Breast nodules and carcinoma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"breast carcinoma" AND "diagnosis"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full, detailed response.
Breast Nodules and Carcinoma
A complete guide covering benign breast nodules, carcinoma in situ, invasive breast carcinoma - including pathology, classification, risk factors, staging, and management.
Part 1: Benign Breast Nodules
Fibroadenoma
Fibroadenoma is the most common benign stromal tumor of the female breast. It arises from the intralobular stroma and is a biphasic tumor (both stromal and epithelial components).
Molecular basis: Two-thirds harbor driver mutations in MED12 (a subunit of the mediator complex regulating RNA polymerase II-dependent transcription). About one-third also carry mutations in RARA (retinoic acid receptor alpha, an estrogen target gene). These same mutations appear in uterine leiomyomas, another estrogen-responsive organ.
Morphology:
- Size ranges from <1 cm to tumors replacing most of the breast
- Mammographic density in younger women; clustered calcifications in older women
- Gross: well-circumscribed, rubbery, gray-white nodule that bulges above surrounding tissue
- Histology: delicate myxoid stroma resembling normal intralobular stroma, with:
- Pericanalicular pattern - stroma surrounds patent ducts
- Intracanalicular pattern - stroma compresses ducts into cleft-like spaces
- In older women: densely hyalinized stroma, atrophic epithelium
Clinical features:
-
Peak age: 20s and 30s
-
Frequently multiple and bilateral
-
Hormonally responsive - grow during pregnancy (can infarct, mimicking carcinoma), regress post-menopause
-
A notable association: ~50% of females on cyclosporin A after renal transplantation develop multiple bilateral fibroadenomas
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 984
Phyllodes Tumor
Phyllodes tumor arises from intralobular stroma and accounts for ~2.5% of fibroepithelial lesions.
Molecular basis: Shares MED12 and RARA mutations with fibroadenoma, but additionally carries mutations in TERT (telomerase), TP53, and RB - explaining its more aggressive potential.
Morphology:
- Varies from a few cm to massive lesions replacing the entire breast
- Larger lesions have bulbous, leaf-like protrusions (phyllodes = Greek for "leaf-like")
- Graded as benign, borderline, or malignant based on stromal atypia, cellularity, and mitotic activity
- Malignant phyllodes tumors can resemble sarcoma when there is marked stromal overgrowth
Clinical features:
-
Peak age: sixth decade (10-20 years later than fibroadenoma)
-
Up to 75% are benign - may recur locally but do not metastasize
-
Borderline and malignant tumors have higher recurrence rates; margin status is the most important predictor
-
Lymphatic spread is rare; axillary lymph node dissection is contraindicated
-
Malignant lesions: ~1/3 develop hematogenous distant metastases (only stromal component metastasizes)
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 984
Other Benign Stromal Lesions
| Lesion | Key Feature |
|---|---|
| Myofibroblastoma | Only breast tumor equally common in males |
| Lipoma | Fat-containing lesion; palpable and mammographically visible |
| Fibromatosis | Clonal fibroblast/myofibroblast proliferation; locally aggressive, no metastasis; associated with FAP, Gardner syndrome |
Part 2: Breast Carcinoma - Epidemiology and Risk Factors
Breast cancer is the most common malignancy globally and the leading cause of cancer death in females worldwide. In 2020, it surpassed lung cancer as the most common cancer overall with an estimated 2.3 million new cases - nearly 12% of all new cancer diagnoses. In the United States, the lifetime risk is 1 in 8 for females living to age 90.
