a 34 year old female suffers from hair thinning hairfall and hair breakage from 2007
Clinical Assessment: 34-Year-Old Female with Hair Thinning, Hair Fall & Hair Breakage (since 2007 — ~17 years)
1. Differential Diagnosis
A. Androgenetic Alopecia (AGA) — Female Pattern Hair Loss
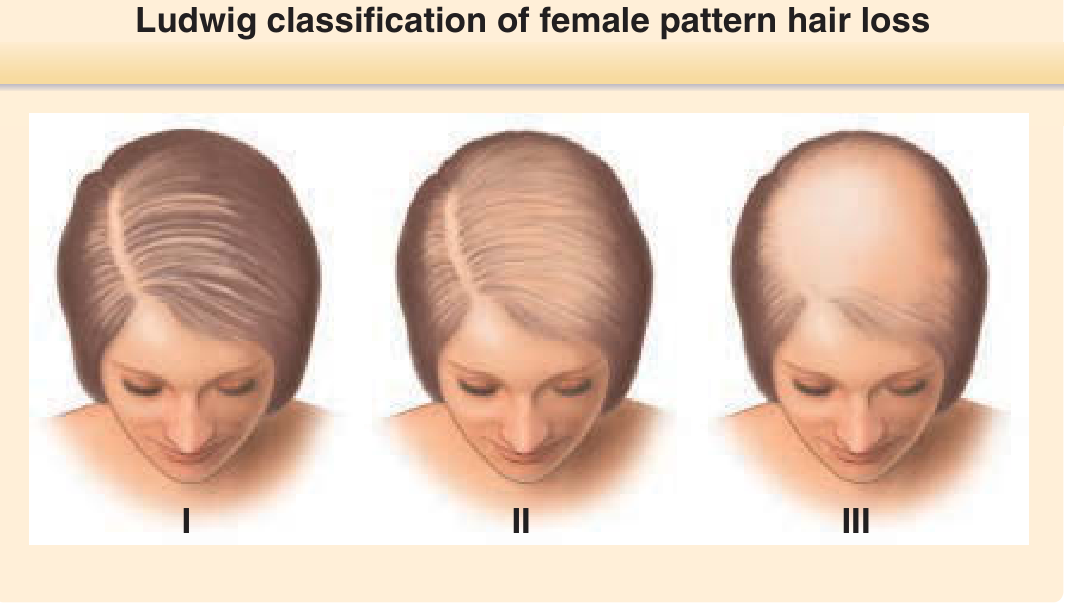
- Characterized by diffuse thinning of the centroparietal region with preservation of the frontal hairline (Ludwig pattern)
- The "Christmas tree pattern" — centroparietal thinning with breach of frontal hairline — is frequently seen in women
- Graded using the Ludwig scale (I–III) or Sinclair scale (I–V)
- Androgens play a role in a subset of women, particularly those with signs of hyperandrogenism (irregular periods, acne, hirsutism, PCOS)
- Polygenic inheritance; weak association with androgen receptor (AR/EDA2) locus and estrogen receptor 2 (ESR2) gene

B. Chronic Telogen Effluvium (CTE)
- Idiopathic diffuse club hair loss, often in women; shedding lasting >6 months to several years
- Typically affects women who previously had dense, long hair
- Marked bitemporal recession is frequently seen
- Must be distinguished from AGA — they can coexist
C. Chronic Diffuse Telogen Hair Loss (CDTHL) — Secondary Causes
| Category | Examples |
|---|---|
| Thyroid disorders | Hypothyroidism (Hashimoto's), hyperthyroidism |
| Nutritional deficiencies | Iron deficiency, zinc deficiency, protein malnutrition, biotin deficiency |
| Hormonal | PCOS, hyperprolactinemia, adrenal disorders |
| Medications | Hormonal contraceptives, retinoids, antithyroid drugs, anticoagulants |
| Systemic illness | Anaemia, autoimmune disorders (e.g., lupus), liver/kidney disease |
D. Hair Shaft Disorders (for Breakage)
- Trichorrhexis nodosa — trauma, chemical damage, nutritional deficiency
- Weathering/structural weakness from chronic styling, heat, chemical treatments
2. Key Diagnostic Workup
History
- Onset, progression, pattern (diffuse vs. frontal vs. vertex)
- Family history of hair loss
- Menstrual cycle history — oligomenorrhoea, PCOS symptoms
- Hormonal contraceptive use
- Nutritional habits, recent weight loss, crash dieting
- Medications since 2007
- Hair care practices (chemical treatments, heat styling, tight hairstyles)
Examination
- Pattern of loss — Ludwig vs. Christmas tree vs. diffuse
- Pull test (telogen effluvium positive — >6 hairs per pull)
- Scalp examination — scarring? scaling? inflammation?
- Signs of hyperandrogenism — acne, hirsutism, clitoromegaly
Investigations
| Test | Rationale |
|---|---|
| CBC | Anaemia |
| Serum ferritin | Iron deficiency (ferritin <30 ng/mL associated with hair loss) |
| TSH, free T4 | Thyroid disease |
| Total & free testosterone, DHEA-S | Androgen excess |
| Prolactin | Hyperprolactinemia |
| LH:FSH ratio | PCOS |
| Zinc, Vitamin D, B12 | Nutritional deficiencies |
| ANA | Autoimmune (if lupus suspected) |
| Trichoscopy | Miniaturization pattern in AGA; exclamation mark hairs in alopecia areata |
3. Management
Female Pattern Hair Loss (AGA)
| Treatment | Notes |
|---|---|
| Minoxidil 2–5% topical | First-line; stimulates anagen, prolongs hair cycle; applied daily |
| Oral minoxidil (low-dose 0.25–1 mg/day) | Emerging evidence; effective for diffuse thinning |
| Spironolactone (anti-androgen) | Useful in women with hormonal component; 50–200 mg/day |
| Finasteride / Dutasteride | Used off-label in postmenopausal women; avoid in women of childbearing age (teratogenic) |
| Platelet-Rich Plasma (PRP) | Adjunct; stimulates follicular growth |
| Low-Level Laser Therapy (LLLT) | FDA-cleared adjunct |
| Hair transplant | For advanced, stable AGA |
If Secondary Cause Found
- Treat the underlying condition (e.g., thyroxine for hypothyroidism, iron supplementation for deficiency, manage PCOS)
- Hair regrowth follows correction, but may take 6–12 months
For Hair Breakage
- Minimize heat, chemicals, mechanical traction
- Protein-rich diet, biotin supplementation if deficient
- Gentle hair care practices
Summary
a 34 year old female suffers from hair thinning hair fall and hair breakage from 2007. she has flaky itchy and oily scalp but the hair ends are rough and frizzy, there is widening of side parting and scalp is a bit vissible diffusely throughout the head. her HB is 13. she has 2 kids, a 3 year old and a 6 year old. what is the probable diagnosis and management
Probable Diagnosis
Primary Diagnosis: Female Pattern Androgenetic Alopecia (FPHL) — Ludwig Type
Secondary/Comorbid: Seborrheic Dermatitis of the Scalp
Clinical Reasoning
| Finding | Significance |
|---|---|
| Diffuse scalp visibility throughout head | Diffuse miniaturization — classic FPHL |
| Widening of side parting | Centroparietal thinning — Ludwig pattern FPHL |
| Hair thinning + hair fall since 2007 (~17 years) | Chronic, slowly progressive AGA |
| Flaky, itchy, oily scalp | Seborrheic dermatitis — co-occurs frequently with AGA (seborrhea is a recognized associated finding on AGA scalp examination) |
| Rough, frizzy hair ends | Hair shaft weathering/damage — not the same as root-level loss; points to structural fragility |
| Hair breakage | Combination of hair shaft weakness and seborrheic scalp inflammation weakening the fiber |
| Hb 13 g/dL | Low-normal in women (normal ≥12); borderline — iron stores (ferritin) need checking separately; not frank anaemia but may contribute |
| 2 children (ages 3 and 6) | Postpartum telogen effluvium likely occurred after both deliveries, potentially triggering/accelerating underlying AGA |
| Age 34, chronic course | Consistent with early-onset FPHL worsening over time |
Fitzpatrick's notes: "The scalp skin usually appears normal in AGA, but frequently associated findings include seborrhea and/or seborrheic dermatitis." — Fitzpatrick's Dermatology, Vol. 1 & 2
The pull test in AGA is typically positive in the frontal region, negative in the occipital region. Hair diameter variations and increased vellus hairs are seen on trichoscopy.
