obtundation, coma, respiratory failure, brain herniation, death"],
]
story.append(make_table(sym_data, [4*cm, 13*cm], hdr_bg=C_RED))
story.append(sp(8))
# Acute vs Chronic two-col
story.append(SubHeader("Acute (<48h) vs Chronic (>48h) — Key Differences", C_BLUE))
story.append(sp(4))
ac_data = [
["ACUTE Hyponatremia (<48h)", "CHRONIC Hyponatremia (>48h)"],
["• Brain has NOT adapted → full osmotic stress\n"
"• Cerebral edema is the main danger\n"
"• Symptoms: nausea, headache, seizures, coma\n"
"• Neurogenic pulmonary edema possible\n"
"• Women (premenopausal) at ↑ risk — estrogen\n inhibits brain osmolyte extrusion\n"
"• Aggressive correction is REQUIRED",
"• Brain has adapted via organic osmolyte loss\n"
"• Reduced acute cerebral edema risk\n"
"• Subtle symptoms: gait disorders, cognitive deficit,\n falls, fractures\n"
"• CAUTION: Rapid correction → osmotic\n demyelination syndrome (ODS)\n"
"• Correction rate must be STRICTLY limited"],
]
t_ac = Table(ac_data, colWidths=[8.5*cm, 8.5*cm])
t_ac.setStyle(TableStyle([
('BACKGROUND', (0,0), (0,0), C_RED),
('BACKGROUND', (1,0), (1,0), C_ORANGE),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8),
('GRID', (0,0), (-1,-1), 0.4, C_GREY_MED),
('BACKGROUND', (0,1), (0,1), C_RED_LIGHT),
('BACKGROUND', (1,1), (1,1), C_ORANGE_LT),
('VALIGN', (0,0), (-1,-1), 'TOP'),
('TOPPADDING', (0,0), (-1,-1), 6),
('BOTTOMPADDING', (0,0), (-1,-1), 6),
('LEFTPADDING', (0,0), (-1,-1), 6),
('ALIGN', (0,0), (-1,0), 'CENTER'),
]))
story.append(t_ac)
story.append(sp(8))
# ODS box
ods_items = [
Paragraph("<b>Osmotic Demyelination Syndrome (ODS) / Central Pontine Myelinolysis (CPM)</b>", S['red_bold']),
Paragraph("Cause: Too-rapid correction of chronic hyponatremia → osmotic myelin destruction", S['body']),
Paragraph("Symptoms: Dysarthria, dysphagia, spastic quadriparesis, pseudobulbar palsy, 'locked-in' syndrome, coma", S['body']),
Paragraph("MRI: T2 hyperintensity in pons (±extrapontine — basal ganglia, thalamus, cerebellum)", S['body']),
Paragraph("<b>High-risk patients:</b> Na⁺ <105 | Alcoholism | Malnutrition | Liver disease | Burns | Hypokalemia", S['warn']),
Paragraph("Note: Not uniformly fatal — significant neurological recovery possible with supportive care", S['body']),
]
story.append(ColorBox(ods_items, C_RED_LIGHT, C_RED))
story.append(sp(8))
# Acute hyponatremia causes table
story.append(SubHeader("Causes of Acute Hyponatremia (Harrison's Table 56-2)", C_ORANGE))
story.append(sp(4))
acute_data = [
["Cause"],
["Postoperative hypotonic fluids — especially premenopausal women"],
["Hypotonic IV fluids with any cause of elevated AVP"],
["Glycine irrigation solutions — TURP, uterine surgery"],
["Colonoscopy preparation solutions"],
["Thiazide diuretics — recent initiation"],
["Primary polydipsia"],
["MDMA ('Ecstasy', 'Molly') — potent AVP release + thirst stimulation"],
["Exercise-associated hyponatremia — endurance events (marathons)"],
["Multifactorial, e.g., thiazide + polydipsia"],
]
story.append(make_table(acute_data, [17*cm], hdr_bg=C_ORANGE))
story.append(sp(8))
# ── SECTION 4: DIAGNOSTIC APPROACH ───────────────────────────────────────────
def section_diagnosis(story, S):
story.append(SectionHeader("4. DIAGNOSTIC APPROACH", C_NAVY, icon="🔍"))
story.append(sp(6))
diag_flow = [
Paragraph("<b>Step 1 — Confirm true hyponatremia: Measure Serum Osmolality</b>", S['bold']),