Risk Factors
Modifiable:
| Factor | Relative Risk |
|---|---|
| Obesity (BMI >30) | RR 1.29 (postmenopausal) |
| Nulliparity / first pregnancy >35 years | Increased |
| HRT use >10 years | RR 1.2 |
| Smoking ≥25 cigarettes/day | RR 1.14 |
| Alcohol (heavy, >4 drinks/day) | RR 1.46 |
| Radiation exposure | RR 6 |
| No/short breastfeeding | Protective if >12 months |
Non-modifiable:
-
Increasing age (75% of cancers diagnosed after age 50)
-
Hormonal factors: early menarche, late menopause (prolonged estrogen exposure)
-
Genetic mutations: ~12% of all breast cancers are caused by germline mutations
- BRCA1 (17q21): 50-85% lifetime risk of breast cancer + up to 40% risk of ovarian cancer; cancers are mostly TNBC
- BRCA2 (13q12.3): up to 50-60% lifetime breast cancer risk + 20% ovarian cancer risk; also associated with prostate, colon, pancreatic cancers
- Other high-penetrance genes: PALB2, TP53, Li-Fraumeni syndrome, Cowden syndrome, Peutz-Jeghers syndrome
-
Bailey and Love's Short Practice of Surgery 28th Edition, p. 952
Part 3: Carcinoma in Situ
Ductal Carcinoma In Situ (DCIS)
- A precursor to invasive ductal carcinoma
- Most often found on mammographic screening as microcalcifications
- If untreated and carcinoma develops, it is usually an invasive ductal carcinoma in the same breast
Lobular Carcinoma In Situ (LCIS)
-
A marker of increased risk AND a precursor lesion
-
When carcinoma later develops: two-thirds in the same breast, one-third in the contralateral breast
-
Histology: small, rounded, loosely cohesive cells filling and expanding lobular acini
-
Immunohistochemistry: E-cadherin negative (distinguishes from ductal carcinoma)
-
Pleomorphic LCIS variant: large pleomorphic cells with abundant cytoplasm mixed with small rounded cells
-
Robbins & Kumar Basic Pathology, p. 719
Part 4: Invasive Breast Carcinoma - Classification
Histological Classification (Foote & Stewart)
| Type | Frequency |
|---|---|
| Invasive ductal carcinoma - No Special Type (NST) | ~80% |
| Invasive lobular carcinoma | ~10% |
| Medullary carcinoma | ~4% |
| Mucinous (colloid) carcinoma | ~2% |
| Papillary carcinoma | ~2% |
| Tubular carcinoma | ~2% |
| Rare (adenoid cystic, squamous cell, apocrine) | <1% |
| Paget's disease of the nipple | Special type |
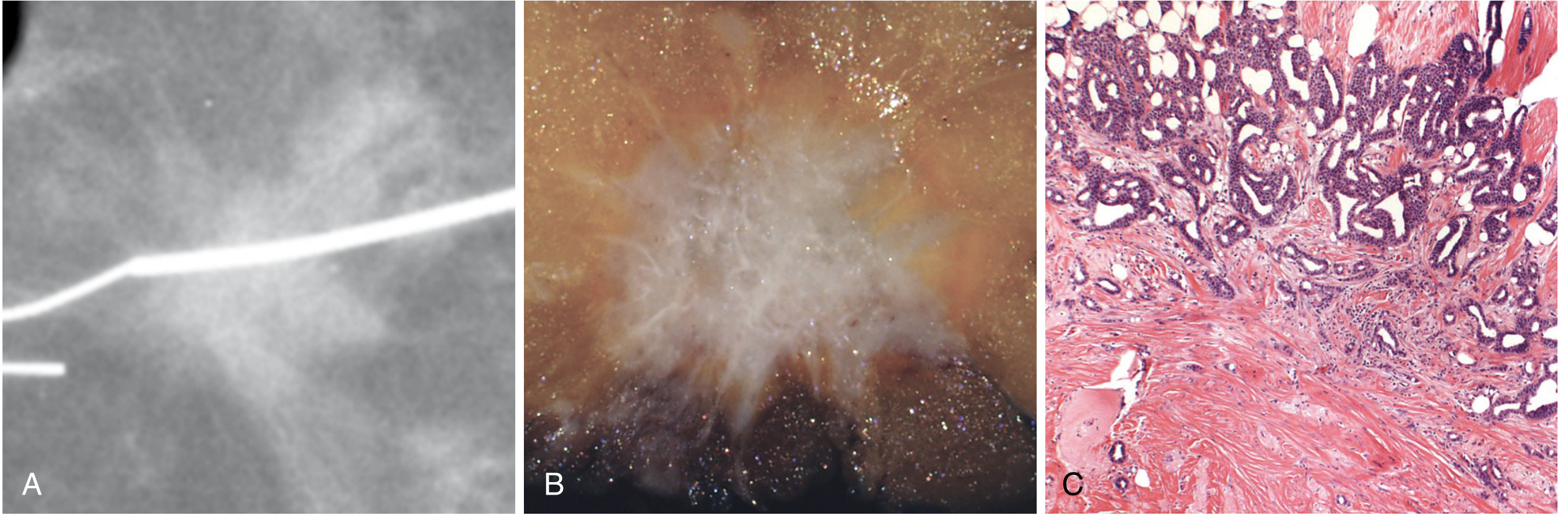
Invasive carcinoma of no special type (NST): Most common. Presents as a hard, irregular, radiodense mass with a characteristic desmoplastic stromal reaction. When cut, produces a grating sound due to chalky-white stroma and calcifications.
Paget's disease of the nipple:
- Presents as a chronic, eczematous eruption of the nipple that may progress to an ulcerated, weeping lesion
