Tell me about heart sound ,it's significance and murmurs and reason behind them as well
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a thorough, well-illustrated answer. Let me compile the full response.
Heart Sounds, Their Significance, and Murmurs
The Normal Heart Sounds
When you listen to a normal heart with a stethoscope, you hear a rhythm described as "lub-dub, lub-dub." These are the first (S1) and second (S2) heart sounds, and they bracket systole.
S1 - The First Heart Sound ("Lub")
S1 is caused by closure of the mitral (bicuspid) and tricuspid valves at the very start of ventricular systole. The mechanism:
- Ventricular contraction creates a sudden backflow of blood against the AV valves.
- The valves close and bulge toward the atria until the chordae tendineae snap them taut.
- The elastic recoil bounces blood back into the ventricles.
- This causes the valve leaflets, ventricular walls, and blood itself to vibrate, producing the "lub" sound that travels to the chest wall.
S1 is louder and lower-pitched than S2 because the AV valves are less taut (they vibrate longer, ~0.14 sec).
Significance: Splitting of S1 is best heard at the tricuspid area. A loud S1 is seen in mitral stenosis; a soft S1 occurs with first-degree heart block or mitral regurgitation.
S2 - The Second Heart Sound ("Dub")
S2 results from closure of the aortic and pulmonary (semilunar) valves at the end of systole.
- When the semilunar valves close, they bulge back toward the ventricles.
- Their elastic recoil sends blood rebounding between the arterial walls and the valves, producing vibrations that travel along vessel walls to the chest wall.
- Duration: ~0.11 sec (shorter because semilunar valves are tauter).
- Higher pitch than S1 for two reasons: greater tautness of semilunar valves, and greater elastic coefficient of the arterial walls serving as the resonating chamber.
Significance: Splitting of S2 is physiologically normal on inspiration (increased venous return to the right heart delays pulmonary valve closure). Fixed splitting is a hallmark of atrial septal defect. Paradoxical splitting (splitting on expiration) is a sign of aortic stenosis or left bundle branch block.
S3 - Third Heart Sound (Ventricular Gallop)
S3 occurs at the beginning of the middle third of diastole - a soft, low-frequency rumble caused by blood rushing from the atria into a partially filled ventricle. As blood inrushes and the ventricular walls suddenly distend, oscillations are set up within the ventricular blood pool, generating a short reverberation.
Significance:
- Normal in children, adolescents, and young adults (physiological S3).
- In adults over 40, S3 generally indicates systolic heart failure (reduced ejection fraction, increased end-diastolic volume).
- Creates the "Ken-tuck-Y" gallop rhythm (S1 - S2 - S3).
S4 - Fourth Heart Sound (Atrial Gallop)
S4 occurs just before S1, at the time of atrial contraction (late diastole). It is caused by the forceful atrial kick pushing blood into a stiff ventricle, causing vibrations similar to S3. Frequency is usually ~20 cycles/sec - at the very threshold of human hearing, often only recordable by phonocardiography.
Significance:
- Seen when there is decreased ventricular compliance (stiff left ventricle) - such as left ventricular hypertrophy, hypertensive heart disease, aortic stenosis, hypertrophic cardiomyopathy.
- Creates the "Ten-NES-see" gallop (S4 - S1 - S2).
- A summation gallop (S3 + S4 merging) can occur at rapid heart rates and strongly suggests significant cardiac disease.