Paragraph("• Low (<275 mOsm/kg) → TRUE hypotonic hyponatremia → proceed to Step 2", S['body']),
Paragraph("• Normal (275–290) → Pseudohyponatremia (lipemia / paraproteinemia) → confirm with direct ISE", S['body']),
Paragraph("• High (>290) → Translocational (hyperglycemia, mannitol, sorbitol, glycine)", S['body']),
]
story.append(ColorBox(diag_flow, C_LIGHT_BLUE, C_BLUE))
story.append(sp(6))
diag_step2 = [
Paragraph("<b>Step 2 — Assess Volume Status (Clinical Examination)</b>", S['bold']),
Paragraph("• <b>Hypovolemic:</b> Dry mucous membranes, ↓ skin turgor, tachycardia, orthostasis, flat neck veins, recent fluid loss", S['body']),
Paragraph("• <b>Euvolemic:</b> No edema, no signs of dehydration, no ascites", S['body']),
Paragraph("• <b>Hypervolemic:</b> Pitting edema, ascites, ↑ JVP, S3 gallop, pulmonary crackles", S['body']),
]
story.append(ColorBox(diag_step2, C_TEAL_LIGHT, C_TEAL))
story.append(sp(6))
diag_step3 = [
Paragraph("<b>Step 3 — Urine Studies</b>", S['bold']),
Paragraph("• <b>Urine osmolality:</b> >100 mOsm/kg → AVP-mediated water retention | <100 mOsm/kg → primary polydipsia or low solute intake", S['body']),
Paragraph("• <b>Urine Na⁺:</b> <10–20 → extrarenal loss or Na⁺-avid state (CHF, cirrhosis, nephrotic) | >20–40 → renal loss, SIAD, hypothyroid, adrenal insuff, AKI", S['body']),
Paragraph("• <b>Urine Cl⁻:</b> Use instead of Na⁺ if vomiting with metabolic alkalosis (bicarbonaturia falsely elevates urine Na⁺)", S['body']),
]
story.append(ColorBox(diag_step3, C_ORANGE_LT, C_ORANGE))
story.append(sp(6))
# Additional tests
story.append(SubHeader("Step 4 — Additional Investigations (to find underlying cause)", C_PURPLE))
story.append(sp(4))
inv_data = [
["Test", "Purpose"],
["Serum glucose, BUN, creatinine", "Exclude translocational; assess renal function"],
["Serum lipids, serum protein (SPEP)", "Exclude pseudohyponatremia"],
["TSH, free T4", "Exclude hypothyroidism"],
["AM cortisol / ACTH stimulation test", "Exclude primary or secondary adrenal insufficiency"],
["Serum potassium", "Hyperkalemia → Addison's; Hypokalemia → ODS risk factor"],
["Serum uric acid", "Low (<4 mg/dL) → SIAD; Normal/high → CSW or hypovolemia"],
["LFTs, albumin, proBNP/BNP", "Assess cirrhosis, cardiac failure"],
["Fractional excretion of urate (FEUA)", ">12% → SIAD; helps distinguish from CSW (2026 evidence)"],
["CXR / CT chest-abdomen", "If SIAD — search for malignancy (SCLC), pulmonary cause"],
["Serum and urine osmolality simultaneously", "Calculate osmolar gap; verify urine diluting ability"],
]
story.append(make_table(inv_data, [6*cm, 11*cm], hdr_bg=C_PURPLE))
story.append(sp(8))
# SIAD vs CSW table
story.append(SubHeader("SIAD vs Cerebral Salt Wasting (CSW) — Critical Distinction", C_RED))
story.append(sp(4))
csw_items = [
Paragraph("<b>Why it matters:</b> SIAD → fluid restriction | CSW → aggressive NaCl + fluid repletion", S['warn']),
Paragraph("Confusing the two is potentially fatal", S['body']),
]
story.append(ColorBox(csw_items, C_RED_LIGHT, C_RED))
story.append(sp(4))
csw_data = [
["Parameter", "SIAD", "CSW"],
["ECF volume", "Normal/increased (euvolemic)", "↓ Decreased"],
["Body weight", "↑ Increased", "↓ Decreased"],
["Fluid balance", "Positive", "Negative"],
["Urine volume", "Normal or ↓", "Normal or ↑"],
["Tachycardia", "Absent", "Present"],
["Hematocrit", "Normal", "↑ Increased"],