- Usually associated with extensive DCIS; may have an underlying invasive cancer
- Pathognomonic: Paget cells - large, pale, vacuolated cells in the rete pegs
- Differentiation from melanoma: Paget's disease is CEA-positive; melanoma is S-100 positive
Histologic Grading (Nottingham Score)
Based on three features: (1) tubule/gland formation, (2) nuclear pleomorphism, (3) mitotic rate.
| Grade | Features |
|---|---|
| Grade 1 (well differentiated) | Tubular/cribriform pattern, small uniform nuclei, low proliferation |
| Grade 2 (moderately differentiated) | Mixed solid and glandular; intermediate nuclear pleomorphism |
| Grade 3 (poorly differentiated) | Ragged nests or solid sheets; enlarged irregular nuclei; high mitotic rate; necrosis |
Part 5: Molecular Classification
Breast cancers are divided into three major clinical groups based on biomarker expression:
| Group | Markers | Features |
|---|---|---|
| Luminal (ER+/HER2-) | ER-positive | Most common; divided into Luminal A (low proliferation) and Luminal B (high proliferation); late recurrences continue beyond 10 years |
| HER2+ | HER2 overexpression (gene amplification) | Responds well to HER2-targeted inhibitors; bimodal recurrence pattern |
| Triple Negative (TNBC) | ER-/PR-/HER2- | Often linked to BRCA1 defects, TP53 mutation; poorest prognosis; almost all recurrences within first 8 years |
Additionally, gene expression profiling identifies 6 intrinsic molecular subtypes: Luminal A, Luminal B, HER2-enriched, Basal-like, Normal-like, and Claudin-low.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
Part 6: Staging (AJCC 8th Edition)
The AJCC 8th edition combines anatomic stage with molecular group to create prognostic stage groups that better estimate survival than anatomic stage alone.
Anatomic staging (simplified TNM):
- T - Tumor size (T1: ≤2 cm, T2: 2-5 cm, T3: >5 cm, T4: skin/chest wall involvement)
- N - Nodal status (N0: no nodes, N1-N3: increasing nodal involvement)
- M - Distant metastasis
Part 7: Management
Surgery
| Stage | Options |
|---|---|
| Early (I, II) | Breast-conserving surgery (BCS/lumpectomy) + sentinel lymph node biopsy (SLNB) OR modified radical mastectomy (MRM) |
| Locally advanced (IIIA, IIIB) | Neoadjuvant chemotherapy (NACT) first, then BCS or mastectomy; inflammatory carcinoma requires MRM |
| Reconstruction | Implant-based or autologous (TRAM/DIEP flap, latissimus dorsi flap) |
Sentinel lymph node biopsy (SLNB): Standard for axillary staging in clinically node-negative disease. False-negative rate >10% after NACT can be reduced by removing ≥3 sentinel nodes with dual tracers or "targeted SLNB" (clip marking of positive nodes pre-NACT).
