Liver and gall-bladder disorders in children. (Biliary dyskinesia. Definition, causes, classification, clinical signs and management. Jaundice, definition, causes, types, clinical signs and management. Portal hypertension, causes, clinical signs, complications and management. Interpretation of results of liver function tests (LFTs) (AST, ALT, bilirubin and alkaline phosphate levels) Ultrasound examination of the gallbladder to determine its function. Skin color (jaundice, pallor). Palpation of labdomen in children. Percussion of the borders of the liver and measurement of its size according to Kurlov. Determination of pathologic signs by percussion (Ortner-Grekov’s sign, Mendel's sign). Long notes extra topics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Here is a comprehensive, structured overview of all the topics you requested.
Liver and Gallbladder Disorders in Children
1. Biliary Dyskinesia
Definition
Biliary dyskinesia is a functional disorder of the biliary tree, generally defined by gallbladder dysmotility — a malfunction in the normal motility response that leads to symptoms of biliary colic without cholelithiasis. It is a diagnosis of exclusion. — Sabiston Textbook of Surgery, p. 1835
Causes
- Abnormal gallbladder contractile response to cholecystokinin (CCK)
- Associated functional GI disorders: delayed colonic transit, delayed gastric emptying
- Possible autonomic dysregulation or hormonal imbalance
- Often co-exists with irritable bowel syndrome or functional dyspepsia
Classification
| Type | Description |
|---|---|
| Hypomotor (hypokinetic) | Reduced gallbladder emptying; ejection fraction < 35% on CCK-HIDA scan |
| Hypermotor (hyperkinetic) | Excessive gallbladder contraction causing colic-like pain |
Clinical Signs
- Right upper quadrant or epigastric pain (biliary colic) — often episodic, postprandial
- Nausea, vomiting, oral intolerance
- No fever or jaundice (distinguishes from cholecystitis)
- No stones or sludge on ultrasound
- A confounding factor: patients often have other functional GI disorders
Diagnosis
- Ultrasound: no stones/sludge — required to exclude organic causes
- CCK-stimulated HIDA scan (cholescintigraphy): ejection fraction < ~35% is diagnostic of hypomotor biliary dyskinesia
- Rome IV criteria help exclude GERD, IBS, and other functional causes
- CT, endoscopy used to rule out other diagnoses
Management
- Cholecystectomy: effective in >85% of patients, especially those with classic biliary colic and reduced ejection fraction
- In non-responders or atypical cases: ERCP with sphincterotomy
- Medical options: dietary fat restriction, antispasmodics, prokinetics
- Patients with nausea as the primary symptom respond less well to cholecystectomy
2. Jaundice
Definition
Jaundice (icterus) is the yellow discoloration of skin, sclerae, and mucous membranes caused by elevated serum bilirubin (hyperbilirubinemia). It becomes clinically visible when serum bilirubin exceeds ~35 µmol/L (2 mg/dL).
Bilirubin Metabolism (basis for classification)
- Unconjugated (indirect) bilirubin: fat-soluble, albumin-bound, produced from RBC breakdown
- Hepatocytes conjugate bilirubin with glucuronic acid → water-soluble conjugated (direct) bilirubin → excreted in bile
Causes and Types
Pre-hepatic (Hemolytic) Jaundice
- Excess RBC breakdown overwhelms hepatic conjugation capacity
- Causes: hemolytic anemia (hereditary spherocytosis, G6PD deficiency, sickle cell disease), incompatible blood transfusion, neonatal hemolysis (Rh/ABO incompatibility)
- Bilirubin: predominantly unconjugated ↑
- Urine: normal color (no bilirubin); urobilinogen ↑
- Stools: dark (excess urobilinogen)
Hepatic (Hepatocellular) Jaundice
- Impaired uptake, conjugation, or excretion of bilirubin by damaged hepatocytes
- Causes: viral hepatitis (A, B, C, E), autoimmune hepatitis, toxic/drug-induced hepatitis, Wilson's disease, metabolic disorders (galactosemia, tyrosinemia), cirrhosis
- Bilirubin: both conjugated and unconjugated ↑ (mixed)
- AST/ALT: markedly elevated
- Urine: dark (bilirubin); urobilinogen variable
Post-hepatic (Obstructive/Cholestatic) Jaundice
- Obstruction of bile flow from hepatocytes to duodenum
- Causes in children: biliary atresia, choledochal cyst, cholelithiasis, primary sclerosing cholangitis, pancreatic mass, bile duct stricture
- Bilirubin: predominantly conjugated ↑
- ALP and GGT markedly elevated
- Urine: dark (bilirubinuria); stools: pale/clay-colored (acholic)
Neonatal Physiological Jaundice
- Appears day 2–4 of life, resolves by day 10–14; unconjugated
- Due to high RBC turnover + immature hepatic conjugation
- Pathological if: appears < 24 h, bilirubin rises rapidly, conjugated bilirubin ