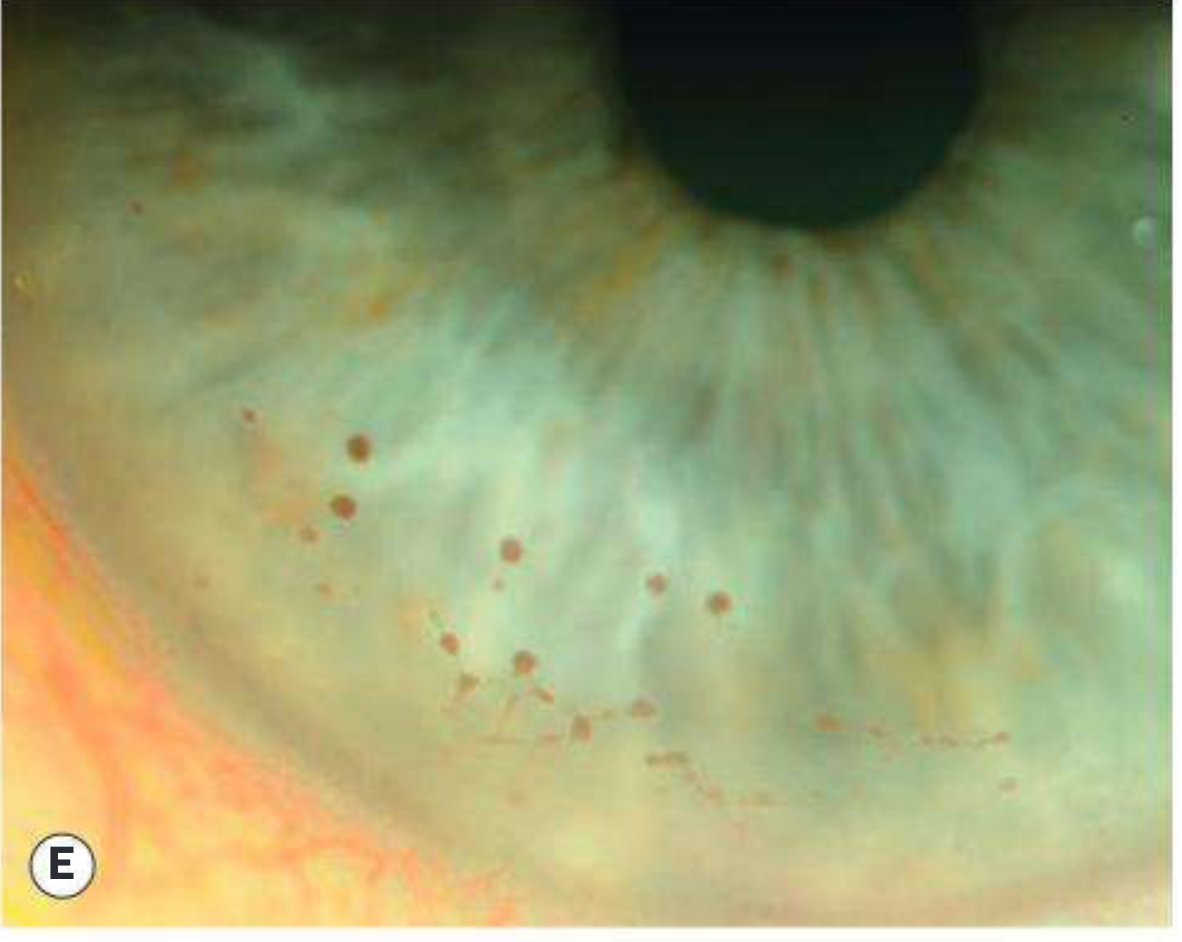
Various signs of anterior uveitis.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Excellent - I now have comprehensive content and images for a full, well-illustrated answer. Let me now compile the complete response.
Signs of Anterior Uveitis
Anterior uveitis is inflammation of the iris and anterior part of the ciliary body (pars plicata). It is the most common form of uveitis. Signs are best appreciated on slit-lamp examination and are traditionally divided into those seen in acute anterior uveitis (AAU) and, additionally, those seen in chronic anterior uveitis (CAU).