Differential Diagnoses to Rule Out
| Condition | Distinguishing Feature |
|---|---|
| Chronic Telogen Effluvium | Diffuse loss, no miniaturization; no family history; recovers; but may co-exist here |
| Alopecia Areata (diffuse type) | Exclamation mark hairs on trichoscopy; may have nail pitting |
| Scalp Psoriasis | Thick silvery plaques, not just flaking; coiled capillaries on dermoscopy |
| Tinea Capitis | Uncommon at 34; broken hairs, comma/corkscrew hairs on trichoscopy |
| Hypothyroidism | Diffuse loss + systemic features; check TSH |
| PCOS | Hyperandrogenism signs — irregular cycles, acne, hirsutism |
Investigations
Scalp
- Trichoscopy — hair diameter variation, vellus:terminal ratio, follicular openings (to exclude scarring), arborizing vessels (seborrheic dermatitis), peripilar sign (AGA)
Blood Tests
| Test | Purpose |
|---|---|
| Serum ferritin | Iron deficiency — ferritin <30 ng/mL associated with hair loss even with normal Hb |
| TSH, free T4 | Thyroid disease |
| Total & free testosterone, DHEA-S | Androgen excess / PCOS |
| LH : FSH ratio | PCOS |
| Prolactin | Hyperprolactinemia |
| Fasting blood glucose / insulin | Metabolic syndrome |
| Vitamin D, B12, zinc | Nutritional deficiencies |
| ANA | If autoimmune suspected |
Management
1. Female Pattern Hair Loss (AGA)
| Treatment | Details |
|---|---|
| Topical Minoxidil 2–5% | First-line. Apply to dry scalp once or twice daily. Takes 4–6 months to show response; must be continued indefinitely. 5% marginally more effective than 2% in women |
| Oral low-dose Minoxidil (0.25–1 mg/day) | Emerging evidence; useful if topical is poorly tolerated or insufficient response |
| Spironolactone 50–200 mg/day | Anti-androgen; add if hormonal workup suggests androgen excess or PCOS. Safe in women of childbearing age (use contraception) |
| Nutritional correction | If ferritin low → iron supplementation. Correct Vitamin D/B12/zinc if deficient |
| PRP (Platelet-Rich Plasma) | Adjunct every 3–6 months; stimulates follicular growth |
| Low-Level Laser Therapy (LLLT) | FDA-cleared adjunct device therapy |
| Hair transplant (FUE/FUT) | If disease is stable and advanced — long-term option |
2. Seborrheic Dermatitis (Scalp)
| Treatment | Details |
|---|---|
| Ketoconazole 2% shampoo | 2–3× per week; leave on scalp 3–5 minutes before rinsing; anti-fungal + anti-inflammatory |
| Zinc pyrithione shampoo | Maintenance; use 2–3× per week |
| Selenium sulfide shampoo | Alternative antifungal |
| Ciclopirox shampoo | If ketoconazole insufficient |
| Mild topical corticosteroid lotion (e.g., fluocinolone, clobetasol) | Short courses for flares with significant inflammation/itch; avoid prolonged use |
| Salicylic acid shampoo | If scaling is thick — helps debride crust |
Treating the seborrheic dermatitis actively is important — chronic scalp inflammation exacerbates hair fragility and may worsen hair loss.
3. Hair Shaft Damage / Breakage / Frizzy Ends
| Advice | Rationale |
|---|---|
| Minimize heat styling (straighteners, blow-dryers) | Thermal damage weakens hair shaft |
| Avoid harsh chemical treatments (bleaching, perming, relaxing) | Structural disulfide bond damage |
| Use gentle sulfate-free shampoo | Less stripping of scalp oils |
| Conditioning + deep conditioning treatments | Restore moisture to shaft |
| Wide-tooth comb on wet hair; detangle gently | Reduces mechanical breakage |
| Protein-enriched hair treatments | Temporarily strengthen damaged cuticle |
| Silk/satin pillowcase | Reduces friction |
| Trim split ends regularly | Prevents further shaft splitting |
Summary
- Trichoscopy to confirm miniaturization
- Check ferritin, TSH, androgens, Vitamin D
- Start Ketoconazole 2% shampoo for the seborrheic dermatitis
- Start Minoxidil 5% topical once scalp is not inflamed
- Address nutritional deficiencies found on workup
- Counsel on hair care practices
a 34 year old female suffers from hair thinning hair fall and hair breakage from 2007. she has flaky itchy and oily scalp but the hair ends are rough and frizzy, there is widening of side parting and scalp is a bit vissible diffusely throughout the head. Ocassionaly she can feel the bumps on scalp via her fingertips and mostly her scalp is painfull to touch and she has mild pain while hair brushing, her HB is 13. she has 2 kids, a 3 year old and a 6 year old. what is the probable diagnosis and management
Updated Clinical Picture: Key New Findings
| New Symptom | Significance |
|---|---|
| Palpable bumps on scalp | Suggests folliculitis (Malassezia/bacterial) or Malassezia folliculitis — a known complication of seborrheic dermatitis |
| Scalp painful to touch | Trichodynia — recognized symptom in both AGA and seborrheic inflammation; also seen in chronic telogen effluvium |
| Pain on hair brushing | Trichodynia; inflamed follicles are tender to mechanical stimulation |
Probable Diagnosis: Triple Pathology
1. Female Pattern Androgenetic Alopecia (FPHL) — Ludwig Type (Primary)
2. Seborrheic Dermatitis with Malassezia Folliculitis (Active complication driving scalp pain + bumps)
3. Hair Shaft Weathering / Structural Damage (Explaining rough, frizzy, breakage-prone ends)
Clinical Reasoning — Symptom by Symptom
| Finding | Explanation |
|---|---|
| Diffuse hair thinning + widening of side parting since 2007 | Chronic FPHL — Ludwig pattern miniaturization |
| Scalp visible diffusely | Diffuse follicular miniaturization |
| Oily, flaky, itchy scalp | Seborrheic dermatitis — Malassezia yeast overgrowth on sebaceous scalp |
| Palpable bumps on scalp | Malassezia (Pityrosporum) folliculitis — a direct complication of seborrheic dermatitis; pruritic follicular papules/pustules in sebaceous-rich areas |
| Scalp painful to touch + painful brushing | Trichodynia — perifollicular neurogenic inflammation; recognized early sign of AGA; also seen in inflamed seborrheic scalp |
| Hair breakage + rough, frizzy ends | Hair shaft structural damage — not follicular; from chronic inflammation, possible nutritional depletion, styling damage |
| Hb 13 g/dL (borderline) | Ferritin stores likely depleted; even normal Hb with low ferritin sustains hair loss |
| 2 children (ages 3 and 6) | Two postpartum telogen effluvium episodes — likely accelerated underlying AGA each time |
| Chronic duration since 2007 (~17 years) | Progressive AGA, not recovering telogen effluvium |
"Pruritus and trichodynia may present as initial signs of AGA." — Fitzpatrick's Dermatology, Vol. 1 & 2
"Malassezia (Pityrosporum) folliculitis is another complication [of seborrheic dermatitis] characterized by pruritic erythematous follicular papules, sometimes pustules, typically in sites rich in sebaceous glands." — Dermatology 2-Volume Set 5e
"Folliculitis, furuncles... are not uncommon complications [of scalp seborrheic dermatitis], elicited by scratching and rubbing." — Dermatology 2-Volume Set 5e
Differential Diagnoses to Actively Exclude
| Condition | Key Distinguishing Feature | How to Exclude |
|---|---|---|
| Scalp Psoriasis | Thick silvery-white plaques, sharply demarcated; coiled capillaries on dermoscopy | Dermoscopy, biopsy if needed |