["Albumin", "Normal", "↑ Increased"],
["Serum bicarbonate", "Normal or low", "↑ Increased"],
["BUN", "Normal or low", "↑ Increased"],
["Serum uric acid", "⬇ LOW (key feature)", "Normal or low"],
["Urinary Na⁺", "↑ High", "↑ High"],
["CVP/PCWP", "Normal or slightly ↑", "⬇ LOW (key feature)"],
["FEUA", ">12% → SIAD", "May be elevated briefly"],
]
t_csw = Table(csw_data, colWidths=[5.5*cm, 5.75*cm, 5.75*cm])
t_csw.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,0), C_RED),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,-1), 8),
('GRID', (0,0), (-1,-1), 0.4, C_GREY_MED),
('ROWBACKGROUNDS', (0,1), (-1,-1), [C_WHITE, HexColor("#FFF1F2")]),
('BACKGROUND', (1,10), (1,10), HexColor("#FEE2E2")), # uric acid SIAD
('BACKGROUND', (2,12), (2,12), HexColor("#FEE2E2")), # CVP CSW
('FONTNAME', (0,10), (2,10), 'Helvetica-Bold'),
('FONTNAME', (0,12), (2,12), 'Helvetica-Bold'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,0), (-1,-1), 4),
('BOTTOMPADDING', (0,0), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
]))
story.append(t_csw)
story.append(sp(8))
# ── SECTION 5: MANAGEMENT ─────────────────────────────────────────────────────
def section_management(story, S):
story.append(SectionHeader("5. MANAGEMENT", C_NAVY, icon="💊"))
story.append(sp(6))
# Correction rate box
rate_items = [
Paragraph("<b>CORRECTION RATE LIMITS — Must Memorize</b>", S['red_bold']),
Paragraph("• Maximum: <b>10–12 mmol/L per 24 hours</b> (conservative: 8–10 if high ODS risk)", S['body']),
Paragraph("• Maximum in first 24h: <b>10 mmol/L</b>", S['body']),
Paragraph("• Do NOT exceed: <b>18 mmol/L in 48 hours</b>", S['body']),
Paragraph("• Highest ODS-risk patients (Na⁺ <105, alcoholism, malnutrition, liver disease): <b>≤8 mmol/L/24h</b>", S['body']),
Paragraph("• 2026 meta-analysis (PMID 41652262): Overcorrection significantly worsens neurological outcomes & mortality", S['body_sm']),
]
story.append(ColorBox(rate_items, C_RED_LIGHT, C_RED))
story.append(sp(8))
# Adrogué-Madias formula
formula_items = [
Paragraph("<b>Adrogué-Madias Formula — Na⁺ Change from 1L Infusate:</b>", S['bold']),
Paragraph("ΔNa⁺ = (Infusate Na⁺ − Serum Na⁺) ÷ (Total Body Water + 1)", S['blue_bold']),
Paragraph("TBW = 0.6 × lean body weight (men) | 0.5 × lean body weight (women)", S['body']),
Paragraph("3% NaCl = 513 mmol/L Na⁺ | 0.9% NaCl = 154 mmol/L | 0.45% NaCl = 77 mmol/L | D5W = 0 mmol/L", S['body_sm']),
]
story.append(ColorBox(formula_items, C_LIGHT_BLUE, C_BLUE))
story.append(sp(8))
# ── 5A Acute Symptomatic ──
story.append(SubHeader("A. Acute Symptomatic Hyponatremia — EMERGENCY", C_RED))
story.append(sp(4))
acute_rx = [
Paragraph("<b>⚠ Medical Emergency — risk of cerebral edema >>> risk of ODS</b>", S['warn']),
Paragraph("<b>Treatment:</b>", S['bold']),
Paragraph("1. <b>3% NaCl (hypertonic saline)</b>", S['body']),
Paragraph(" • Standard: 1–2 mL/kg IV over 60 min, OR 100 mL IV bolus over 10 min (repeat up to 3×)", S['body_sm']),
Paragraph(" • Severe symptoms (seizures, coma): 4–6 mL/kg/hr", S['body_sm']),
Paragraph("2. <b>Target:</b> Raise Na⁺ by 4–6 mmol/L in first 6h (enough to reverse cerebral edema; full correction not needed)", S['body']),
Paragraph("3. Add <b>furosemide</b> (loop diuretic) to enhance free water excretion", S['body']),
Paragraph("4. Monitor serum electrolytes every <b>2 hours</b>", S['body']),