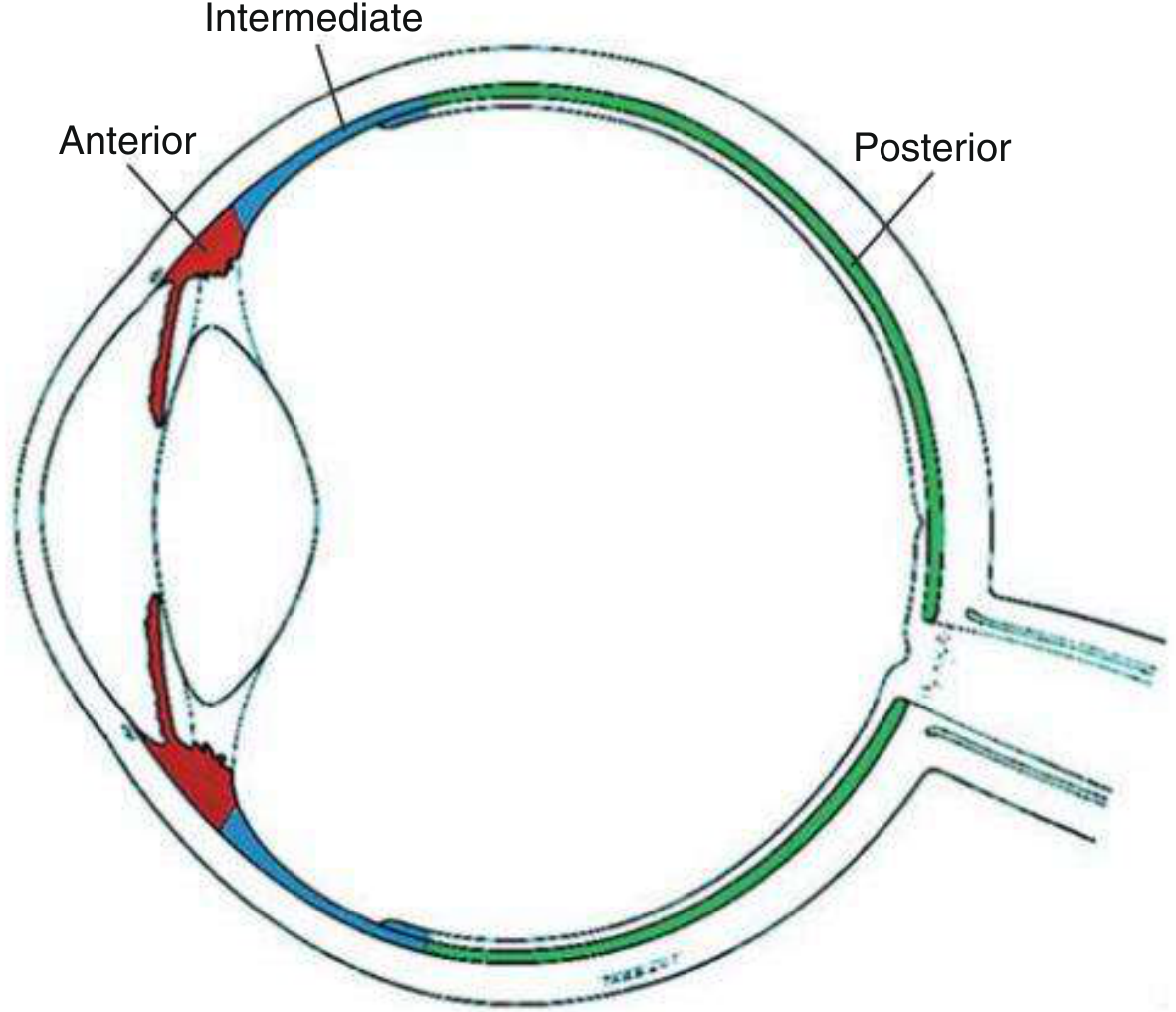
Fig. 12.1 - Anatomical classification of uveitis (anterior region highlighted in red):
1. Ciliary Injection (Perilimbal/Ciliary Flush)
Circumcorneal conjunctival hyperaemia with a violaceous (purplish) hue, due to involvement of the deeper episcleral and limbal blood vessels. It is characteristically present in AAU and may be absent in some forms of CAU. It is distinct from the bright-red superficial injection of conjunctivitis.
