btb graft
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
bone patellar tendon bone BTB graft ACL reconstruction
Here is a comprehensive overview of the Bone–Patellar Tendon–Bone (BTB / BPTB) Graft for ACL reconstruction:
BTB (Bone–Patellar Tendon–Bone) Graft
What It Is
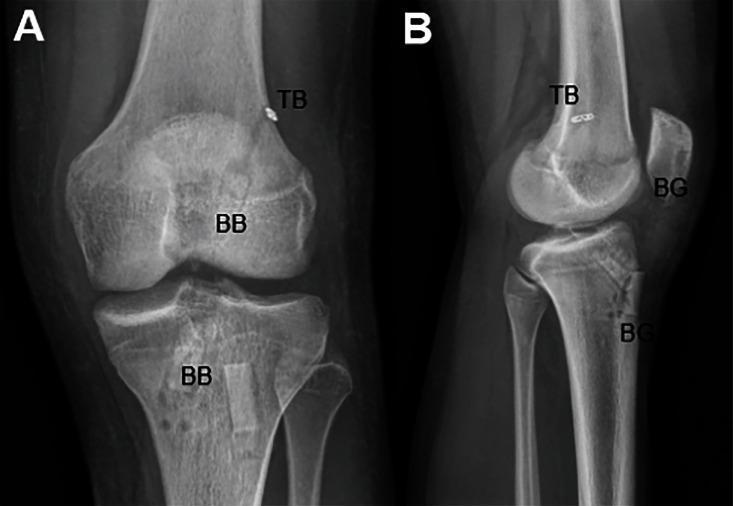
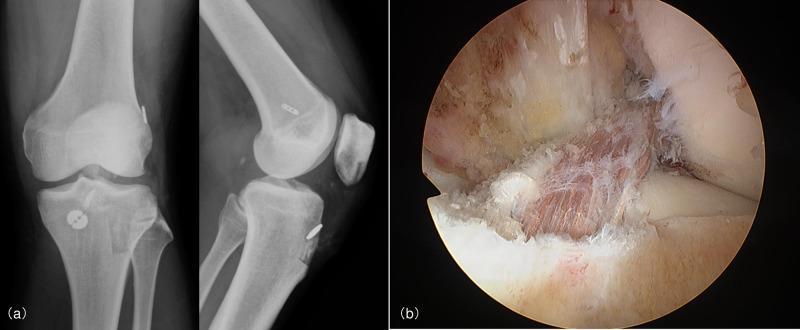
The BTB graft uses the central third of the patellar tendon with a bone plug at each end — one from the patella and one from the tibial tuberosity. It is one of the primary autograft options for ACL reconstruction, alongside hamstring and quadriceps tendon grafts.

Biomechanics
- Tensile strength of a 10-mm patellar tendon graft (young specimen): >2900 N — approximately 30% stronger when rotated 90°, though this strength diminishes in vivo
- Native ACL tensile strength: ~2200–2500 N (young individuals)
- BTB is therefore initially stronger than the native ACL
— Miller's Review of Orthopaedics 9th Edition, p. 340
Advantages
- Faster bone-tunnel incorporation than hamstring autograft — bone-to-bone healing via the bone plugs is more reliable and quicker than tendon-to-bone healing
- Often the graft of choice for early return to sports
- Predictable, reproducible harvest
- Excellent long-term track record
— Miller's Review of Orthopaedics 9th Edition, p. 351
Disadvantages / Donor Site Morbidity
- Anterior knee pain (most commonly reported)
- Pain with kneeling
- Loss of extension postoperatively
- Poorer recovery of quadriceps strength compared to hamstring graft
- Risk of patellar fracture (incidence ~0.2%) — both at harvest and postoperatively
- Higher incidence of arthritis at 5–7 years post-reconstruction compared to hamstring autograft
— Miller's Review of Orthopaedics 9th Edition, p. 351
Graft Fixation
The bone plugs are press-fit and fixed with interference screws in the femoral and tibial tunnels. Newer techniques also use suspensory fixation (e.g., TightRope button on the lateral femoral cortex).
Surgical Technique Notes
- Femoral tunnel placement is critical — most common error: too far anterior, causing flexion loss
- Vertical graft placement → decreased rotational stability; more horizontal placement (anatomic position, 10- or 2-o'clock) reduces rotational instability
- Interference screw divergence >30° (femoral) or >15° (tibial) leads to complications
- Rectangular tunnel geometry has been described to better match the BTB graft profile
BTB vs. Other Grafts — Comparison
| Feature | BTB Autograft | Hamstring Autograft | Allograft |
|---|---|---|---|
| Tensile strength | >2900 N | ~4000 N (quadrupled) | Variable |
| Bone incorporation | Fast (bone-to-bone) | Slower (tendon-to-bone) | Slowest |
| Anterior knee pain | Common | Less common | Absent |
| Return to sport | Faster | Slightly slower | Slower |
| Arthritis risk (5–7 yr) | Higher | Lower | — |
| Infection risk | Very low | Very low | Low (1:6 million for HIV) |
| Use in revision | Yes (with bone block) | Yes (ipsilateral or contralateral) | Option when autograft unavailable |
Rehabilitation
- Early motion and weight bearing encouraged
- Avoid open kinetic chain quadriceps exercises (0–30° of flexion) — stresses the graft
- Closed kinetic chain exercises preferred
- Postoperative bracing not proven beneficial (except in downhill skiers)
- Full ROM and good quadriceps control should be achieved before surgery
— Miller's Review of Orthopaedics 9th Edition, p. 352
Complications
- Arthrofibrosis — most common overall complication; risk minimized by achieving full ROM pre-op
- Graft failure (tunnel malposition is #1 technical cause)
- Patellar fracture (at harvest or post-op)
- Infection (<1%); irrigation and debridement with graft retention successful in ~85% of cases
This is a shared conversation. Sign in to Orris to start your own chat.