| Lichen Planopilaris (LPP) | Perifollicular erythema, scale, scarring; loss of follicular ostia | Trichoscopy + biopsy |
| Frontal Fibrosing Alopecia | Band-like frontotemporal recession, eyebrow loss | Clinical exam |
| Chronic Telogen Effluvium | No miniaturization; trichodynia may be present; diagnosis of exclusion | Trichoscopy, ferritin |
| Dissecting Cellulitis of Scalp | Boggy, fluctuant painful nodules/sinuses | Clinical; more severe; commoner in men |
| PCOS / Hyperandrogenism | Irregular periods, hirsutism, acne | LH:FSH, testosterone, DHEA-S |
| Hypothyroidism | Systemic features — fatigue, weight gain, dry skin | TSH |
Investigations
Scalp Assessment
| Investigation | Purpose |
|---|---|
| Trichoscopy (dermoscopy) | Confirm miniaturization (AGA); arborizing vessels (seborrheic dermatitis); follicular ostia loss (scarring); follicular pustules (folliculitis) |
| Scalp swab (bacterial/fungal culture) | If folliculitis suspected — identify Malassezia vs. bacterial etiology |
| Scalp biopsy | If scarring alopecia cannot be excluded clinically |
Blood Tests
| Test | Why |
|---|---|
| Serum ferritin | Key — even Hb 13 with low ferritin (<30 ng/mL) drives hair loss |
| CBC with peripheral smear | Iron deficiency anaemia workup |
| TSH + free T4 | Thyroid disease |
| Total testosterone, free testosterone, DHEA-S | Androgen excess |
| LH : FSH ratio, fasting insulin | PCOS |
| Prolactin | Hyperprolactinemia |
| Vitamin D, B12, zinc | Nutritional deficiencies |
| ANA | Autoimmune screen (especially if LPP/lupus suspected) |
Management — Step-by-Step
Step 1: Treat the Active Scalp Inflammation FIRST
| Treatment | Regimen | Target |
|---|---|---|
| Ketoconazole 2% shampoo | 3× per week, leave 5 min before rinse | Seborrheic dermatitis + Malassezia folliculitis |
| Ciclopirox 1% shampoo | Alternate days (if ketoconazole insufficient) | Antifungal + anti-inflammatory |
| Zinc pyrithione shampoo | Maintenance 2–3× per week | Long-term control of SD |
| Topical low-potency corticosteroid lotion (e.g., fluocinolone acetonide 0.01%) | Short course for acute flare, 1–2 weeks | Reduce inflammation + pruritus |
| Salicylic acid shampoo | If thick scales present | Keratolytic — debride crust |
| Oral antifungal (e.g., Fluconazole 150 mg/week × 4 weeks) | If folliculitis is extensive or unresponsive | Systemic Malassezia control |
Step 2: Address FPHL (Once Scalp Calmer)
| Treatment | Details |
|---|---|
| Topical Minoxidil 5% solution or foam | Apply to dry scalp daily; first-line for FPHL; takes 4–6 months; must continue indefinitely |
| Oral low-dose Minoxidil (0.25–1 mg/day) | If topical poorly tolerated or scalp sensitivity persists |
| Spironolactone 50–100 mg/day | Add if hormonal workup confirms androgen excess or PCOS; safe in women of reproductive age (use contraception) |
| PRP therapy | Adjunct every 3 months — growth factors stimulate follicles |
| Low-Level Laser Therapy (LLLT) | FDA-cleared adjunct device |
Step 3: For Trichodynia / Scalp Pain
| Treatment | Mechanism |
|---|---|
| Treat the underlying seborrheic dermatitis/folliculitis | Resolves inflammatory pain component |
| Topical corticosteroid (short course) | Reduces perifollicular neurogenic inflammation |
| Topical minoxidil improvement of AGA | As AGA improves, trichodynia often subsides |
| Avoid tight hairstyles | Mechanical traction aggravates scalp pain |
Step 4: Hair Shaft Damage / Breakage / Frizzy Ends
| Advice | Rationale |
|---|---|
| Stop/minimize heat styling and chemical treatments | Structural hair shaft protection |
| Sulfate-free gentle shampoo + regular conditioning | Restore moisture balance |
| Weekly protein hair mask | Temporarily reinforces weakened cuticle |
| Trim split ends | Prevents further shaft splitting |
| Wide-tooth comb; never brush wet hair forcefully | Reduces mechanical breakage |
Step 5: Nutritional Correction
| Supplement | Indication |
|---|---|
| Elemental iron + Vitamin C | If ferritin <30 ng/mL |
| Vitamin D3 | If deficient |
| Vitamin B12 | If deficient |
| Zinc | If deficient |
| Biotin (only if frank deficiency) | Evidence weak for supplementation without deficiency |
Counselling Points
- Seborrheic dermatitis is chronic relapsing — not curable, but controllable with maintenance antifungal shampoos
- FPHL is progressive — the goal of treatment is arrest + partial regrowth, not full restoration; early treatment gives best outcomes
- Postpartum hair loss after both children likely accelerated existing AGA — hair fully recovered after delivery is not expected with underlying FPHL
- Minoxidil must be used long-term — stopping causes hair loss to resume
- Trichodynia (scalp pain) usually improves as inflammation is controlled
Summary Diagnosis
Female Pattern Androgenetic Alopecia (FPHL, Ludwig pattern) + Active Seborrheic Dermatitis with Malassezia Folliculitis + Trichodynia + Hair Shaft WeatheringTwo postpartum telogen effluvium episodes (after her children born ~2018 and ~2021) have likely superimposed on and worsened her underlying long-standing FPHL. Borderline Hb (13) warrants ferritin check. Active scalp folliculitis is driving the palpable bumps and scalp pain.
make a weekly routine plan with exact shampoo and supplements to take to manage this condition
Weekly Hair & Scalp Care Routine Plan
Phase 1: Active Treatment Routine (Months 1–3)
Morning Routine — Every Day
| Step | Product / Action | Instructions |
|---|---|---|
| 1. Scalp application | Minoxidil 5% topical solution or foam (e.g. Rogaine 5%, Tugain 5%, Mintop 5%) | Apply 1 mL directly to dry scalp along parting and diffuse thinning areas. Massage gently with fingertips for 1 min. Leave on — do NOT rinse. Wait 4 hours before washing hair |
| 2. Supplement | See supplement table below | Take with breakfast |
⚠️ Do NOT apply Minoxidil immediately after washing — scalp must be completely dry. Apply at least 30 min before styling.
Weekly Wash Schedule
| Day | Shampoo Used | Method & Contact Time |
|---|---|---|
| Monday | Ketoconazole 2% shampoo (e.g. Nizoral 2%, Ketomac, Sebifin Plus) | Wet scalp, apply shampoo to scalp (not just hair), lather and leave on 5 minutes, then rinse thoroughly |
| Tuesday | Rest day — no wash | If scalp feels oily, rinse with plain water only |
| Wednesday | Zinc Pyrithione shampoo (e.g. Head & Shoulders Clinical Strength, Selsun Blue for SD, Zinc-PT) | Apply to scalp, gentle massage 2–3 min, rinse. Follow with conditioner on lengths only |
| Thursday | Rest day — no wash | |
| Friday | Ketoconazole 2% shampoo | Same as Monday — 5 min contact time on scalp |
| Saturday | Ciclopirox 1% shampoo (e.g. Stieprox, Sebiprox) OR Selenium Sulfide 2.5% (e.g. Selsun Gold) | Apply, leave 3 min, rinse. Follow with moisturizing conditioner on ends only |
| Sunday | Rest day — scalp oil massage (optional) | Warm coconut oil or argan oil — apply to lengths and ends ONLY (not scalp — oil on scalp worsens SD). Leave 30 min, rinse |
Key rule: Never apply conditioner to the scalp — only to mid-lengths and ends. This prevents worsening oiliness and Malassezia overgrowth.
