Masquelet technique ms ortho 20 marks answer
Reading File
Finding Sources
Finding Sources
Searching PubMed
Masquelet technique induced membrane bone defect
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content from Rockwood & Green's and Campbell's. I have enough for a complete 20-mark MS Ortho answer. Let me compile the full structured answer.
Masquelet Technique (Induced Membrane Technique)
Definition and Introduction
The Masquelet technique, also called the induced membrane technique (IMT), is a two-stage biological method for reconstruction of large segmental bone defects (critical-size defects). It was first described by Alain Charles Masquelet in 2000, who reported successful use in 35 cases with defects ranging from 4 to 25 cm. The technique exploits the body's foreign body reaction to a PMMA cement spacer to generate a biologically active "induced membrane" that then facilitates bone healing in the second stage.
Indications
- Large segmental bone defects (typically >2 cm; classically 4-25 cm or more)
- Post-traumatic bone loss (high-energy fractures, open fractures with bone extrusion)
- Infected nonunion with bone defect (osteomyelitis)
- Chronic osteomyelitis with segmental bone loss
- Tumor resection defects (non-oncological reconstruction)
- Failed bone grafting procedures
- Tibial, femoral, humeral, radial/ulnar, and foot/ankle defects
Defects up to 62 mm have the best outcomes; success rates decline beyond this threshold (Frese et al., 195 patients, ~90% overall success).
Prerequisites (Requirements Before the Procedure)
- Adequate soft tissue coverage - an excellent soft tissue envelope is mandatory
- Infection control - active infection must be eradicated before or as part of Stage 1
- Stable fixation - internal or external
- Patient optimization - no uncontrolled diabetes, adequate nutrition, non-smoking ideally
- Adequate vascularity of the limb
Principle / Biological Basis
The PMMA cement spacer acts as a foreign body and triggers a foreign body reaction. Over 4-8 weeks, a pseudomembrane (the "Masquelet membrane") forms around the spacer. This membrane:
| Property | Detail |
|---|---|
| Histology | Synovial-like, vascularized, with few inflammatory cells |
| Growth factors | Produces BMP-2, TGF-beta, VEGF, FGF - maximal at ~4 weeks |
| Function 1 | Contains the graft and maintains the space |
| Function 2 | Prevents fibrous ingrowth into the defect |
| Function 3 | Osteoinductive - provides growth factors for bone regeneration |
| Function 4 | Osteoconductive scaffolding environment |
The membrane itself is capable in some cases of generating enough bone without secondary grafting (though this is the exception, not the rule).
The Two Stages
Stage 1: Cement Spacer Implantation
Timing: Acute (within days) or after debridement and infection control
Steps:
- Thorough debridement - excision of all devitalized/infected bone and soft tissue; achieve clean margins
- Fracture stabilization - IM nail (diaphyseal defects) or locking plate (metaphyseal defects); external fixator may also be used
- Fill the defect with a PMMA cement spacer - shaped to match the defect; can be antibiotic-laden (vancomycin + gentamicin achieve 200x the serum antibiotic concentration locally) for infected cases
- Wound closure over the spacer (or soft tissue coverage flap if required)
- Systemic antibiotics as per intraoperative cultures
In infected cases, antibiotic-impregnated PMMA (Palacos cement is superior in elution to Simplex cement) achieves extremely high local antibiotic concentrations compared to IV dosing.