Adjuvant Radiotherapy
Indicated for:
- All patients after BCS (breast-only if node-negative: 40-42.5 Gy in 15-16 fractions hypofractionation, or 45-50.4 Gy in 25 fractions)
- After mastectomy if: tumor ≥5 cm, skin/chest wall involvement, lymphovascular invasion (grade 3), or lymph node-positive disease
- Locally advanced cancers (T3, T4, N1-N3): locoregional radiotherapy covering chest wall + supraclavicular region
Systemic Therapy
| Type | Target | Examples |
|---|---|---|
| Endocrine therapy | ER-positive disease | Tamoxifen, aromatase inhibitors |
| HER2-targeted therapy | HER2-positive | Trastuzumab, pertuzumab, lapatinib |
| Chemotherapy | All subtypes (especially TNBC) | Anthracyclines, taxanes |
| CDK 4/6 inhibitors | Luminal A/B metastatic | Palbociclib, ribociclib |
Metastatic Disease (Stage IV)
Treatment is palliative:
-
Hormone receptor-positive with bony/limited visceral metastasis: endocrine therapy preferred
-
Hormone receptor-negative or visceral crisis: systemic chemotherapy
-
Bone metastases: palliative radiotherapy to weight-bearing areas + bisphosphonates
-
Pleural effusions: intercostal drainage + pleurodesis
-
Solitary visceral metastasis in good performance status: surgical resection may be considered
-
Bailey and Love's Short Practice of Surgery 28th Edition
Part 8: Hereditary and Familial Breast Cancer
- Hereditary breast cancer (HBC): 5-10% of all breast cancers; identifiable genetic mutation, more aggressive, earlier onset, more often multicentric and bilateral
- Familial breast cancer (FBC): 20-30%; affects family members but no known single mutation
- High-penetrance mutations: BRCA1, BRCA2, TP53 (Li-Fraumeni), PTEN (Cowden), STK11 (Peutz-Jeghers), CDH1 (hereditary gastric cancer)
- Genetic risk evaluation is recommended for high-risk individuals (strong family history, early onset, bilateral or male breast cancer)
Summary Table: Key Breast Nodules at a Glance
| Lesion | Age Peak | Key Feature | Malignant Potential |
|---|---|---|---|
| Fibroadenoma | 20s-30s | Mobile, rubbery, MED12 mutation | Benign |
| Phyllodes tumor | 50s-60s | Leaf-like, large; graded benign/borderline/malignant | Variable |
| DCIS | Varies | Microcalcifications on mammo; precursor to IDC | Pre-malignant |
| LCIS | Varies | E-cadherin negative; bilateral risk marker | Pre-malignant |
| Invasive ductal (NST) | >50 | Hard, spiculate, desmoplastic | Malignant (most common) |
| Invasive lobular | >50 | Single file infiltration; E-cadherin loss | Malignant |
| Inflammatory carcinoma | Varies | Peau d'orange, erythema, no discrete mass | Malignant (aggressive) |
| Paget's disease | Varies | Eczematous nipple; Paget cells | Malignant |
Recent evidence note: A 2024 systematic review and meta-analysis (PMID 39270543) confirms that atypical ductal/lobular hyperplasia, LCIS, and flat epithelial atypia significantly increase future breast cancer risk, supporting their use as risk stratification markers. A 2026 systematic review (PMID 41232399) highlights advances in multimodal AI-based fusion methods for breast carcinoma diagnosis, an evolving clinical tool.
This is a shared conversation. Sign in to Orris to start your own chat.