Once a Week — Scalp Treatment (Friday Night or Saturday)
| Step | Product | Instructions |
|---|---|---|
| Salicylic acid scalp serum/solution (e.g. Dermaceutic Activ Retinol, or any 2% salicylic acid scalp toner) | Apply to scalp, leave 15–20 min before Saturday shampoo | Loosens flaky scale, unblocks follicles, reduces palpable bumps |
| OR Topical steroid lotion — Fluocinolone acetonide 0.01% (e.g. Synalar lotion) | Apply to itchy, painful, bumpy areas only | Use maximum 4 consecutive weeks, then stop for 2 weeks |
Twice a Week (Evening) — Hair Conditioning
| Day | Treatment | Instructions |
|---|---|---|
| Wednesday evening | Deep conditioning hair mask (protein-based — e.g. Schwarzkopf Bonacure Repair Rescue, OGX Biotin & Collagen, TRESemmé Keratin Smooth mask) | Apply to mid-lengths and ends only. Leave 15–20 min. Rinse. Reduces breakage and frizz |
| Sunday (post-oil rinse) | Same as above, or lighter leave-in conditioner | Apply leave-in to damp ends; do not touch scalp |
Phase 2: Maintenance Routine (Month 4 Onwards — When Scalp Is Calm)
| Shampoo Rotation | Frequency |
|---|---|
| Ketoconazole 2% | Once a week (maintenance — prevents Malassezia relapse) |
| Zinc Pyrithione or Ciclopirox | Once a week |
| Gentle sulfate-free shampoo (e.g. Dove Nutritive Solutions, Sebamed Anti Hair-Loss Shampoo) | 1–2× per week for non-medicated wash days |
Maintenance is lifelong for seborrheic dermatitis — Malassezia has a slow proliferation rate, so relapses appear every few weeks if maintenance is stopped.
Daily Supplement Plan
| Supplement | Dose | When to Take | Why |
|---|---|---|---|
| Ferrous Sulphate 200 mg (provides 65 mg elemental iron) OR Iron Bisglycinate 25–50 mg (gentler on stomach) | Once daily | With Vitamin C (100–200 mg) at breakfast — enhances absorption. Avoid with tea/coffee/dairy | Ferritin target for hair regrowth: >70 ng/mL. Hb 13 makes iron deficiency very likely |
| Vitamin C 500 mg | Once daily | With iron supplement | Enhances iron absorption; antioxidant |
| Vitamin D3 2000–4000 IU | Once daily | With a fatty meal (lunch/dinner) | Deficiency very common in women; linked to hair cycling |
| Vitamin B12 500 mcg (methylcobalamin preferred) | Once daily | Morning with breakfast | Supports RBC formation; deficiency causes hair loss |
| Biotin 2500–5000 mcg (only if deficient) | Once daily | Morning | Benefit only proven in frank deficiency; still widely used |
| Zinc 25–50 mg (Zinc gluconate or zinc picolinate) | Once daily | With food (zinc on empty stomach causes nausea) | Zinc deficiency documented in both AGA and SD; supports follicle metabolism |
| Omega-3 Fatty Acids (Fish Oil) 1000–2000 mg EPA+DHA | Once daily | With a fatty meal | Anti-inflammatory; reduces scalp inflammation; improves hair shaft quality |
| Multivitamin with Hair Support (e.g. Viviscal Women, Nourkrin, Kérastase Initialiste Capsules, OR a basic women's multivitamin) | As directed | Morning | Broad micronutrient support |
Important: Do NOT take zinc and iron at the same time — they compete for absorption. Take iron at breakfast, zinc at dinner.
Hair Care Rules — Daily Habits
| Do | Don't |
|---|---|
| Use a wide-tooth comb on damp hair | Never brush soaking wet hair with a bristle brush |
| Detangle from ends upward, never root to tip | No tight ponytails, braids, or buns daily (traction worsens FPHL) |
| Allow hair to air dry when possible | No daily heat styling (straightener, curling iron, blow dryer on high heat) |
| Use a silk or satin pillowcase at night | No sleeping with wet hair tightly tied |
| Trim split ends every 6–8 weeks | No chemical treatments (bleach, relaxer, perm) during Phase 1 |
| Use heat protectant spray if heat styling is unavoidable | No harsh sulfate shampoos (SLS/SLES) |
What to Expect — Timeline
| Timeframe | Expected Progress |
|---|---|
| Week 1–2 | Scalp itching and oiliness begin to reduce with Ketoconazole shampoo |
| Week 3–4 | Palpable bumps (folliculitis) start to flatten; scalp pain reduces |
| Month 2 | Flaking significantly controlled; scalp tenderness mostly resolved |
| Month 3–4 | Hair breakage reduces; frizzy ends improve with conditioning routine |
| Month 4–6 | First signs of Minoxidil effect — reduced shedding; early new growth (fine hairs along parting) |
| Month 6–12 | Visible improvement in part-width and overall density |
| Ongoing | Maintenance shampoo rotation prevents SD relapse; Minoxidil must continue indefinitely |
"Seborrheic dermatitis tends to relapse if a maintenance regimen is not instituted... the interval of topical therapy should follow the proliferation rhythm of Malassezia." — Dermatology 2-Volume Set 5e
Quick Reference Weekly Summary
MON → Ketoconazole 2% shampoo (5 min) | Minoxidil morning | Iron + Vit C + D3 + B12
TUE → No wash | Minoxidil morning | Zinc at dinner
WED → Zinc Pyrithione shampoo | Deep conditioning mask (ends only) | All supplements
THU → No wash | Minoxidil morning | Zinc at dinner
FRI → Ketoconazole 2% shampoo (5 min) | Salicylic acid scalp pre-treatment | All supplements
SAT → Ciclopirox OR Selenium Sulfide shampoo | Minoxidil morning | Zinc at dinner
SUN → Oil treatment on lengths/ends only (30 min) → rinse | Deep condition ends | Rest day for supplements (optional)
can she dye her hair with herbatint hair colour?
Can She Use Herbatint Hair Colour?
What Is Herbatint?
- p-Phenylenediamine (PPD) or its derivatives — the colourant
- Hydrogen peroxide (developer) — low volume (typically 3–6%), but still oxidative
- Herbal extracts (aloe vera, walnut, etc.) added for conditioning
Why Timing Matters for This Patient
❌ NOT NOW — During Phase 1 (Active Seborrheic Dermatitis + Folliculitis)
| Reason | Explanation |
|---|---|
| Inflamed, broken skin barrier | Seborrheic dermatitis causes microerosions in the scalp. Applying any oxidative dye on a compromised barrier dramatically increases absorption of PPD and hydrogen peroxide — raising risk of severe allergic contact dermatitis |
| Active folliculitis (palpable bumps) | Open follicular pustules mean dye chemicals have direct access to dermis — intense burning, chemical injury, worsening infection |
| Scalp already painful (trichodynia) | Chemical exposure on an already sensitised, neurogenically inflamed scalp will cause severe burning and pain |
| Ketoconazole shampoo interaction | The acidic/alkaline pH shifts from frequent medicated shampoos alter the scalp's surface chemistry — this can affect dye uptake and increase irritation |
| Risk of worsening hair breakage | Hair shaft is already structurally weakened — oxidative chemistry (even low peroxide) causes further disulfide bond disruption, worsening breakage |
✅ When She CAN Use It — Phase 2 (Month 3–4 Onwards)
Before Application
- Patch test 48 hours before every single application — PPD sensitivity can develop even after years of safe use; inflamed scalps have increased sensitisation risk
- Do NOT apply to scalp the day of or day after a medicated shampoo — allow 48 hours gap after Ketoconazole or Ciclopirox wash
- Do NOT apply if scalp has any active bumps, cuts, soreness, or visible redness
- Wait at least 24–48 hours after applying Minoxidil — Minoxidil leaves a propylene glycol base on the scalp that can react with dye developer; wash scalp thoroughly first
During Application
- Apply to hair lengths first, then scalp last — minimise scalp contact time
- Limit contact time to the minimum recommended (do not exceed the stated time on the box)
- Do NOT use in a warm room or under a heat cap — heat increases skin permeability and chemical absorption
- Rinse thoroughly — at least 3–5 minutes of water flush
After Application
- Do NOT use Ketoconazole shampoo on the same day — use a gentle sulfate-free shampoo to rinse the dye out
- Resume medicated shampoo schedule the next wash day
- Deep condition hair ends immediately after — oxidative dye is drying; her already frizzy, weathered ends need moisture replenishment
Safer Alternatives Worth Considering
| Option | Pros | Cons |
|---|---|---|
| Herbatint (as discussed) | Low peroxide, conditioning herbs, widely available | Still oxidative; still contains PPD |
| Pure henna (100% Lawsonia inermis) | Truly chemical-free; no PPD; actually strengthens shaft | Only deposits red-orange tone; cannot darken or give brown/black; no lifting |
| Indigo + henna mix | Natural dark tones possible | Multi-step process; still stains scalp |
| Semi-permanent / demi-permanent dye | No ammonia; much lower peroxide | Less long-lasting; no significant lightening |
| Root touch-up powder/spray | Zero chemistry; no scalp contact | Temporary; cosmetic only |
Summary
| Scenario | Recommendation |
|---|---|
| Right now (active SD + folliculitis + scalp pain) | ❌ Avoid all hair dye — scalp too compromised |
| During Months 1–3 (Phase 1) | ❌ Wait — medicated shampoos and inflammation make it unsafe |
| From Month 3–4, when scalp is calm | ✅ Herbatint is acceptable — with patch test, timing gap from Minoxidil and medicated shampoos, and good post-colour conditioning |
| Long-term frequency | No more than every 6–8 weeks — more frequent application accelerates shaft weathering |
The "herbal" label on Herbatint does not make it safe to apply to an inflamed or broken scalp. The active chemistry remains oxidative and sensitising. The scalp must be fully settled before any permanent hair dye is used.
she has seen increased number of white hairs recently is it related to her condition
Is the Increase in White Hairs Related to Her Condition?
The Biology of Hair Colour
"Graying of hair results from a decreased number of melanocytes, which produce fewer melanosomes. Repetitive oxidative stress causes apoptosis of hair follicle melanocytes, resulting in normal hair graying. Premature graying is related to exhaustion of the melanocyte stem cell pool." — Andrews' Diseases of the Skin, Clinical Dermatology
How Her Conditions Are Contributing
1. Chronic Oxidative Stress from Seborrheic Dermatitis + Folliculitis
- Active scalp inflammation generates reactive oxygen species (ROS) at the follicular level
- Repetitive, sustained oxidative stress — as in her 17-year history of seborrheic dermatitis — directly causes apoptosis of follicular melanocytes
- Malassezia yeast itself generates oxidative byproducts that damage the follicular microenvironment
- Result: melanocyte stem cell exhaustion → white hairs appearing earlier than genetically expected
2. Androgenetic Alopecia (AGA)
- Miniaturising follicles in AGA undergo repeated accelerated hair cycles
- Each cycle is a "use" of the melanocyte stem cell reserve — more cycles = faster depletion
- Miniaturised follicles in AGA are also more metabolically stressed, worsening melanocyte survival
3. Nutritional Deficiencies — Likely Ongoing
| Nutrient | Link to Greying |
|---|---|
| Vitamin B12 | Most directly linked — B12 deficiency causes premature greying; reversal possible if caught early |
| Ferritin / Iron | Iron is a cofactor in melanin synthesis via tyrosinase enzyme |
| Vitamin D | Plays a role in melanocyte stem cell regulation and survival |
| Copper | Essential cofactor of tyrosinase — the enzyme that synthesises melanin |
| Zinc | Supports melanocyte function and antioxidant defence |
| Folate | Deficiency associated with premature greying in multiple studies |
4. Chronic Psychological Stress
- Two children under 6, 17 years of hair problems — chronic psychosocial stress elevates cortisol and norepinephrine
- Norepinephrine release depletes melanocyte stem cells in animal models — this is the validated mechanism behind the "stress turns hair white" phenomenon
- Chronic stress also worsens both AGA and seborrheic dermatitis — creating a vicious cycle
5. Possible Underlying Thyroid Disease (Not Yet Ruled Out)
- Both hypothyroidism and hyperthyroidism are associated with premature greying
- She hasn't had thyroid function checked yet — this is still in the pending workup
- Hashimoto's thyroiditis in particular is strongly linked to early greying and co-occurs with other autoimmune conditions
Is the Greying Reversible?
| Situation | Reversibility |
|---|---|
| B12 or folate deficiency corrected early | Partial to full repigmentation possible in some cases |
| Iron/copper/zinc corrected | May slow further greying; partial repigmentation unlikely but possible |
| Thyroid disease treated | Greying may slow or partially reverse |
| Scalp inflammation controlled | Stops further melanocyte damage — may preserve remaining pigmented follicles |
| Long-standing depletion of melanocyte stem cell pool | Irreversible — once the stem cell pool is exhausted, that follicle will remain white permanently |
What This Means for Her Management
Additional Blood Tests to Order Now
| Test | Purpose |
|---|---|
| Serum B12 (methylmalonic acid if borderline) | Most directly correctable cause of greying |
| Serum folate | Deficiency linked to premature greying |
| Serum copper | Tyrosinase cofactor |
| TSH + free T4 | Rule out thyroid disease (already recommended) |
Additional Supplements (if deficient)
| Supplement | Dose | Note |
|---|---|---|
| Methylcobalamin (B12) 1000–1500 mcg | Once daily | Most bioavailable form; supplement even if low-normal |
| Folic acid 400–800 mcg | Once daily | Supports melanin synthesis pathway |
| Copper 1–2 mg | Once daily | Do NOT take with zinc (competes) — take at a different time |
| Pantothenic acid (Vitamin B5) 500 mg | Once daily | Classically linked to melanocyte function; limited but consistent evidence |
Summary
- Chronic scalp oxidative stress from 17 years of seborrheic dermatitis and folliculitis is depleting her follicular melanocyte stem cells
- Nutritional deficiencies (especially B12, iron, copper) are impairing melanin production
- Accelerated follicular cycling from AGA exhausts the melanocyte reserve faster
- Chronic stress compounds all of the above
compile all the management steps ( weekly routines)with the shampoos and supplements for her
Complete Management Plan
PHASE 1 — Active Treatment (Months 1–3)
DAILY MORNING ROUTINE
| Step | Product | Instructions |
|---|---|---|
| 1 | Minoxidil 5% topical (Rogaine 5% / Tugain 5% / Mintop 5%) | Apply 1 mL to completely dry scalp along parting and thinning areas. Massage 1 min. Do NOT rinse. Wait 4 hrs before washing |
| 2 | Supplements (see table below) | Take with breakfast |
⚠️ Start Minoxidil only after the first 2 weeks — let the scalp calm slightly first. If scalp is very painful and bumpy in Week 1, delay until Week 3.
WEEKLY WASH SCHEDULE
| Day | Shampoo | Method |
|---|---|---|
| Monday | Ketoconazole 2% (Nizoral 2% / Ketomac / Sebifin Plus) | Wet scalp → apply to scalp → lather → leave 5 min → rinse. Conditioner on ends only |
| Tuesday | No wash — rest day | Plain water rinse only if needed |
| Wednesday | Zinc Pyrithione shampoo (Head & Shoulders Clinical Strength / Zinc-PT) | Apply to scalp → gentle massage 2–3 min → rinse. Conditioner on ends only |
| Thursday | No wash — rest day | |
| Friday | Ketoconazole 2% (same as Monday) | Same method — 5 min contact time |
| Saturday | Ciclopirox 1% (Stieprox / Sebiprox) OR Selenium Sulfide 2.5% (Selsun Gold) | Apply → leave 3 min → rinse. Follow with moisturising conditioner on ends only |
| Sunday | No wash — oil treatment day | Warm coconut or argan oil on lengths and ends ONLY (never scalp). Leave 30 min → rinse with plain water |
Key rule: Conditioner — lengths and ends ONLY, never the scalp. Oil — ends ONLY, never scalp. This prevents Malassezia flare-up.
ONCE WEEKLY — Scalp Pre-Treatment (Friday Night, before Saturday shampoo)
| Product | Instructions |
|---|---|
| Salicylic acid 2% scalp solution/serum (any brand — e.g. Paula's Choice BHA, or a pharmacy salicylic acid scalp toner) | Apply to scalp, leave 15–20 min, then shampoo as normal next morning. Loosens flakes, unblocks follicles, reduces palpable bumps |
| OR Fluocinolone acetonide 0.01% lotion (Synalar lotion — prescription) | Apply to painful/bumpy areas only. Use max 4 consecutive weeks, then pause 2 weeks |
TWICE WEEKLY — Hair Conditioning (Wednesday + Sunday)
| Day | Treatment | Instructions |
|---|---|---|
| Wednesday (post-wash) | Protein-based deep conditioning mask (Schwarzkopf Bonacure Repair Rescue / OGX Biotin & Collagen / TRESemmé Keratin Smooth mask) | Apply to damp mid-lengths and ends only. Leave 15–20 min. Rinse thoroughly |
| Sunday (post-oil rinse) | Same mask OR a lightweight leave-in conditioner | Apply to damp ends only. Do not touch scalp |
PHASE 2 — Maintenance (Month 4 Onwards, When Scalp Is Calm)
| Shampoo | Frequency |
|---|---|
| Ketoconazole 2% | Once a week (long-term maintenance — Malassezia returns in weeks without it) |
| Zinc Pyrithione or Ciclopirox | Once a week |
| Gentle sulfate-free shampoo (Dove Nutritive Solutions / Sebamed Anti Hair-Loss / Vanicream Free & Clear) | 1–2× per week on non-medicated days |
COMPLETE DAILY SUPPLEMENT SCHEDULE
Morning (with breakfast)
| Supplement | Dose | Purpose |
|---|---|---|
| Ferrous Bisglycinate (iron — gentler on stomach) OR Ferrous Sulphate 200 mg | 25–50 mg elemental iron once daily | Ferritin <30 ng/mL drives hair loss even when Hb is normal; target ferritin >70 ng/mL |
| Vitamin C | 500 mg | Take WITH iron — enhances absorption; do NOT drink tea/coffee/milk within 1 hr of iron |
| Methylcobalamin (Vitamin B12) | 1000–1500 mcg | B12 deficiency causes both hair loss AND premature greying; most bioavailable form |
| Folic acid | 400–800 mcg | Supports melanin synthesis; deficiency linked to premature greying |
| Biotin | 2500–5000 mcg | Supports keratin structure; benefit mainly if deficient |
| Vitamin B5 (Pantothenic acid) | 500 mg | Supports melanocyte function; linked to pigmentation |
With Lunch (fatty meal)
| Supplement | Dose | Purpose |
|---|---|---|
| Vitamin D3 | 2000–4000 IU | Very commonly deficient; regulates hair cycling and melanocyte stem cell survival |
| Omega-3 (Fish Oil — EPA+DHA) | 1000–2000 mg | Anti-inflammatory; reduces scalp inflammation; improves hair shaft strength and moisture |
With Dinner
| Supplement | Dose | Purpose |
|---|---|---|
| Zinc (Zinc Gluconate or Zinc Picolinate) | 25–50 mg | Supports follicle metabolism and sebum regulation; also cofactor for melanin |
| Copper | 1–2 mg | Essential cofactor of tyrosinase (melanin enzyme); take at dinner, separated from zinc |
⚠️ Critical spacing rules:
- Iron and zinc must NOT be taken together — they compete for absorption
- Copper and zinc must NOT be taken together — they antagonise each other
- Iron and calcium (dairy/antacids) must be separated by at least 2 hours
- Take iron on an empty stomach or with light food for best absorption
Optional: Hair-Specific Combination Supplement (if managing individual supplements is difficult)
| Product | Notes |
|---|---|
| Viviscal Women's Hair Growth | Contains AminoMar marine complex, biotin, zinc, iron, B vitamins — clinically studied |
| Nourkrin Woman | Marine protein, biotin, zinc, silica |
| Perfectil Plus Hair | Comprehensive hair/skin/nail formula with most needed micronutrients |
PRESCRIPTION MEDICATIONS (via Dermatologist)
| Medication | Dose | Purpose | Notes |
|---|---|---|---|
| Minoxidil 5% topical | 1 mL once daily to scalp | First-line FPHL treatment | Must be continued indefinitely; takes 4–6 months to show effect |
| Spironolactone | 50–100 mg/day | Anti-androgen for FPHL | Add after hormonal workup — if testosterone/DHEA-S elevated or PCOS confirmed; use contraception |
| Fluocinolone acetonide 0.01% lotion | Short courses only | Reduce scalp inflammation/trichodynia | Max 4 weeks at a time |
| Oral Fluconazole 150 mg/week × 4 weeks | Weekly for 4 weeks | If folliculitis does not respond to topical antifungals | Prescription only |
PENDING BLOOD TESTS (do before finalising supplement doses)
| Test | Why |
|---|---|
| Serum ferritin | Most important — guides iron supplementation |
| CBC | Full blood count, confirm Hb 13 picture |
| TSH + free T4 | Thyroid disease — linked to hair loss AND greying |
| Total testosterone + DHEA-S | Androgen excess / PCOS |
| LH : FSH ratio | PCOS |
| Prolactin | Hyperprolactinemia |
| Vitamin D (25-OH) | Guide D3 dose |
| Vitamin B12 + Serum folate | Guide B12/folate dose |
| Serum zinc + copper | Guide mineral supplementation |
| ANA | Autoimmune screen (especially if lichen planopilaris/lupus suspected) |
HAIR CARE RULES — DAILY HABITS
| ✅ Do | ❌ Don't |
|---|---|
| Wide-tooth comb on damp hair | Brush soaking wet hair with bristle brush |
| Detangle ends first, work upward | Tight ponytails, buns, or braids daily |
| Air dry whenever possible | Daily heat styling (straightener/blow dryer on high heat) |
| Silk or satin pillowcase at night | Sleep with wet hair tightly tied |
| Trim split ends every 6–8 weeks | Chemical treatments (bleach, perm, relaxer) during Phase 1 |
| Heat protectant if heat styling unavoidable | Harsh SLS/SLES sulfate shampoos |
| Gentle scalp massage (no scratching) | Scratching — worsens folliculitis and introduces infection |
HAIR DYEING RULE
| Phase | Decision |
|---|---|
| Phase 1 (Months 1–3, active inflammation) | ❌ No hair dye at all |
| Phase 2 (Month 4+, scalp calm) | ✅ Herbatint acceptable — patch test 48 hrs before; wait 48 hrs after medicated shampoo; wait 24 hrs after Minoxidil application; condition ends thoroughly after |
| Frequency | No more than every 6–8 weeks |
EXPECTED TIMELINE
| Time | What to Expect |
|---|---|
| Week 1–2 | Itching and oiliness start to reduce |
| Week 3–4 | Scalp bumps flatten; pain reduces |
| Month 2 | Flaking largely controlled; scalp tenderness resolves |
| Month 3 | Hair breakage reduces; frizzy ends improve |
| Month 3–4 | Minoxidil shedding phase may occur — temporary increase in fall, then stabilises |
| Month 4–6 | Reduced daily shedding; fine new hairs visible along parting |
| Month 6–12 | Measurable improvement in part width and overall density |
| Month 6+ | Greying may slow as nutritional deficiencies are corrected |
| Ongoing | Maintenance shampoo rotation lifelong; Minoxidil lifelong |
WEEKLY QUICK REFERENCE CARD
────────────────────────────────────────────────────────
MON Ketoconazole 2% shampoo (5 min contact)
Minoxidil 5% (morning, dry scalp)
Morning supps: Iron + Vit C + B12 + Folate + Biotin + B5
Lunch: Vit D3 + Omega-3
Dinner: Zinc + Copper
TUE No wash (plain water rinse if needed)
Minoxidil 5% (morning)
All supplements as above
WED Zinc Pyrithione shampoo (3 min)
Deep conditioning mask on ends (15–20 min)
Minoxidil 5% (morning)
All supplements as above
THU No wash
Minoxidil 5% (morning)
All supplements as above
FRI Salicylic acid scalp pre-treatment (evening, 15–20 min)
Ketoconazole 2% shampoo next morning (5 min contact)
Minoxidil 5% (morning)
All supplements as above
SAT Ciclopirox 1% OR Selenium Sulfide 2.5% shampoo (3 min)
Conditioning mask on ends
Minoxidil 5% (morning)
All supplements as above
SUN Oil (coconut/argan) on lengths + ends only (30 min → rinse)
Leave-in conditioner on damp ends
Minoxidil 5% (morning)
Rest day for supplements (optional)
────────────────────────────────────────────────────────
All prescription items must be initiated under a dermatologist's supervision. Supplement doses should be confirmed against actual blood test results before starting.
can neutrogena t gel shampoo be used in place of this ONCE WEEKLY — Scalp Pre-Treatment (Friday Night, before Saturday shampoo) Product Instructions Salicylic acid 2% scalp solution/serum (any brand — e.g. Paula's Choice BHA, or a pharmacy salicylic acid scalp toner) Apply to scalp, leave 15–20 min, then shampoo as normal next morning. Loosens flakes, unblocks follicles, reduces palpable bumps OR Fluocinolone acetonide 0.01% lotion (Synalar lotion — prescription) Apply to painful/bumpy areas only. Use max 4 consecutive weeks, then pause 2 weeks
Can Neutrogena T/Gel Replace the Friday Night Scalp Pre-Treatment?