Interval between stages: 4 to 8 weeks (minimum 4 weeks; growth factor expression peaks at ~4 weeks; some surgeons prefer 6-8 weeks for larger defects or infected cases)
Stage 2: Membrane Preservation + Bone Grafting
Timing: 4-8 weeks after Stage 1 (when the membrane has matured)
Steps:
- Reopen the wound through the SAME incision
- Carefully incise the induced membrane longitudinally (do NOT excise or damage it - the membrane must be preserved)
- Remove the PMMA spacer (the membrane stays intact like a biological "tube")
- Pack the defect tightly with bone graft - cancellous autograft (iliac crest is gold standard; RIA - Reamer-Irrigator-Aspirator from femur/tibia for large volumes)
- Close the membrane over the graft
- Maintain stable fixation
- Allow recorticalization (typically 3 to 6 months)
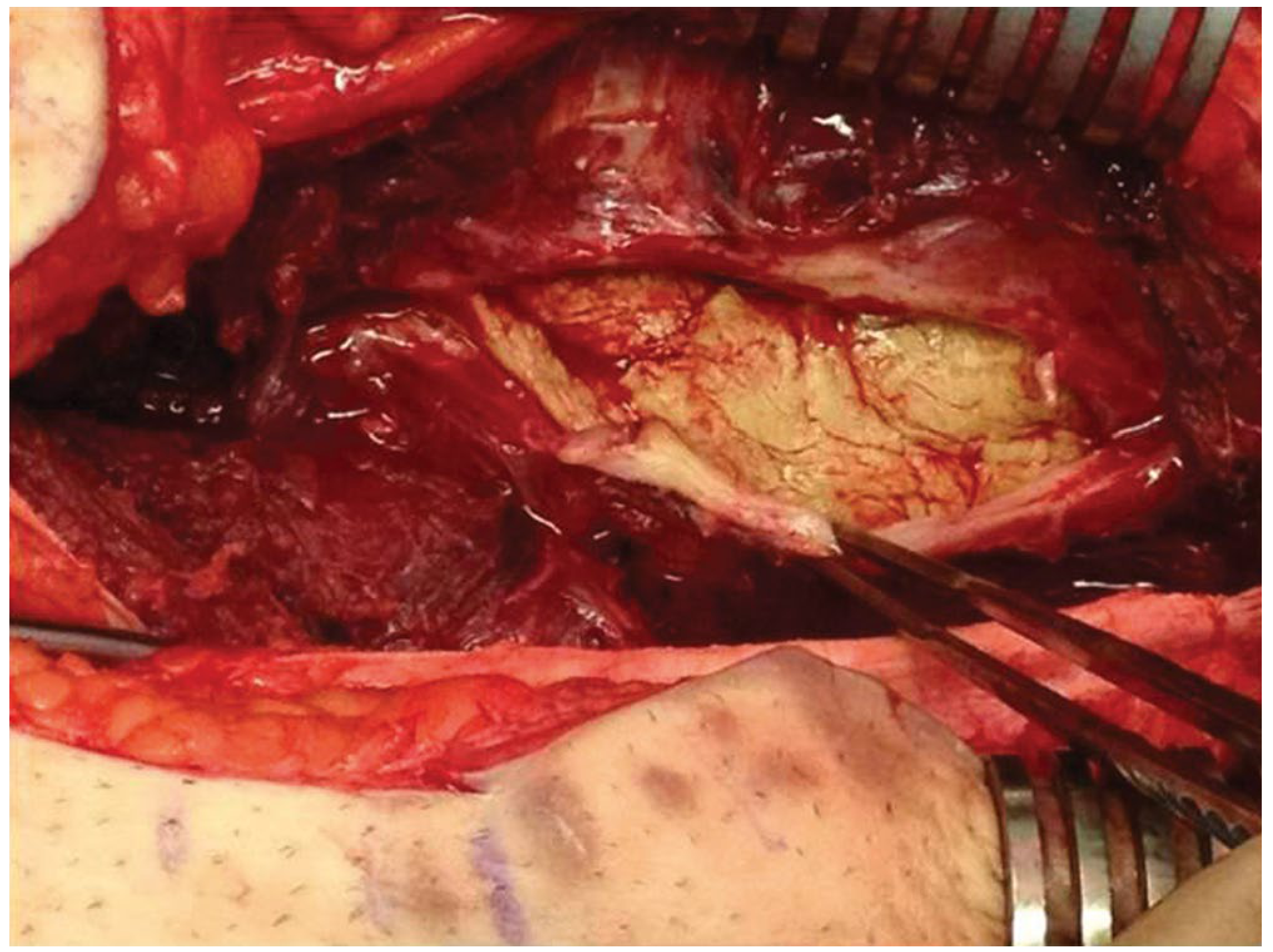
FIGURE: Intraoperative photo (Stage 2) showing the vascularized Masquelet membrane formed around the PMMA spacer - Campbell's Operative Orthopaedics 15th Ed.