2. Miosis
Pupillary constriction due to sphincter spasm from inflamed iris tissue. The small pupil predisposes to posterior synechiae formation.
3. Anterior Chamber (AC) Cells
The most reliable indicator of active inflammation. Inflammatory cells (lymphocytes, plasma cells) are visible as white particles floating in the aqueous on slit-lamp examination using a narrow, bright 1 mm × 1 mm beam. The SUN Working Group grading system is used:
| Grade | Cells in 1 mm × 1 mm field |
|---|---|
| 0 | < 1 |
| 0.5+ | 1-5 |
| 1+ | 6-15 |
| 2+ | 16-25 |
| 3+ | 26-50 |
| 4+ | > 50 |
Cells may also be seen in the anterior vitreous. Swept-source anterior segment OCT can image individual inflammatory cells.
4. Aqueous Flare
Haziness of the normally optically clear anterior chamber fluid due to protein leakage from breakdown of the blood-aqueous barrier. Seen as a "Tyndall effect" - the slit beam appears as a hazy column. Graded on the SUN scheme:
| Grade | Description |
|---|---|
| 0 | None |
| 1+ | Faint |
| 2+ | Moderate (iris and lens details clear) |
| 3+ | Marked (iris and lens details hazy) |
| 4+ | Intense (fibrin or "plastic aqueous") |
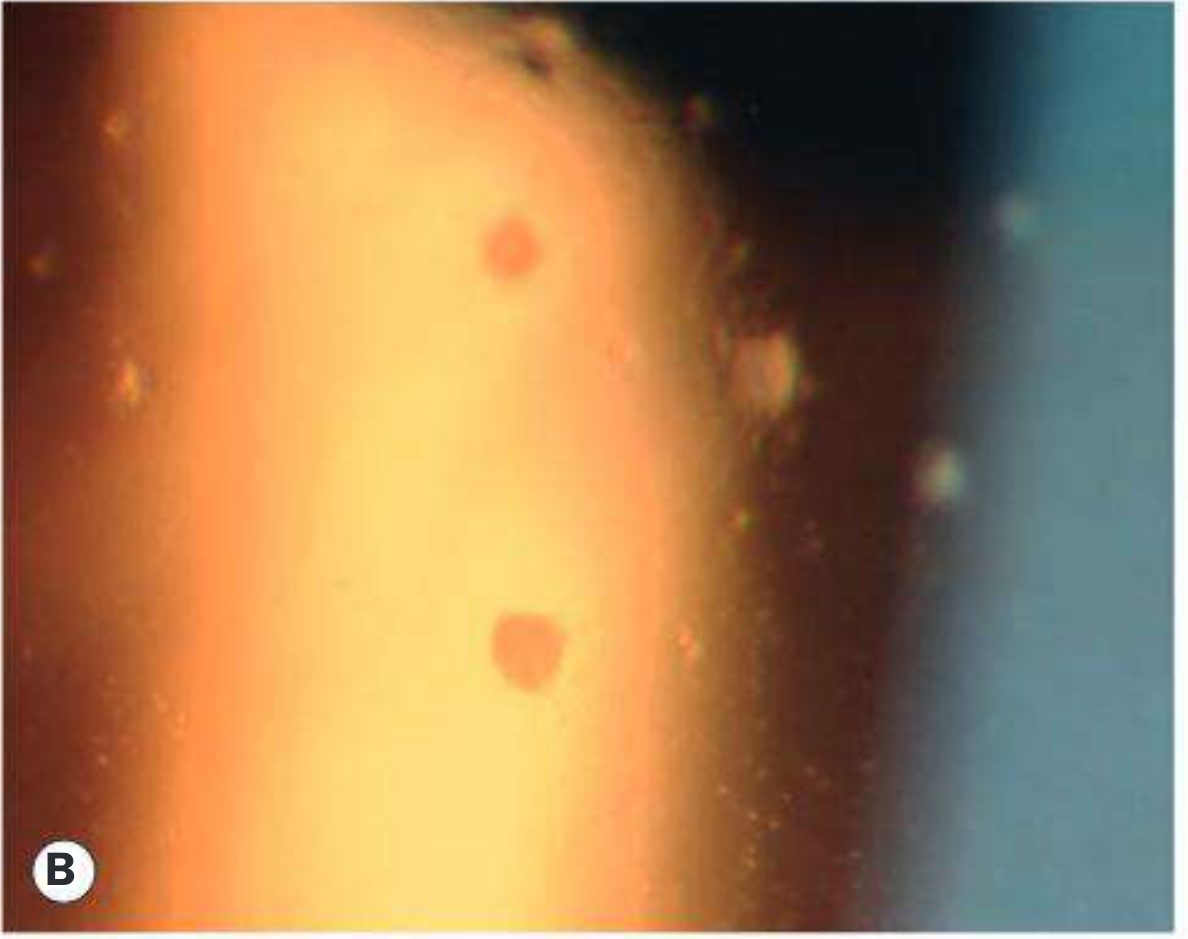
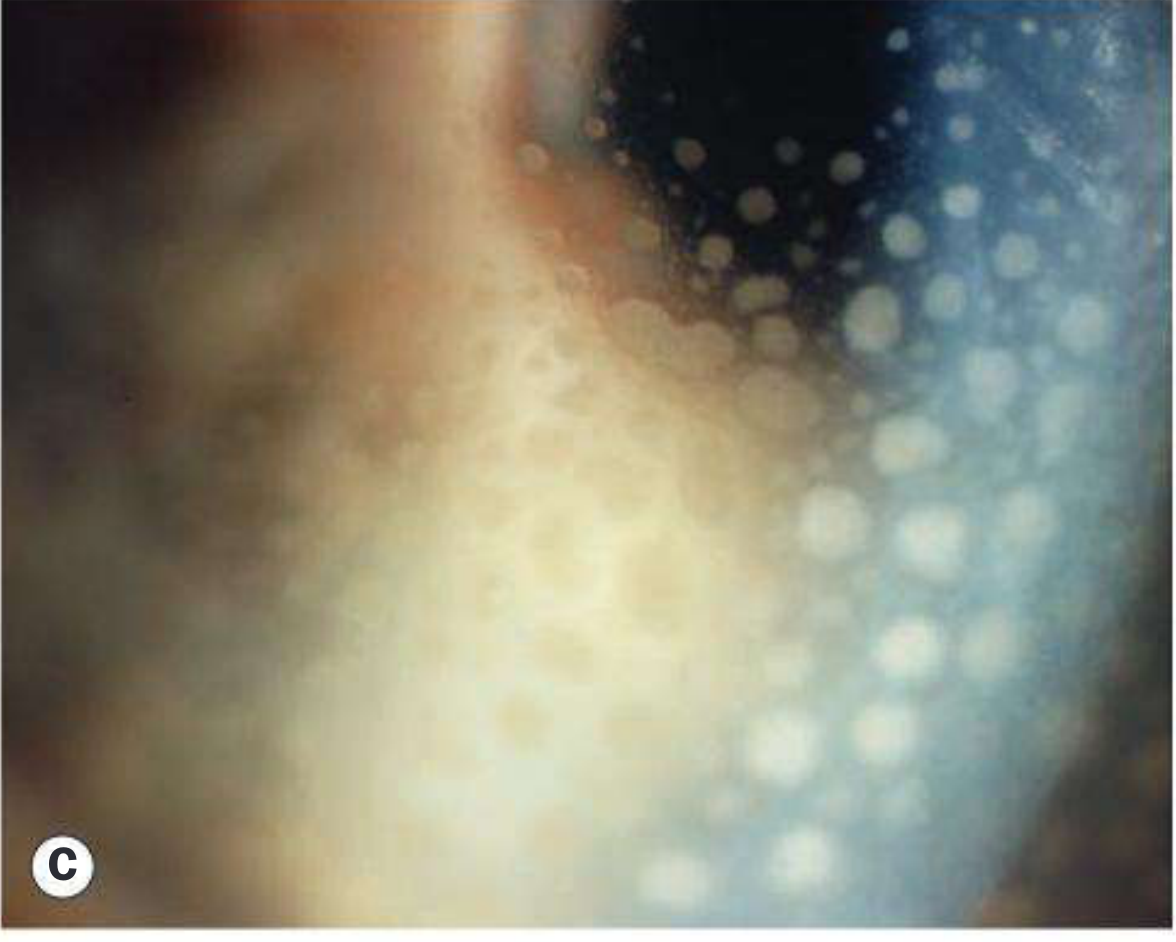
5. Keratic Precipitates (KP)
Deposits of inflammatory cells (lymphocytes, plasma cells, macrophages) on the corneal endothelium. They typically concentrate inferiorly in a triangular pattern - apex pointing upward - known as Arlt's triangle, due to gravity and aqueous convection currents.
