Current guidelines to treat spondylolysthesis from grade 1 to 5 in details
Reading File
Finding Sources
Finding Sources
Searching Images
spondylolisthesis grades classification treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive information to provide a detailed, well-structured answer. Let me compile it:
Spondylolisthesis: Grading & Treatment Guidelines (Grade I–V)
Classification & Grading
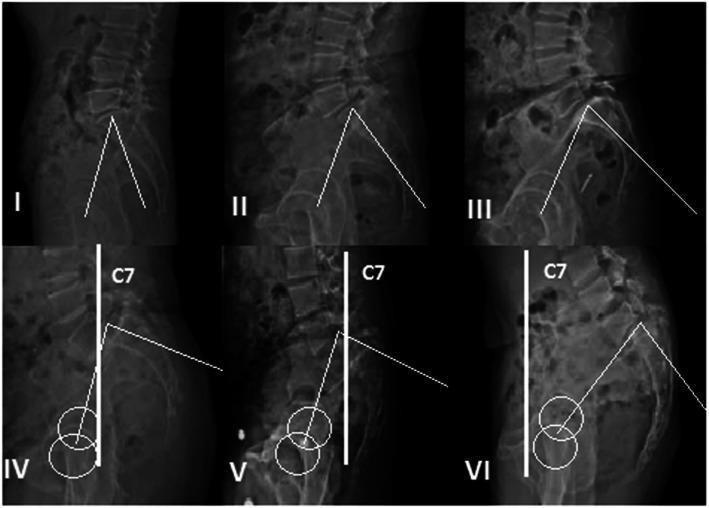
Meyerding Classification — based on percentage of forward vertebral slip relative to the vertebral body below:
| Grade | Slip % | Description |
|---|---|---|
| I | 1–25% | Low-grade |
| II | 26–50% | Low-grade |
| III | 51–75% | High-grade |
| IV | 76–100% | High-grade |
| V | >100% | Spondyloptosis (complete dislocation) |
Wiltse Classification (etiology):
- Type I – Dysplastic (congenital dysplasia of S1 facets; highest risk of progression)
- Type II – Isthmic (pars interarticularis defect; most common, L5–S1)
- Type III – Degenerative (facet arthrosis; most common at L4–L5, women >40 yrs)
- Type IV – Traumatic
- Type V – Pathological
- Type VI – Post-surgical
Key Radiographic Measurements
- Slip angle: Measured from the superior endplate of L5 to a line perpendicular to the posterior sacrum. Values >45–50° indicate high risk of progression, instability, and postoperative pseudarthrosis.
- Pelvic incidence (PI): Normal ~50°. PI = pelvic tilt (PT) + sacral slope (SS). Increased PI predisposes to higher-grade slippage.
- Sacral inclination: Normally >30°.
Treatment by Grade
Grade I (1–25% slip)
Asymptomatic:
- No treatment required.
- Younger/skeletally immature patients: serial monitoring for progression (risk of progression requiring surgery <5%).
- Adolescents with grade I slip may return to full activities, including contact sports, once asymptomatic.
Symptomatic:
- Nonoperative (first-line):
- Activity modification and relative rest
- Lumbar flexion-based exercises; hamstring stretching; core strengthening
- NSAIDs for pain control
- Physical therapy
- Antilordotic bracing (TLSO with thigh extension) in acute/active phases, especially in adolescents
- Operative (if conservative treatment fails after 6 months, or neurologic symptoms develop):
- In situ posterolateral fusion (L5–S1 most commonly)
- Decompression only if neurologic compression is present
- Reduction is generally not attempted in low-grade slips; fusion in situ is standard
Grade II (26–50% slip)
Asymptomatic:
- No active treatment, but activity restriction recommended (avoid gymnastics, football, heavy contact sports).
- Close observation with serial radiographs to monitor for progression.