Auscultation Areas
The four classic areas where each valve's sounds are best heard:
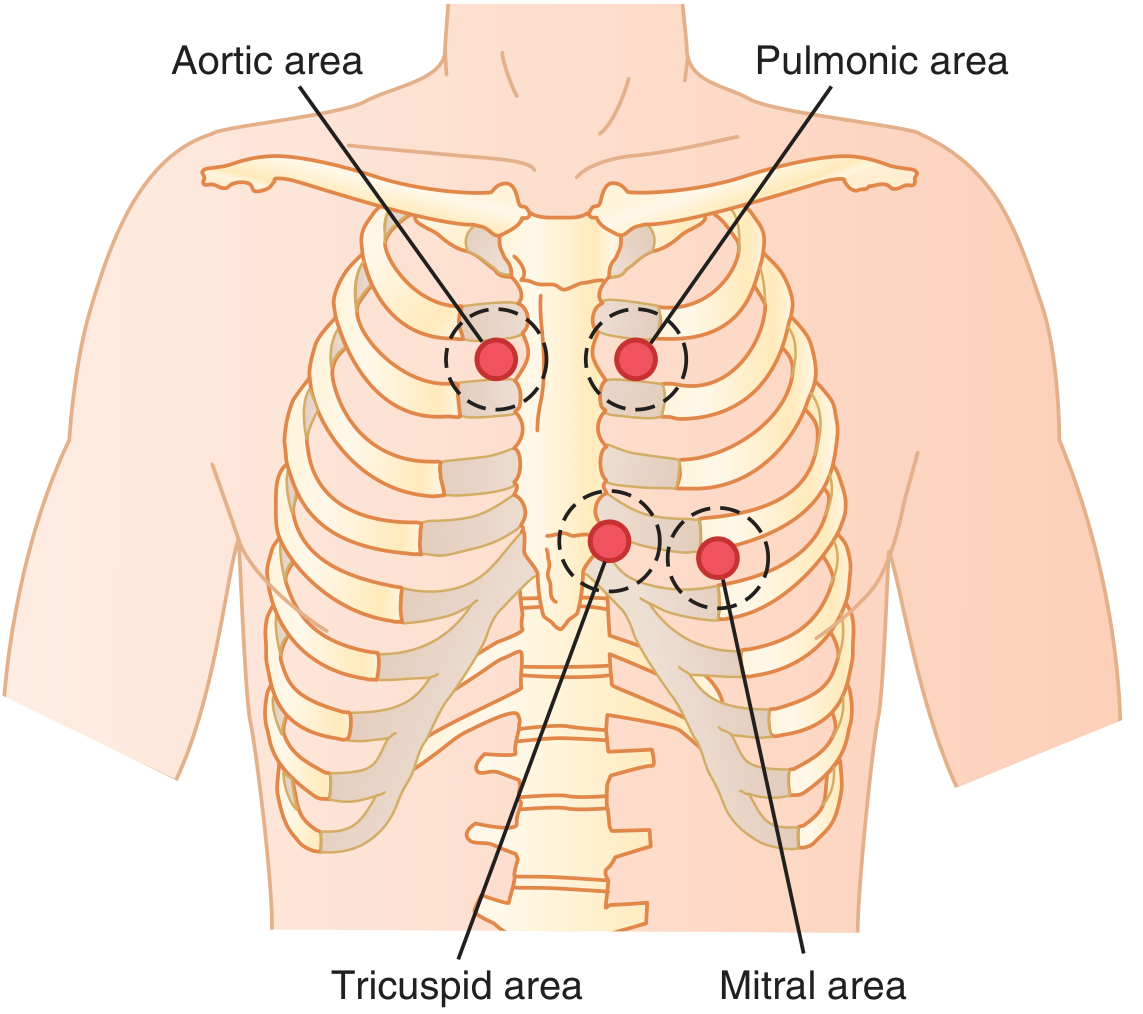
| Valve | Auscultation Area |
|---|---|
| Aortic | Right 2nd intercostal space, sternal border |
| Pulmonic | Left 2nd intercostal space, sternal border |
| Tricuspid | Left lower sternal border |
| Mitral | Cardiac apex (5th ICS, midclavicular line) |
Heart Murmurs
A murmur is an abnormal heart sound caused by turbulent blood flow through a valve or defect. Turbulence arises when:
- Blood flows through a narrowed (stenotic) opening at high velocity (nozzle effect).
- Blood flows backward (regurgitation) through an incompetent valve.
- Blood flows through an abnormal communication (e.g., VSD, PDA).
Grading (Levine Scale)
| Grade | Description |
|---|---|
| I | Faintest - can be heard only with difficulty |
| II | Faint but easily heard |
| III | Moderately loud, without a thrill |
| IV | Loud, with a palpable thrill |
| V | Very loud, still requires stethoscope (thrill present) |
| VI | Heard without a stethoscope |
The Major Valvular Murmurs - Mechanisms
Here are the phonocardiogram patterns of normal and abnormal heart sounds:
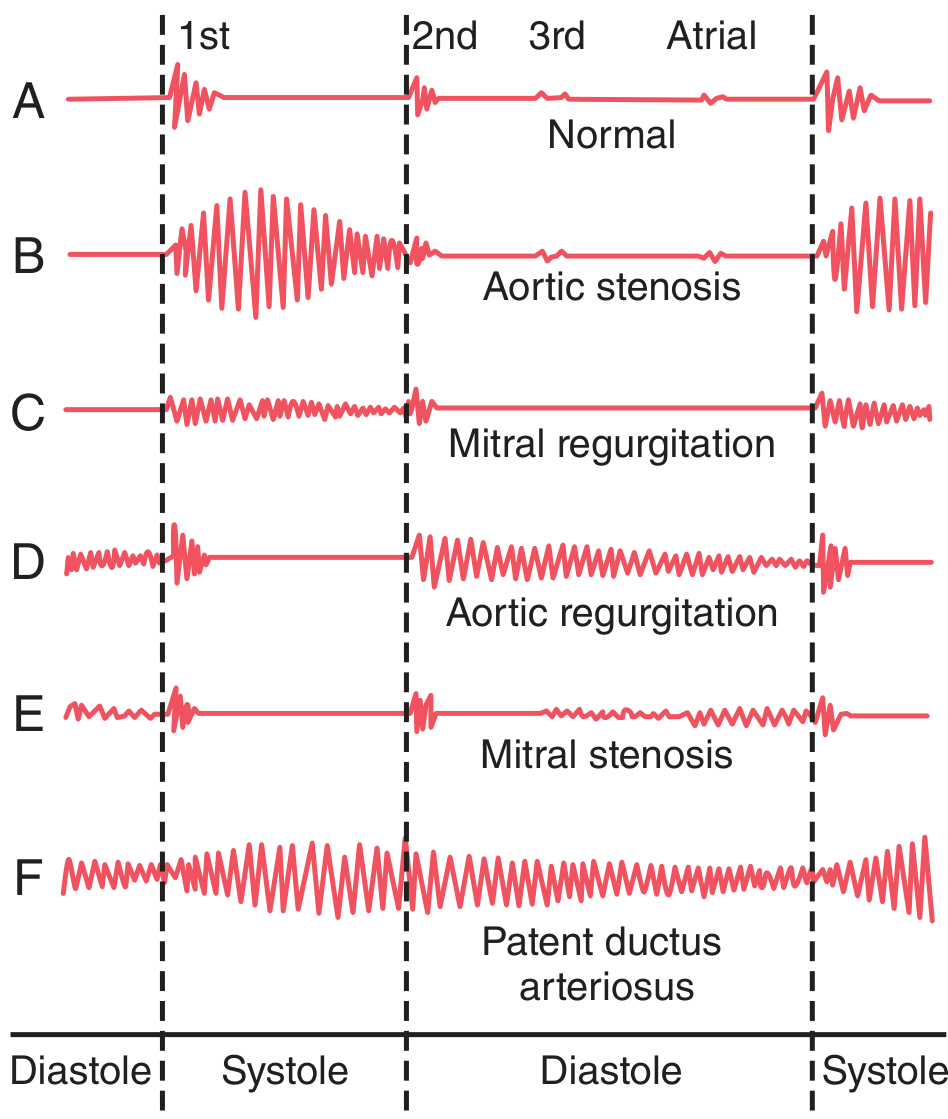
1. Aortic Stenosis - Systolic Ejection Murmur
Timing: Systole (S1 to S2)
Mechanism: The aortic valve opening is narrowed by fibrosis/calcification. Blood is forced through a tiny orifice at very high velocity (nozzle effect). Left ventricular pressure can rise up to 300 mmHg while aortic pressure stays normal. The high-velocity jet causes severe turbulence in the root of the aorta, which vibrates the aortic walls intensely.
Character: Harsh, crescendo-decrescendo (diamond-shaped) systolic murmur. Radiates to the neck/carotid arteries. A thrill may be palpable at the upper sternum. Associated with a delayed carotid upstroke and paradoxically split S2.
Common causes: Calcific degeneration (elderly), bicuspid aortic valve (younger patients, 50-60s), rheumatic heart disease.
2. Aortic Regurgitation - Diastolic Blowing Murmur
Timing: Diastole (S2 to S1)
Mechanism: The incompetent aortic valve allows blood to flow backward from the high-pressure aorta into the low-pressure left ventricle during diastole. The reverse jet turbulently enters a ventricle already holding diastolic blood, creating a high-frequency "blowing" sound.
Character: High-pitched, blowing, decrescendo diastolic murmur, heard best at the left sternal border with the patient leaning forward. Over time causes eccentric LV hypertrophy (dilated, enlarged LV).
Common causes: Rheumatic fever, infective endocarditis, aortic root dilation, bicuspid aortic valve, aortopathy (Marfan's syndrome).