What Is Neutrogena T/Gel?
| Action | Effect on Her Scalp |
|---|---|
| Keratolytic | Breaks down and loosens thickened scale and flakes — same action as salicylic acid |
| Antipruritic | Directly reduces scalp itch |
| Anti-inflammatory | Reduces the inflammatory component of seborrheic dermatitis |
| Antifungal (mild) | Has some activity against Malassezia, though weaker than ketoconazole |
| Cytostatic | Slows down abnormal skin cell turnover that drives scaling |
"Second-line treatment options [for seborrheic dermatitis] include zinc pyrithione, selenium sulfide, and tar shampoos as well as topical calcineurin inhibitors." — Dermatology 2-Volume Set 5e
Key Difference: How to Use It
| Salicylic Acid 2% Serum | Neutrogena T/Gel | |
|---|---|---|
| Form | Leave-on serum/solution | Rinse-off shampoo |
| Application | Apply to dry scalp, leave 15–20 min overnight, shampoo next morning | Apply to wet scalp, leave 5–10 min, then rinse off |
| Mode of action | Penetrates and dissolves scale while sitting overnight | Works during contact time on wet scalp |
| Can it be left on overnight? | ❌ No — coal tar is not designed for prolonged leave-on use; can cause photosensitisation and irritation if left on |
How to Incorporate T/Gel Into Her Routine
Option A — Use T/Gel as the Saturday Shampoo (Replaces Ciclopirox/Selenium)
| Day | Change |
|---|---|
| Friday night | Skip the salicylic acid pre-treatment |
| Saturday | Use T/Gel as the shampoo — wet scalp → apply → leave 5–10 min → rinse thoroughly. Follow with conditioner on ends only |
Option B — Use T/Gel as an Additional Scalp Treatment (Extended Contact)
- Apply T/Gel to dry or slightly damp scalp on Friday evening
- Leave for 20–30 min (not overnight)
- Then shampoo it off with Ketoconazole 2% or plain water
- This gives longer contact time for keratolytic and anti-inflammatory action
⚠️ Do NOT leave coal tar on overnight — it is a photosensitiser. Any residue on the scalp can make the skin sensitive to UV the next day.
Revised Friday–Saturday Slot With T/Gel
| Time | Action |
|---|---|
| Friday evening | Apply T/Gel to dry scalp → leave 20–30 min → rinse off (no full shampoo needed) |
| Saturday morning | Shampoo with Ketoconazole 2% (5 min contact) as usual → conditioner on ends |
| Time | Action |
|---|---|
| Saturday morning | Use T/Gel as the shampoo (5–10 min contact) → rinse → skip salicylic acid pre-treatment entirely |
One Caution Specific to Her Case
| Issue | Detail |
|---|---|
| Hair staining | Coal tar can impart a slight yellow-brown tint to light-coloured or grey/white hair — relevant since she has increasing white hairs |
| Odour | T/Gel has a distinctive medicinal tar smell; many find it strong |
| Photosensitivity | Rinse thoroughly and avoid direct sun for several hours after use |
| Minoxidil timing | Do not apply Minoxidil to scalp for at least 4 hours after T/Gel wash — let scalp fully dry first |
Bottom Line
| Question | Answer |
|---|---|
| Can T/Gel replace the salicylic acid pre-treatment slot? | ✅ Yes — it achieves the same goals (descaling, anti-itch, anti-inflammatory) via a different mechanism |
| Is it used the same way (leave-on overnight)? | ❌ No — used as a shampoo with 5–10 min contact, or as a 20–30 min scalp treatment before rinsing off |
| Is it better or worse than salicylic acid? | Different, not better or worse — salicylic acid is a pure keratolytic; T/Gel adds anti-inflammatory and mild antifungal benefits |
| Best placement in her weekly schedule | Saturday shampoo OR Friday evening extended-contact rinse-off treatment |
if t gel is used on friday then saturday wash with selsun blue can be done ?
Why T/Gel (Friday) + Selsun Blue (Saturday) Works
| Product | Active Ingredient | Primary Action |
|---|---|---|
| T/Gel (Friday) | Coal tar 0.5–1% | Keratolytic — loosens and lifts scale; anti-inflammatory; antipruritic |
| Selsun Blue (Saturday) | Selenium sulfide 1–2.5% | Antifungal — directly suppresses Malassezia; cytostatic (slows cell turnover) |
How to Do It
| Time | Action |
|---|---|
| Friday evening | Apply T/Gel to dry/slightly damp scalp → leave 20–30 min → rinse off thoroughly → pat dry |
| Friday night | Leave scalp bare — no oils, no products |
| Saturday morning | Wash with Selsun Blue 2.5% (or Selsun Gold) → apply to scalp → leave 3–5 min → rinse well → conditioner on ends only |
One Thing to Watch
| Issue | Detail |
|---|---|
| Scalp dryness | Using two active treatments on consecutive days can occasionally dry the scalp slightly — if this happens, reduce T/Gel contact time to 15 min instead of 30 |
| Selsun Blue odour + residue | Rinse very thoroughly on Saturday — selenium sulfide has a sulphurous smell and can leave a residue if not fully rinsed |
| Minoxidil on Saturday | Apply Minoxidil only after scalp is completely dry — at least 1–2 hours after Saturday wash |
| White hair staining | Selsun Blue (selenium sulfide) can cause a yellow discolouration on white or light grey hair with repeated use — rinse immediately and thoroughly to minimise this |
Updated Friday–Saturday Slot in Her Routine
FRIDAY EVENING
→ T/Gel to dry scalp → leave 20–30 min → rinse off
→ No other products overnight
SATURDAY MORNING
→ Selsun Blue 2.5% shampoo → 3–5 min contact → rinse thoroughly
→ Conditioner on ends only
→ Air dry → Minoxidil 5% once scalp is fully dry
compile the whole updated routine
Complete Updated Management Plan
PHASE 1 — Active Treatment (Months 1–3)
DAILY MORNING ROUTINE
| Step | Product | Instructions |
|---|---|---|
| 1. Minoxidil | Minoxidil 5% topical (Rogaine 5% / Tugain 5% / Mintop 5%) | Apply 1 mL to completely dry scalp along parting and thinning areas. Massage gently 1 min. Do NOT rinse. Wait at least 4 hrs before washing hair |
| 2. Supplements | See supplement table below | Take with breakfast/lunch/dinner as specified |
⚠️ If scalp is very painful and bumpy in Week 1, delay starting Minoxidil until Week 3 — let scalp calm first.