Paragraph("5. Monitor neurological and pulmonary status continuously", S['body']),
]
story.append(ColorBox(acute_rx, C_RED_LIGHT, C_RED))
story.append(sp(8))
# ── 5B Chronic Symptomatic ──
story.append(SubHeader("B. Chronic Symptomatic Hyponatremia (>48h duration)", C_ORANGE))
story.append(sp(4))
chronic_rx = [
Paragraph("<b>Correction must be cautious</b> — ODS risk when brain depleted of osmolytes", S['orange_bold']),
Paragraph("<b>Moderate symptoms (nausea, confusion — no seizures):</b>", S['bold']),
Paragraph("• 3% NaCl at low rate: 0.5–1 mL/kg/hr", S['body']),
Paragraph("• Raise Na⁺ 1–2 mmol/L per hour until symptoms improve", S['body']),
Paragraph("• STOP/slow once Na⁺ rises by 8–10 mmol/L or reaches 125–130 mmol/L (whichever first)", S['body']),
Paragraph("<b>If Overcorrection Occurs — Rescue Protocol:</b>", S['bold']),
Paragraph("1. STOP all hypertonic saline immediately", S['body']),
Paragraph("2. Give DDAVP 2–4 mcg IV (clamps further correction by restoring AVP effect)", S['body']),
Paragraph("3. Give D5W to re-lower Na⁺ back to safe level", S['body']),
Paragraph("4. Target: re-lower to 8–10 mmol/L below the overcorrected value", S['body']),
]
story.append(ColorBox(chronic_rx, C_ORANGE_LT, C_ORANGE))
story.append(sp(8))
# ── 5C-E Management by type ──
story.append(SubHeader("C–E. Management by Volume Status", C_BLUE))
story.append(sp(4))
mgmt_data = [
["TYPE", "FIRST-LINE", "ADDITIONAL OPTIONS"],
["Hypovolemic",
"0.9% NaCl (isotonic saline)\nCorrects volume → AVP falls → water diuresis\n⚠ Monitor closely — rapid overcorrection possible as AVP drops",
"Fludrocortisone/hydrocortisone if adrenal insufficiency\nStop diuretics"],
["Hypervolemic\n(CHF, cirrhosis, nephrotic)",
"Treat underlying disease\nFluid restriction (1–1.5 L/day)\nLoop diuretics (furosemide)",
"Vaptans (tolvaptan oral, conivaptan IV)\n• Block V2 receptor → aquaresis\n• Start in hospital — overcorrection risk\n⚠ Tolvaptan CONTRAINDICATED in cirrhosis (hepatotoxicity)"],
["Euvolemic — SIAD",
"Step 1: Remove/treat underlying cause\nStep 2: Fluid restriction <800–1000 mL/day\n(fails if urine Osm >500 or >2× serum Osm)",
"Salt tablets + furosemide (long-term)\nOral urea 15–60g/day (European guideline favourite; cheap)\nDemeclocycline (rarely used now; nephrotoxic)\nTolvaptan (short-term hospital use; expensive)"],
["Hypothyroid",
"Thyroid hormone replacement\nNa⁺ corrects spontaneously",
"Avoid aggressive Na⁺ correction\n(allow thyroid hormone to work first)"],
["Adrenal insufficiency",
"Primary: Hydrocortisone + Fludrocortisone + NS\nSecondary: Hydrocortisone alone",
"Na⁺ rapidly improves\nMonitor for overcorrection as AVP rapidly normalizes"],
]
story.append(make_table(mgmt_data, [3.5*cm, 6.5*cm, 7*cm], hdr_bg=C_BLUE))
story.append(sp(8))
# Vaptans box
vaptan_items = [
Paragraph("<b>Vasopressin V2 Receptor Antagonists (Vaptans):</b>", S['blue_bold']),
Paragraph("• Tolvaptan (oral) | Conivaptan (IV, only for euvolemic/hypervolemic)", S['body']),
Paragraph("• Mechanism: Block AVP at V2 receptor → selective aquaresis (free water loss without electrolyte loss)", S['body']),
Paragraph("• Indications: Hypervolemic and euvolemic hyponatremia refractory to fluid restriction", S['body']),
Paragraph("• CONTRAINDICATED: Hypovolemic hyponatremia | Anuric patients | Liver disease (tolvaptan hepatotoxicity)", S['warn']),
Paragraph("• Initiate ONLY in hospital; do not restrict fluids during vaptan therapy; risk of rapid overcorrection", S['body']),
]
story.append(ColorBox(vaptan_items, C_LIGHT_BLUE, C_BLUE))
story.append(sp(8))
# ── SECTION 6: QUICK REFERENCE SUMMARY ───────────────────────────────────────
def section_summary(story, S):
story.append(SectionHeader("6. QUICK REFERENCE SUMMARY TABLE", C_NAVY, icon="📊"))
story.append(sp(6))
sum_data = [
["Feature", "Hypovolemic", "Euvolemic", "Hypervolemic"],
["Total body water", "↓", "↑", "↑↑"],
["Total body Na⁺", "↓↓", "Normal", "↑"],
["Urine Na⁺", "<20 (extra-renal)\n>20 (renal)", ">20", "<10 (CHF/cirrhosis)\n>20 (AKI/CKD)"],
["Urine osmolality", "High", "High", "Variable"],
["Typical causes", "GI losses, burns,\nthiazides, Addison's,\nsalt-losing nephropathy",
"SIAD, hypothyroid,\nsecondary adrenal insuff,\nbeer potomania",
"CHF, cirrhosis,\nnephrotic syndrome,\nAKI/CKD"],
["Treatment", "0.9% NaCl + correct cause", "Fluid restriction;\ntolvaptan/urea if refractory",
"Fluid restriction;\nloop diuretics;\nvaptans; treat cause"],
["Key investigations", "Urine Na/Cl; cortisol;\nserum K; ACTH test",
"TSH; cortisol; urine Osm;\nCXR/CT chest (SIAD search)",
"Echo; LFTs; albumin;\nproBNP; creatinine"],
]
story.append(make_table(sum_data, [3.3*cm, 4.6*cm, 4.6*cm, 4.5*cm], hdr_bg=C_NAVY))
story.append(sp(8))
# Key facts box
kf_items = [
Paragraph("<b>KEY FACTS — High-Yield Points:</b>", S['bold']),
Paragraph("• Hyponatremia is the most common electrolyte abnormality — up to 22% hospitalized patients (Harrison's 22e)", S['body']),
Paragraph("• Classify ALWAYS by volume status first — this determines cause AND treatment", S['body']),
Paragraph("• First step in workup: measure serum osmolality (exclude pseudo/translocational)", S['body']),
Paragraph("• Urine Na⁺ <20 → extrarenal or Na⁺-avid state | >20 → renal/SIAD/adrenal", S['body']),
Paragraph("• Urine Cl⁻ (NOT Na⁺) in vomiting with alkalosis — more reliable", S['body']),
Paragraph("• SIAD: urine Osm > plasma Osm + euvolemia + urine Na⁺ >20 + exclude hypothyroid/adrenal insuff", S['body']),
Paragraph("• Serum uric acid: LOW in SIAD, normal/high in CSW — useful differentiator", S['body']),
Paragraph("• Correction limit: max 10 mmol/L/24h | ODS risk group: max 8 mmol/L/24h", S['body']),
Paragraph("• Acute (<48h) symptomatic: 3% NaCl bolus immediately — cerebral edema risk dominates", S['body']),
Paragraph("• Overcorrection rescue: DDAVP + D5W to re-lower Na⁺", S['body']),
Paragraph("• Beer potomania: low solute → insufficient osmoles for free water excretion; treat with dietary solute", S['body']),
]
story.append(ColorBox(kf_items, C_YELLOW_LT, C_YELLOW))
story.append(sp(8))
# Sources
story.append(SubHeader("References & Sources", C_GREY))
story.append(sp(4))
ref_data = [
["Source", "Coverage"],
["Harrison's Principles of Internal Medicine, 22nd Ed. (2025)\nCh. 56 — Sodium & Water Disorders", "Definition, pathophysiology, SIAD criteria, AVP patterns, acute hyponatremia causes, clinical features, ODS, correction approach"],
["Comprehensive Clinical Nephrology, 7th Ed.\nCh. 9 — Hyponatremia", "Etiology/classification, diluting mechanism, cerebral adaptation, treatment algorithm, acute/chronic management, vaptans, urea"],
["Bradley & Daroff's Neurology in Clinical Practice\nCh. 53 — Fluid & Electrolytes", "SIAD vs CSW comparison table, neurological hyponatremia in ICU"],