Types by morphology:
- Fine/small KP - seen in non-granulomatous (typically acute) inflammation
- "Mutton fat" KP - large, greasy-appearing deposits of epithelioid cells; hallmark of granulomatous uveitis (e.g., sarcoidosis, TB)
- Stellate / filamentous KP - small to medium, star-shaped; characteristic of Fuchs uveitis syndrome (diffusely distributed, not in Arlt's triangle)
- Pigmented KP - old resolved KP; may take on a "ground glass" appearance in granulomatous disease
- Endothelial "dusting" - individual cells seen before true KP aggregates form

6. Hypopyon
A whitish, purulent exudate composed of inflammatory cells that settles by gravity into the inferior anterior chamber, forming a horizontal fluid level. Common in HLA-B27-associated AAU and also seen in Behcet disease. It indicates severe, often non-granulomatous inflammation.
7. Fibrinous Exudate
Fibrin strands or a fibrinous membrane in the anterior chamber, seen in severe AAU. Like hypopyon, it is especially associated with HLA-B27-related inflammation. Graded 1-4+ using the AC flare scale; grade 4+ is sometimes called "plastic aqueous."
8. Iris Nodules
Present in both granulomatous and non-granulomatous uveitis:
- Busacca nodules - located in the iris stroma; feature of granulomatous uveitis (e.g., sarcoidosis)
- Koeppe nodules - located at the pupillary margin; can occur in both granulomatous and non-granulomatous types; may be a site of posterior synechiae formation
- Roseolae - yellowish nodules from dilated iris vessels; seen in syphilitic uveitis
- Iris "pearls" - in lepromatous CAU
- Iris crystals (Russell bodies) - immunoglobulin deposits; rare; seen in Fuchs uveitis syndrome and some chronic uveitides
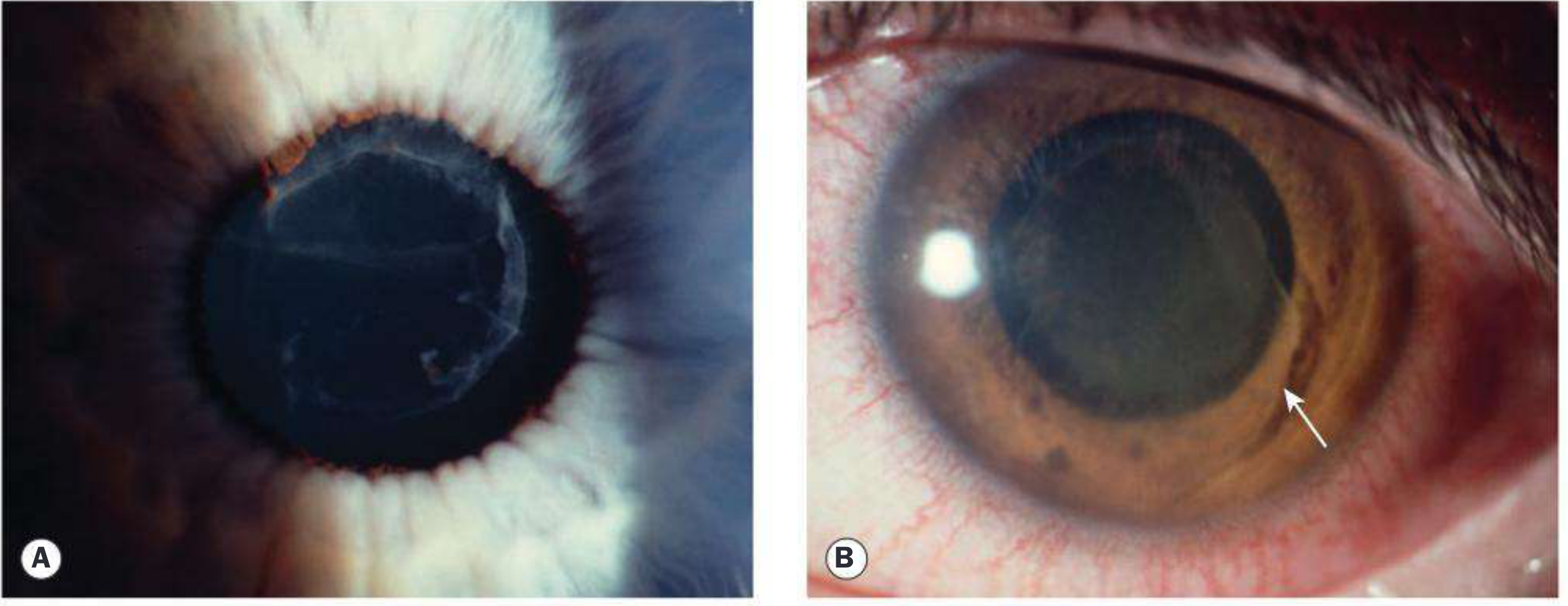
9. Posterior Synechiae (PS)
