Epilepsy Clinical features Cause Diagnostics treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"epilepsy"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"epilepsy" AND "antiseizure"
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive material from multiple authoritative textbooks. Let me compose the full clinical reference answer.
Epilepsy: Complete Clinical Overview
Definition
Epilepsy is a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures, together with the neurobiologic, cognitive, psychological, and social consequences of this condition. A seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. Epilepsy is diagnosed after two unprovoked seizures, or one unprovoked seizure with high risk of recurrence. The active epilepsy prevalence is approximately 6 per 1000 persons.
1. Classification (ILAE 2017)
The 2017 International League Against Epilepsy (ILAE) classification operates at three levels:
| Level | Categories |
|---|---|
| Seizure type | Focal, Generalized, Unknown onset |
| Epilepsy type | Focal, Generalized, Combined, Unknown |
| Epilepsy syndrome | Age-specific (see below) |
At each level, an etiology should be assigned: Structural, Genetic, Infectious, Metabolic, Immune, or Unknown.
2. Clinical Features
A. Generalized Onset Seizures
Tonic-Clonic (Grand Mal)
- May be preceded by a prodrome (hours of irritability, depression) or myoclonic jerks on awakening
- Tonic phase (10-20 seconds): sudden loss of consciousness, fall, tonic stiffening, jaw clenching with lateral tongue bite, piercing cry, cyanosis, dilated unreactive pupils, bladder emptying
- Clonic phase (~30 seconds): rhythmic flexor spasms, autonomic activation (hypertension, tachycardia, salivation, sweating), apnea continues
- Postictal phase: deep coma, then confusion, agitation, drowsiness for minutes to hours; pulsatile headache on waking; no memory of the event
Absence Seizures
- Sudden onset, abrupt offset (seconds) - no postictal state
- Blank stare, cessation of activity, simple automatisms
- EEG: characteristic 3-Hz generalized spike-and-wave discharge
- Provoked by hyperventilation; multiple per day possible
- Remit by adolescence in ~60% of cases
Myoclonic Seizures - brief, shock-like jerks of trunk/limbs, often on awakening; seen in juvenile myoclonic epilepsy (JME)
B. Focal Onset Seizures
Focal Aware (formerly simple partial) - consciousness preserved; symptoms reflect locus:
- Motor: contralateral clonic jerking, tonic posturing, Todd paralysis post-ictally
- Sensory: contralateral tingling, numbness (somatosensory cortex); visual phenomena (occipital) - sparks, flashes, colors (red most common), or formed hallucinations (temporal-occipital junction)
- Auditory: buzzing, roaring, or voices (superior temporal gyrus)
- Visceral/Autonomic: epigastric rising sensation (most frequent aura - temporal lobe origin), palpitations
- Psychic: déjà vu, jamais vu, fear, euphoria, depersonalization
Focal Impaired Awareness (formerly complex partial) - impaired consciousness:
- Aura followed by behavioral arrest
- Automatisms: lip smacking, chewing, hand fumbling, ambulation
- Post-ictal confusion and fatigue (key distinguishing feature from absence)
- Typically 1-2 minutes duration
Temporal Lobe Seizures are the most common focal epilepsy in adults. Features include psychic experiences - illusions, hallucinations, depersonalization, and affective experiences.
Focal to Bilateral Tonic-Clonic - focal onset spreading to both hemispheres; secondary generalization implies a focal lesion.
C. Age-Related Distribution
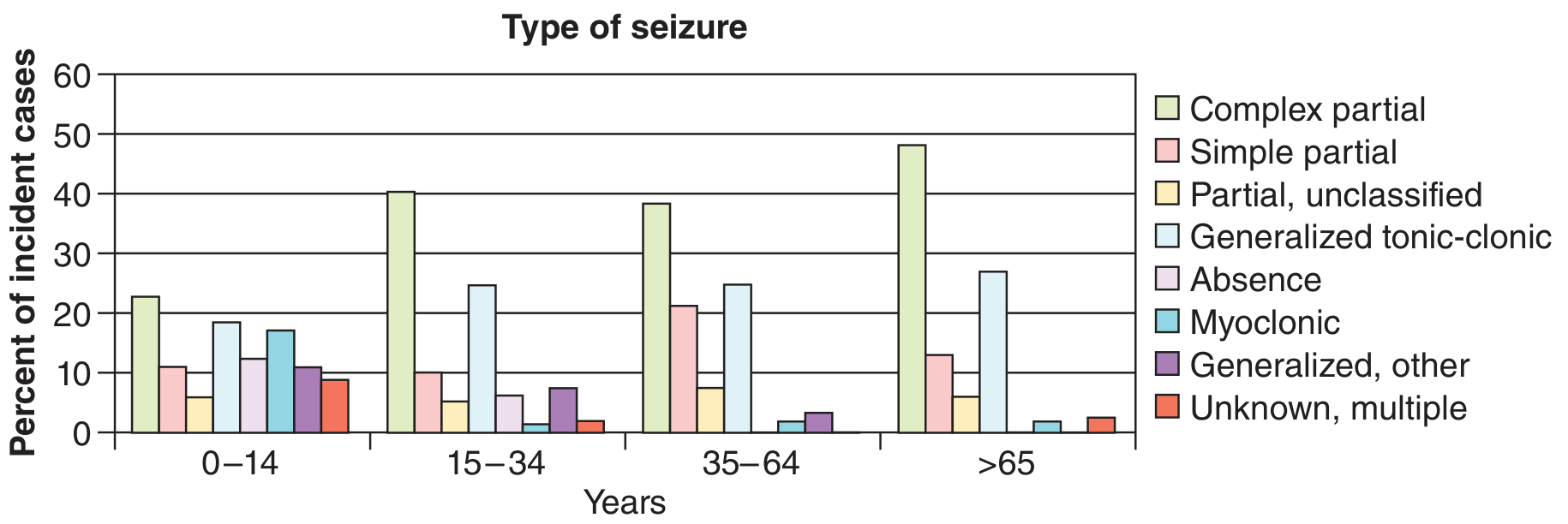
Absence and myoclonic seizures predominate in childhood; complex partial seizures dominate from age 15 onward and especially in the elderly (>65 years). - Adams and Victor's Principles of Neurology, 12th Ed
3. Causes / Etiology
Etiology is categorized by the ILAE into six groups:
| Category | Examples |
|---|---|
| Structural | Mesial temporal sclerosis, cortical dysplasia, hippocampal sclerosis, tumor (primary or metastatic), stroke/infarct, arteriovenous malformations, traumatic brain injury, porencephaly |
| Genetic | Ion channel mutations (SCN1A in Dravet syndrome), GABR mutations (GABRA1, GABRG2 in absence epilepsy), GLUT1 deficiency (SLC2A1), autosomal dominant nocturnal frontal lobe epilepsy, juvenile myoclonic epilepsy genes |
| Infectious | Neurocysticercosis (most common worldwide), tuberculoma, cerebral abscess, viral encephalitis (HSV), neurosyphilis, HIV encephalopathy |
| Metabolic | Hypoglycemia, hyponatremia, hypocalcemia, hypomagnesemia, hyperosmolarity, uraemia, hepatic failure, pyridoxine deficiency, mitochondrial disorders |
| Immune/Autoimmune | Anti-NMDAR encephalitis, anti-LGI1 antibodies, anti-CASPR2, Rasmussen encephalitis, other autoimmune encephalitides |
| Unknown | Idiopathic generalized epilepsies with no identifiable structural or genetic cause |
Age-related predominance:
- Neonates: hypoxic-ischemic encephalopathy, metabolic, intracranial hemorrhage, infections
- Infants/children: febrile seizures, genetic syndromes (West, Dravet, Lennox-Gastaut)
- Adolescents: idiopathic generalized epilepsies (JME, childhood absence)
- Adults: structural causes (trauma, tumor, stroke, mesial temporal sclerosis)
- Elderly: stroke (most common), neurodegenerative disease, tumor
4. Diagnosis
Epilepsy is fundamentally a clinical diagnosis supported by investigations.
History and Examination
- Detailed eyewitness account of the event (onset, duration, movements, postictal state)
- Personal/family history of seizures, febrile convulsions, birth injury
- Precipitants: sleep deprivation, alcohol, fever, photosensitivity, drugs
- Full neurological examination
Investigations
EEG (Electroencephalography)
- Most helpful laboratory test for epilepsy
- Epileptiform activity (spikes and sharp waves) - the only EEG finding with strong correlation to epilepsy
- Present in ~90% of epilepsy patients (depending on recording circumstances) but in only ~2% without epilepsy
- Normal interictal EEG does NOT exclude epilepsy
- Minor nonspecific abnormalities do NOT confirm epilepsy
- Absence seizures: diagnostic 3-Hz spike-and-wave; provoked by hyperventilation
- Video-EEG monitoring: gold standard - records ictal event simultaneously with clinical behavior; distinguishes epileptic from non-epileptic (psychogenic) spells
- Activation techniques: sleep deprivation, hyperventilation, photic stimulation (photoparoxysmal response)
| Feature | Absence | Complex Partial |
|---|---|---|
| Onset/offset | Abrupt | Gradual |
| Duration | Seconds | 1-2 minutes |
| Aura | No | Common |
| Postictal confusion | No | Yes |
| Automatisms | Simple | Complex |
| EEG | 3-Hz spike-wave | Focal discharge/slowing |
| Hyperventilation provocation | Common | Uncommon |
Neuroimaging
- MRI brain is the modality of choice (superior to CT) - detects mesial temporal sclerosis, cortical dysplasia, tumors, vascular malformations
- CT brain for acute settings (intracranial hemorrhage, trauma)
- [18F]FDG-PET: interictal hypometabolism at the seizure focus; useful in pre-surgical evaluation when MRI is normal
- Ictal SPECT (SISCOM): injected at seizure onset - shows ictal hyperperfusion; complementary to PET in pre-surgical evaluation
Blood Tests
- CBC, glucose, electrolytes (Na, Ca, Mg), renal and liver function, toxicology screen
- Consider amino acid screen in neonates/infants
CSF examination - reserved for suspected CNS infection; not routine
Genetic testing - increasingly used when genetic syndrome suspected
5. Treatment
General Principles
- Treatment is usually initiated after two unprovoked seizures
- Monotherapy preferred - start low, titrate slowly
- Serum drug levels guide compliance and toxicity; trough levels (pre-morning dose) are most consistent
- Higher serum concentrations needed for focal seizures than generalized ones
Antiseizure Drug (ASD) Selection by Seizure Type
| Seizure Type | First Line | Second Line | Third Line |
|---|---|---|---|
| Generalized tonic-clonic | Valproate, Carbamazepine | Lamotrigine, Oxcarbazepine | Phenytoin |
| Myoclonic | Valproate, Levetiracetam | Lamotrigine | Phenobarbital, Clobazam |
| Absence | Valproate, Ethosuximide | Topiramate, Levetiracetam | Lamotrigine |
| Focal (with/without impaired awareness) | Carbamazepine, Lamotrigine, Levetiracetam | Valproate, Oxcarbazepine | Topiramate, Vigabatrin |
| Infantile spasms (West) | ACTH, Vigabatrin | Valproate | - |
| Lennox-Gastaut | Valproate | Topiramate, Lamotrigine | Levetiracetam |
Broad-spectrum (both focal and generalized): Valproate, Levetiracetam, Lamotrigine, Phenytoin, Topiramate, Zonisamide
Narrow-spectrum (focal only): Carbamazepine, Oxcarbazepine, Gabapentin, Tiagabine, Pregabalin
Key Drug Notes
- Valproate: broad-spectrum; avoid in women of childbearing age (teratogenic - 20% serious adverse outcomes); monitor LFTs
- Carbamazepine: first-line focal; enzyme inducer; check for HLA-B*1502 (Stevens-Johnson risk in Asian patients)
- Lamotrigine: broad-spectrum; safest in pregnancy (1% serious adverse outcomes); slow titration to avoid rash
- Levetiracetam: broad-spectrum; renal dosing; behavioral side effects (irritability)
- Phenytoin: narrow therapeutic index; zero-order kinetics; gingival hyperplasia, hirsutism, nystagmus; available IV for acute use
- Ethosuximide: absence seizures only
Non-Pharmacological Treatment
Epilepsy Surgery
- Indicated for drug-refractory focal epilepsy (failure of 2 adequate AED trials)
- Pre-surgical evaluation: history, neuropsychological testing, video-EEG, high-resolution MRI, FDG-PET, ictal SPECT (SISCOM), depth EEG recordings
- Temporal lobectomy for mesial temporal lobe epilepsy - best outcomes (60-80% seizure-free)
- Hemispherectomy, corpus callosotomy for selected generalized syndromes
Vagal Nerve Stimulation (VNS)
- Adjunctive therapy for drug-resistant epilepsy when surgery is not feasible
- Reduces seizure frequency by 50% in ~50% of patients
Ketogenic Diet
- High-fat, low-carbohydrate diet; particularly effective in children and Dravet syndrome
- Produces ketosis, which reduces seizure susceptibility
Responsive Neurostimulation (RNS)
- Closed-loop cortical stimulation; detects and aborts seizures
- For patients with drug-resistant focal epilepsy
Special Situations
Status Epilepticus (seizure >5 minutes or failure to regain consciousness between seizures):
- Benzodiazepine IV (lorazepam/diazepam) - first-line
- Phenytoin/fosphenytoin or Levetiracetam IV - second-line
- Anesthetic agents (propofol, midazolam infusion) - refractory status
Pregnancy: Lamotrigine and Levetiracetam are safest ASDs. Valproate is most teratogenic and should be avoided. Folic acid supplementation 5 mg/day. Women with epilepsy have a tenfold higher risk of death compared to pregnant women without epilepsy.
Driving: Most jurisdictions require a seizure-free period (typically 1 year) before driving is permitted.
Lifestyle: Avoid precipitants - sleep deprivation, alcohol, flickering lights; maintain regular medication schedule.
Summary Framework
EPILEPSY
├── CAUSES (ILAE 6 categories)
│ ├── Structural (tumor, stroke, dysplasia, trauma)
│ ├── Genetic (channelopathies, SCN1A, GABA receptor genes)
│ ├── Infectious (NCC, encephalitis)
│ ├── Metabolic (electrolytes, glucose, organ failure)
│ ├── Immune (anti-NMDAR, LGI1, Rasmussen)
│ └── Unknown
├── CLINICAL FEATURES
│ ├── Focal (aware/impaired awareness → temporal, frontal lobe)
│ └── Generalized (tonic-clonic, absence, myoclonic)
├── DIAGNOSIS
│ ├── EEG (epileptiform spikes; video-EEG gold standard)
│ ├── MRI brain (structural lesion)
│ └── Bloods, PET/SPECT (pre-surgical)
└── TREATMENT
├── Pharmacological (ASD - matched to seizure type)
├── Surgical (temporal lobectomy for refractory focal)
├── VNS / RNS / DBS
└── Ketogenic diet
Sources: Bradley and Daroff's Neurology in Clinical Practice | Adams and Victor's Principles of Neurology, 12th Ed | Goldman-Cecil Medicine | Grainger & Allison's Diagnostic Radiology | Rosen's Emergency Medicine | Katzung's Basic and Clinical Pharmacology, 16th Ed
Recent evidence note: A 2025 genome-wide meta-analysis (PMID 40240269) identified genetic loci contributing to drug-resistant epilepsy, supporting future pharmacogenomic treatment stratification. A 2024 Cochrane review on cenobamate (PMID 39087564) confirmed efficacy as add-on therapy for drug-resistant focal epilepsy - a newer option worth considering for refractory cases.
This is a shared conversation. Sign in to Orris to start your own chat.