3. Mitral Regurgitation - Systolic Blowing Murmur
Timing: Systole (S1 to S2) - holosystolic
Mechanism: The mitral valve fails to close properly during ventricular contraction, allowing blood to jet backward into the left atrium. The regurgitant jet causes turbulence with a high-frequency blowing/swishing quality. Because the left atrium is deep in the chest, the sound is transmitted primarily to the chest wall via the left ventricle toward the cardiac apex.
Character: High-pitched, blowing holosystolic murmur at the apex, radiating to the axilla.
Common causes: Rheumatic fever (leaflet scarring), mitral valve prolapse, heart failure with LV dilation (papillary muscle displacement), infective endocarditis, ruptured chordae tendineae.
In heart failure with reduced ejection fraction, as the LV dilates, the papillary muscles are pulled laterally, tethering the chordae and preventing full mitral leaflet coaptation - this mechanism produces functional mitral regurgitation even with structurally normal leaflets.
4. Mitral Stenosis - Diastolic Rumble
Timing: Diastole (after S2, opening snap, then rumble)
Mechanism: Rheumatic fever fuses the mitral leaflet edges, producing a narrow opening. Blood must pass with difficulty from the left atrium into the left ventricle. The left atrial pressure rarely rises above 30 mmHg, so the pressure gradient is small - there is little driving force compared to aortic stenosis. Consequently, this murmur is weak and of very low frequency, often below the audible threshold.
Character: Low-pitched, rumbling diastolic murmur, best heard at the apex with the bell of the stethoscope. Preceded by an opening snap (OS) - the snap of the stenotic but mobile leaflet snapping open. No murmur may be heard in early diastole; the rumble typically starts in the middle third of diastole once sufficient blood has accumulated to create reverberations.
Common causes: Virtually always rheumatic heart disease.
5. Right Heart Valve Murmurs (Pulmonary/Tricuspid)
Pulmonic and tricuspid stenosis/regurgitation produce murmurs similar in timing and quality to their left-sided counterparts, but with one key distinguishing feature: right heart murmurs increase in intensity on inspiration (Carvallo's sign) due to increased venous return to the right heart during inspiration.
6. Patent Ductus Arteriosus - Machinery Murmur
Timing: Continuous (both systole and diastole)
Mechanism: The ductus arteriosus fails to close after birth. Aortic pressure (high) continuously exceeds pulmonary arterial pressure, so blood shunts left-to-right through the ductus throughout the cardiac cycle. The shunt is greatest in systole (when aortic pressure is highest) and diminishes in diastole, creating a murmur that waxes and wanes like machinery.
Character: Harsh, continuous "machinery murmur" heard in the pulmonary area. It is one of the few truly continuous murmurs (spanning both S1 and S2).
Summary Table
| Valve Lesion | Timing | Character | Best Heard | Radiation |
|---|---|---|---|---|
| Aortic stenosis | Systolic (ejection) | Harsh, crescendo-decrescendo | Right 2nd ICS | Carotids, neck |
| Aortic regurgitation | Diastolic (decrescendo) | High-pitched blowing | Left sternal border | - |
| Mitral regurgitation | Holosystolic | High-pitched blowing | Apex | Axilla |
| Mitral stenosis | Mid-diastolic rumble | Low, rumbling | Apex (bell) | - |
| Tricuspid/Pulmonic lesions | Same as L-sided | Similar quality | Lower left sternal border | Increases with inspiration |
| PDA | Continuous | Machinery | Pulmonic area | - |
The Underlying Cause of Rheumatic Valvular Disease
The most common cause of acquired valve disease globally is rheumatic fever, an autoimmune reaction following group A beta-hemolytic streptococcal infection. The streptococcus releases proteins against which the body produces antibodies that cross-react with heart valve proteins (molecular mimicry). This triggers chronic immune-mediated valve damage:
- Stenosis occurs when leaflet edges fuse (scar tissue adheres adjacent leaflets).
- Regurgitation occurs when leaflet edges are so destroyed by scar tissue that they can no longer close.
- The mitral valve is most commonly affected (highest pressure stress), followed by the aortic valve. Right heart valves are less commonly involved due to lower pressure loads.
Sources: Guyton and Hall Textbook of Medical Physiology, pp. 289-292; Miller's Anesthesia 10e, p. 3907-3908
This is a shared conversation. Sign in to Orris to start your own chat.