Inflammatory adhesions between the pupil margin and the anterior lens capsule. They form rapidly when miosis and fibrin are present. On attempted dilatation, the pupil assumes an irregular ("festooned") shape. When 360° of the pupil margin is adherent, seclusion pupillae results, blocking aqueous flow and causing iris bombe and secondary angle-closure glaucoma.
10. Iris Changes
- Iris atrophy: Diffuse stromal atrophy is typical of Fuchs uveitis syndrome; patchy or sectoral atrophy is characteristic of herpetic uveitis (both HSV and VZV, though VZV more commonly gives a sectoral pattern)
- Heterochromia iridis: Difference in iris colour between the two eyes; classically seen in Fuchs uveitis syndrome (the affected eye is typically lighter)
- Iris neovascularization (rubeosis iridis): Occurs in chronic inflammation; abnormal vessels are very common in Fuchs uveitis syndrome but do not cause synechial angle closure there
11. Intraocular Pressure (IOP) Changes
- Reduced IOP - common in acute inflammation due to impaired aqueous secretion by the inflamed ciliary epithelium
- Elevated IOP - can occur as inflammation subsides (trabecular obstruction by cells/debris, trabeculitis, or steroid use); particularly associated with herpetic and Posner-Schlossman syndrome; in CAU, trabecular scarring from chronic trabeculitis is the main mechanism
Summary Table
| Sign | Non-granulomatous (AAU) | Granulomatous (CAU) |
|---|---|---|
| Ciliary injection | Present | Often absent |
| Miosis | Yes | Variable |
| AC cells + flare | Yes | Yes |
| KP type | Fine, small | Mutton fat, pigmented |
| Hypopyon | Common (HLA-B27) | Rare |
| Fibrinous exudate | Common | Uncommon |
| Iris nodules | Koeppe nodules | Busacca + Koeppe |
| Posterior synechiae | Yes | Yes |
| Iris atrophy | Herpetic pattern | Diffuse (Fuchs) |
| Heterochromia | Fuchs syndrome | Fuchs syndrome |
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 12.
This is a shared conversation. Sign in to Orris to start your own chat.