Symptomatic:
-
Nonoperative (first-line):
- Same as grade I: activity modification, flexion-based PT, core strengthening, NSAIDs, bracing
- Trial of 3–6 months conservative management
-
Operative indications:
- Failure of conservative management
- Persistent or progressive neurologic deficit
- Progressive radiographic slip
-
Operative options:
- Pediatric/adolescent: posterolateral fusion (PLF), typically L4 to S1; instrumented fusion preferred
- Adult: decompression (if stenosis/radiculopathy present) + posterolateral fusion; TLIF or PLIF considered for interbody support
- Instrumented fusion (pedicle screws) improves fusion rates
- Reduction not routinely required
Grade III (51–75% slip) — High-Grade
These are typically symptomatic and require surgical planning:
-
Nonoperative: rarely adequate for high-grade slips; conservative care may be used to optimize the patient prior to surgery
-
Operative (generally indicated):
- Posterior decompression (laminectomy) to free neural elements, especially L5 nerve root
- Posterolateral instrumented fusion, typically L4–S1 or L4–S1 with iliac fixation for added stability
- Reduction of deformity: partial or complete reduction may be attempted to restore sagittal alignment, reduce lumbosacral kyphosis (slip angle correction), and improve fusion bed — but carries risk of L5 nerve root injury
- Interbody fusion (TLIF/PLIF or anterior interbody) often added to maximize fusion surface
- Pelvic fixation (iliac screws) may be required in high-grade slips with sacropelvic instability
- Slip angle >45–50° is a critical threshold indicating high deformity risk
-
Pediatric high-grade slip (>50%):
- Higher rate of progression; surgical stabilization is the standard of care
- Fusion typically from L4 to S1
Grade IV (76–100% slip) — High-Grade
- Surgical treatment is mandatory in virtually all cases
- Complex deformity correction: significant lumbosacral kyphosis, abnormal sacropelvic parameters must be addressed
- Staged approach may be necessary: anterior release/interbody fusion followed by posterior instrumented reduction and fusion
- Neurologic monitoring (IONM) is critical intraoperatively
- L5 and S1 nerve root decompression is prioritized before reduction attempts
- Circumferential fusion (360°) with anterior interbody + posterior instrumented PLF is the most reliable construct
- Iliopelvic fixation commonly required
- Complication rate is substantial: neurologic deficit (especially L5 palsy), pseudarthrosis, hardware failure, junctional kyphosis
Grade V — Spondyloptosis (>100%, complete dislocation)
- L5 is completely displaced anterior to the sacrum
- Represents the most severe form; almost always requires surgery
- Objectives: neural decompression, restoration of sagittal balance, solid arthrodesis
- Surgical options:
- In situ fusion without reduction: lower neurologic risk, but poor correction of deformity; reserved for patients with significant neurologic risk
- Reduction and fusion: preferable for sagittal balance restoration; high risk of L5 nerve root injury
- L5 vertebrectomy (Gaines procedure): removes the L5 vertebra entirely, allows the spine to sit on the sacrum; reserved for severe cases where reduction is not feasible; risk of neurologic deficit
- Posterior instrumented fusion with iliopelvic fixation is mandatory
- Anterior column support (interbody cage/graft) essential
- Requires multidisciplinary planning; performed at high-volume spine centers
Degenerative Spondylolisthesis (Special Consideration — typically Grades I–II)
- More common in women, typically at L4–L5
- Presents with symptoms of spinal stenosis (neurogenic claudication, bilateral radiculopathy)
- Nonoperative: physical therapy, epidural steroid injections, weight loss, NSAIDs
- Operative: decompression (laminectomy) + posterolateral fusion
- The SPORT trial (4-year follow-up) showed significant improvement in pain and function with surgery vs. nonoperative treatment
- Decompression alone (without fusion) carries risk of iatrogenic instability and is generally not recommended
Summary Table
| Grade | Slip | Symptoms | First-Line | Surgical Indication | Procedure |
|---|---|---|---|---|---|
| I | 0–25% | Asymptomatic → observe; Symptomatic → PT/NSAIDs | Nonoperative | Failed conservative Rx, neuro deficit | In-situ PLF ± decompression |
| II | 25–50% | Activity restriction + PT | Nonoperative | Same + progressive slip | Instrumented PLF ± interbody |
| III | 50–75% | Usually symptomatic | Surgery strongly considered | Near always | Instrumented PLF, reduction, interbody, ± iliopelvic fixation |
| IV | 75–100% | Symptomatic | Surgery mandatory | Always | Circumferential fusion, reduction, IONM |
| V | >100% | Severe | Surgery mandatory | Always | In-situ fusion or L5 vertebrectomy (Gaines) |
Sources:
- Miller's Review of Orthopaedics, 9th Edition (Wiltse classification table, treatment algorithms)
- Bailey and Love's Short Practice of Surgery, 28th Edition (Meyerding classification, Wiltse classification table)
- SPORT Trial data cited in Miller's Review of Orthopaedics — degenerative spondylolisthesis surgical outcomes
This is a shared conversation. Sign in to Orris to start your own chat.