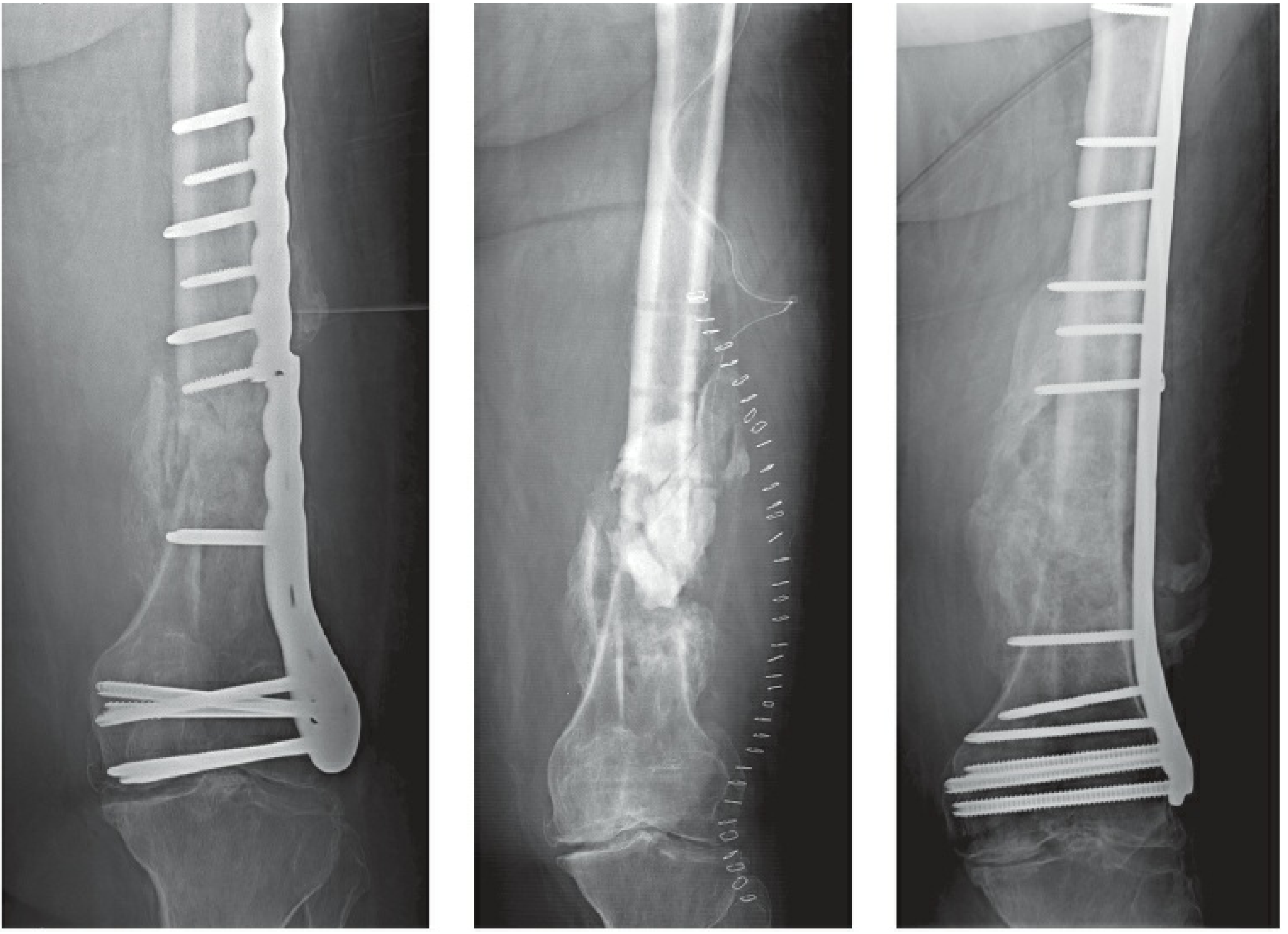
FIGURE 30-29: (A) Infected distal femur nonunion. (B) PMMA spacer in place. (C) Healed bone after Stage 2 grafting. - Rockwood & Green's Fractures in Adults, 10th Ed.
Bone Graft Options (Stage 2)
| Graft Type | Comment |
|---|---|
| Cancellous autograft (iliac crest) | Gold standard - osteogenic, osteoconductive, osteoinductive |
| RIA (Reamer-Irrigator-Aspirator) | Large volumes for big defects; lower donor site morbidity than iliac crest |
| Free non-vascularized fibular graft | Combined with cancellous graft for defects 5-14 cm (87% healing rate) |
| Beta-tricalcium phosphate (beta-TCP) | Successfully used as graft expander with cancellous graft |
| BMP-2 + cancellous graft | Adjunct to augment osteoinduction |
Fixation
- Diaphyseal defects: Locked intramedullary nail (preferred)
- Metaphyseal defects: Locked plate
- Secondary stabilization may be required and is associated with improved outcomes (~34% of cases in Frese's series needed it)
Advantages Over Alternatives
| Feature | Masquelet | Ilizarov/Bone Transport | Free Vascularized Fibula |
|---|---|---|---|
| Technical complexity | Moderate | High | Very high |
| Time | Shorter (months) | Long (1-2+ years) | Moderate |
| Equipment | Standard | Specialized frame | Microvascular setup |
| Infection | Excellent (antibiotic spacer) | Good | Moderate risk |
| Defect size | 4-25+ cm | Unlimited | Up to ~25 cm |
| Upper limb | Better tolerated | Cumbersome | Good |
Outcomes
- Masquelet's original series (2000): 35 cases, defects 4-25 cm, successful in all
- Frese et al. (2017): 195 infected defects, 175 patients - ~90% overall success; critical limit of success = 62 mm defect size
- Morris et al. (2017): 12 tibial defects - only 5/12 achieved union; 5 infective complications, 2 required amputation (highlights complexity)
- Upper limb defects: Better tolerated and more successful than lower limb
- Meta-analysis (Singh et al. 2023, PMID 37542493): Compared to vascularized bone grafting in upper extremity - comparable outcomes with Masquelet
- Systematic review (Wakefield et al. 2024, PMID 37921889): IMT vs. distraction osteogenesis for infected tibial non-unions - both viable with different complication profiles
Complications
| Complication | Note |
|---|---|
| Infection / septic complications | Most common; up to 40% in complex tibial cases |
| Graft resorption | Inadequate packing or membrane damage |
| Refracture | Before full recorticalization |
| Nonunion (Stage 2 failure) | Need for secondary procedures |
| Donor site morbidity | Iliac crest pain, hernia, nerve injury |
| Membrane damage at Stage 2 | Technical error - avoid by careful opening |
| Amputation | In most severe infected failures |
Special Situations
Infected Nonunion (most common indication):
- Stage 1 uses antibiotic-impregnated PMMA spacer (vancomycin + tobramycin or gentamicin)
- Mandatory: eradicate infection before Stage 2; systemic antibiotics per culture sensitivities
- Membrane itself acts as a barrier to reinfection
Lower vs. Upper Limb:
- Upper limb: Moderate gaps can be managed by bone shortening; IMT more successful and better tolerated
- Lower limb: More challenging due to weight-bearing demands; higher complication rates
Talus:
- Masquelet with cement spacer indicated for significant contamination, irreparable talar comminution
Comparison with Bone Transport (Ilizarov)
Both techniques are valid for segmental defects >6 cm. Masquelet requires:
- Two operations, shorter treatment time, no external frame issues
- Ilizarov requires prolonged frame wearing, pin tract infections are universal, but can manage unlimited defect sizes and simultaneously correct deformity/LLD
Key Points to Remember (Summary Box)
- Two-stage technique: Stage 1 (PMMA spacer) → wait 4-8 weeks → Stage 2 (graft)
- PMMA spacer induces a biologically active pseudo-membrane (BMP-2, TGF-beta, VEGF)
- Membrane is synovial-like, vascular, with few inflammatory cells
- Growth factors peak at ~4 weeks
- Stage 2: preserve the membrane, remove cement, pack with cancellous autograft
- Fixation: IM nail (diaphyseal) or locked plate (metaphyseal)
- Recorticalization: 3-6 months
- Works for defects 4-25+ cm; best outcomes below 62 mm
- Antibiotic spacer achieves 200x local antibiotic concentration vs. IV
- Excellent soft tissue envelope is mandatory
Sources: Rockwood & Green's Fractures in Adults, 10th Ed. 2025 (Ch. 30); Campbell's Operative Orthopaedics, 15th Ed. 2026 (Ch. 64); Masquelet et al. original series 2000; Frese et al. 2017 (195 cases); Singh et al. meta-analysis PMID 37542493; Wakefield et al. systematic review PMID 37921889
This is a shared conversation. Sign in to Orris to start your own chat.