["Schneider AR et al. J Gen Intern Med. 2026 Jun\nPMID: 41652262", "Systematic review: sodium overcorrection in chronic hyponatremia → worse outcomes; validates strict correction limits"],
["Assadi F. Clin Endocrinol. 2026 Jan\nPMID: 41058069", "Systematic review: FEUA, urinary phosphate, BNP for distinguishing CSW from SIAD in neurological illness"],
["European Clinical Practice Guideline — Hyponatremia\nSpasovski et al., Eur J Endocrinol (2014)", "Standard thresholds for correction rate; vaptan indications; fluid restriction criteria; urea recommendations"],
]
story.append(make_table(ref_data, [6*cm, 11*cm], hdr_bg=C_GREY))
story.append(sp(8))
# ── MAIN ──────────────────────────────────────────────────────────────────────
def build():
out_path = "/home/daytona/workspace/hyponatremia-notes/Hyponatremia_Medical_Notes.pdf"
doc = SimpleDocTemplate(
out_path,
pagesize=A4,
topMargin=1.4*cm,
bottomMargin=1.2*cm,
leftMargin=1.75*cm,
rightMargin=1.75*cm,
title="Hyponatremia — Clinical Study Notes",
author="Orris AI",
subject="Medical Notes — Hyponatremia",
)
S = styles()
story = []
cover_page(story, S)
section_patho(story, S)
story.append(sp(4))
section_causes(story, S)
story.append(PageBreak())
section_clinical(story, S)
story.append(sp(4))
section_diagnosis(story, S)
story.append(PageBreak())
section_management(story, S)
story.append(sp(4))
section_summary(story, S)
doc.build(story, onFirstPage=make_header_footer, onLaterPages=make_header_footer)
print(f"PDF generated: {out_path}")
return out_path
if __name__ == "__main__":
build()
Running Command
cd /home/daytona/workspace/hyponatremia-notes && python3 build_pdf.py 2>&1
Running Command
ls -lh /home/daytona/workspace/hyponatremia-notes/Hyponatremia_Medical_Notes.pdf
Your Hyponatremia clinical study notes PDF is ready!
Hyponatremia Medical Notes
PDF Document · PDF
What's inside the PDF (6 sections, fully styled):
| Section | Content |
|---|---|
| Cover Page | Title card with source badges (Harrison's / Nephrology / UpToDate / PubMed), quick summary box |
| 1. Pathophysiology | Severity classification table, AVP mechanism, brain adaptation acute vs chronic table, quote from Harrison's |
| 2. Classification & Causes | 3-group overview (hypovolemic/euvolemic/hypervolemic), detailed cause tables, SIAD diagnostic criteria box, SIAD causes by category, Addison's callout, pseudohyponatremia table |
| 3. Clinical Features | Symptom severity table, acute vs chronic side-by-side comparison, ODS/CPM detail box, acute hyponatremia causes table (Harrison's) |
| 4. Diagnostic Approach | Step-by-step algorithm boxes (serum Osm → volume status → urine studies → investigations), SIAD vs CSW comparison table with highlighted key differentiators |
| 5. Management | Correction rate limits box (with 2026 meta-analysis note), Adrogué-Madias formula, acute emergency protocol, chronic symptomatic + overcorrection rescue, management-by-type table, vaptan guidelines |
| 6. Summary + References | Quick reference master table, 11 high-yield key facts, full reference list |
Styling: Color-coded section bars (navy), sub-headers (teal/blue/orange/red by topic), colored callout boxes with left accent bars, alternating-row tables, running header/footer with page numbers.
This is a shared conversation. Sign in to Orris to start your own chat.