WEEKLY WASH & TREATMENT SCHEDULE
| Day | Time | Product | Instructions |
|---|---|---|---|
| MONDAY | Morning | Ketoconazole 2% shampoo (Nizoral 2% / Ketomac / Sebifin Plus) | Wet scalp → apply to scalp → lather → leave 5 min → rinse thoroughly. Conditioner on ends only. Air dry → Minoxidil once fully dry |
| TUESDAY | — | No wash | Plain water rinse only if scalp feels very oily. Minoxidil morning |
| WEDNESDAY | Morning | Zinc Pyrithione shampoo (Head & Shoulders Clinical Strength / Zinc-PT) | Apply to scalp → massage 2–3 min → rinse. Conditioner on ends only. Air dry → Minoxidil once fully dry |
| WEDNESDAY | Evening | Deep conditioning mask (Schwarzkopf Bonacure Repair Rescue / OGX Biotin & Collagen / TRESemmé Keratin Smooth) | Apply to damp mid-lengths and ends only. Leave 15–20 min. Rinse thoroughly |
| THURSDAY | — | No wash | Minoxidil morning |
| FRIDAY | Evening | Neutrogena T/Gel (coal tar 0.5–1%) | Apply to dry/slightly damp scalp → leave 20–30 min → rinse off thoroughly → pat dry. No other products overnight |
| SATURDAY | Morning | Selsun Blue 2.5% (selenium sulfide) | Apply to scalp → leave 3–5 min → rinse very thoroughly. Conditioner on ends only. Air dry → Minoxidil once fully dry |
| SATURDAY | Evening | Deep conditioning mask (same as Wednesday) | Apply to damp mid-lengths and ends only. Leave 15–20 min. Rinse |
| SUNDAY | Morning | No wash — Oil treatment | Warm coconut oil or argan oil on lengths and ends ONLY (never scalp). Leave 30 min → rinse with plain water → light leave-in conditioner on damp ends only |
SCALP INFLAMMATION / PAIN MANAGEMENT (As Needed)
| Situation | Product | Instructions |
|---|---|---|
| Active bumps + painful areas | Fluocinolone acetonide 0.01% lotion (Synalar — prescription) | Apply to affected scalp areas only (not whole scalp). Use maximum 4 consecutive weeks then pause 2 weeks |
| If bumps/folliculitis not clearing after 4 weeks of topical routine | Oral Fluconazole 150 mg once weekly × 4 weeks (prescription) | Under dermatologist supervision only |
PHASE 2 — Maintenance (Month 4 Onwards, When Scalp Is Calm)
| Day | Shampoo | Frequency |
|---|---|---|
| Once weekly | Ketoconazole 2% | Non-negotiable lifelong maintenance — prevents Malassezia relapse |
| Once weekly | Zinc Pyrithione or Ciclopirox 1% (Stieprox) | Alternates with ketoconazole week |
| Once weekly | T/Gel (Friday evening extended contact) + Selsun Blue (Saturday morning) | Monthly or fortnightly — reduce to once every 2 weeks when scale is well controlled |
| 1–2× weekly | Gentle sulfate-free shampoo (Dove Nutritive Solutions / Sebamed Anti Hair-Loss / Vanicream Free & Clear) | Non-medicated wash days |
COMPLETE DAILY SUPPLEMENT SCHEDULE
With Breakfast (Morning)
| Supplement | Dose | Purpose |
|---|---|---|
| Ferrous Bisglycinate (preferred) OR Ferrous Sulphate 200 mg | 25–50 mg elemental iron | Ferritin <30 ng/mL drives hair loss even with normal Hb; target ferritin >70 ng/mL |
| Vitamin C | 500 mg | Take WITH iron — enhances absorption. No tea/coffee/dairy within 1 hr |
| Methylcobalamin (B12) | 1000–1500 mcg | Deficiency causes hair loss AND premature greying |
| Folic acid | 400–800 mcg | Supports melanin synthesis; deficiency linked to greying |
| Biotin | 2500–5000 mcg | Supports keratin structure |
| Vitamin B5 (Pantothenic acid) | 500 mg | Supports melanocyte function and pigmentation |
With Lunch (Fatty Meal)
| Supplement | Dose | Purpose |
|---|---|---|
| Vitamin D3 | 2000–4000 IU | Regulates hair cycling and melanocyte stem cell survival |
| Omega-3 Fish Oil (EPA+DHA) | 1000–2000 mg | Reduces scalp inflammation; improves hair shaft strength |
With Dinner
| Supplement | Dose | Purpose |
|---|---|---|
| Zinc Gluconate or Zinc Picolinate | 25–50 mg | Follicle metabolism, sebum regulation, melanin cofactor |
| Copper | 1–2 mg | Tyrosinase cofactor — essential for melanin production; take separately from zinc |
⚠️ Critical spacing rules:
- Iron (breakfast) and Zinc (dinner) — never together, they compete for absorption
- Zinc and Copper — never together, they antagonise each other; both at dinner but separate by 1–2 hrs if possible, or copper at dinner and zinc before bed
- Iron and dairy/antacids — separate by at least 2 hours
- No tea or coffee within 1 hour of iron tablet
PRESCRIPTION MEDICATIONS (via Dermatologist)
| Medication | Dose | Purpose | Important Notes |
|---|---|---|---|
| Minoxidil 5% topical | 1 mL once daily | First-line FPHL treatment | Lifelong — stopping resumes hair loss; takes 4–6 months to show effect |
| Spironolactone | 50–100 mg/day | Anti-androgen for FPHL | Only after hormonal workup confirms androgen excess or PCOS; use contraception |
| Fluocinolone acetonide 0.01% lotion | Short courses | Scalp inflammation and trichodynia | Max 4 consecutive weeks at a time |
| Oral Fluconazole 150 mg/week | × 4 weeks | Severe/unresponsive folliculitis | Prescription only |
PENDING BLOOD TESTS
| Test | Purpose |
|---|---|
| Serum ferritin | Most important — guides iron dose |
| CBC | Full blood picture |
| TSH + free T4 | Thyroid disease — linked to hair loss and greying |
| Total testosterone + DHEA-S | Androgen excess / PCOS |
| LH : FSH ratio | PCOS |
| Prolactin | Hyperprolactinemia |
| Vitamin D (25-OH) | Guide D3 dose |
| Vitamin B12 + Serum folate | Guide B12 and folate dose |
| Serum zinc + copper | Guide mineral doses |
| ANA | Autoimmune screen |
HAIR CARE RULES
| ✅ Do | ❌ Don't |
|---|---|
| Wide-tooth comb on damp hair | Brush soaking wet hair |
| Detangle from ends upward | Tight ponytails, buns, braids daily |
| Air dry whenever possible | Daily heat styling on high heat |
| Silk or satin pillowcase | Sleep with wet hair tied |
| Trim split ends every 6–8 weeks | Chemical treatments (bleach, perm, relaxer) in Phase 1 |
| Heat protectant if heat styling needed | Harsh SLS/SLES sulfate shampoos |
| Gentle scalp massage with fingertips | Scratching scalp — worsens folliculitis |
HAIR DYEING RULE
| Phase | Decision |
|---|---|
| Phase 1 — Months 1–3 (active inflammation) | ❌ No hair dye at all |
| Phase 2 — Month 4+ (scalp calm) | ✅ Herbatint acceptable — patch test 48 hrs before; 48 hr gap after medicated shampoo; 24 hr gap after Minoxidil; deep condition ends after |
| Frequency | No more than every 6–8 weeks |
EXPECTED TIMELINE
| Timeframe | Expected Progress |
|---|---|
| Week 1–2 | Itching and oiliness begin to reduce |
| Week 3–4 | Scalp bumps flatten; pain and trichodynia reduce |
| Month 2 | Flaking largely controlled; scalp tenderness mostly resolved |
| Month 3 | Hair breakage reduces; frizzy ends improve with conditioning |
| Month 3–4 | Minoxidil shedding phase — brief temporary increase in fall, then stabilises |
| Month 4–6 | Reduced daily shedding; fine new hairs visible along parting |
| Month 6–12 | Measurable improvement in part width and overall density |
| Month 6+ | Greying may slow as nutritional deficiencies are corrected |
| Ongoing | Maintenance shampoo rotation lifelong; Minoxidil lifelong |
WEEKLY QUICK REFERENCE CARD
────────────────────────────────────────────────────
MON Morning: Ketoconazole 2% shampoo (5 min contact)
Air dry → Minoxidil 5%
Supps: Breakfast: Iron + Vit C + B12 + Folate + Biotin + B5
Lunch: Vit D3 + Omega-3
Dinner: Zinc + Copper
TUE No wash (water rinse if needed)
Morning: Minoxidil 5%
Supps: As above
WED Morning: Zinc Pyrithione shampoo (3 min)
Air dry → Minoxidil 5%
Evening: Deep conditioning mask on ends (15–20 min)
Supps: As above
THU No wash
Morning: Minoxidil 5%
Supps: As above
FRI Evening: T/Gel on dry scalp (20–30 min) → rinse off
No other products overnight
Morning: Minoxidil 5%
Supps: As above
SAT Morning: Selsun Blue 2.5% shampoo (3–5 min contact)
Air dry → Minoxidil 5%
Evening: Deep conditioning mask on ends (15–20 min)
Supps: As above
SUN Morning: Oil (coconut/argan) on lengths + ends only
(30 min) → rinse → leave-in conditioner on damp ends
Morning: Minoxidil 5%
Supps: As above (rest day optional)
────────────────────────────────────────────────────
All prescription medications must be initiated under a dermatologist's supervision. Supplement doses must be confirmed against actual blood test results before committing to full doses.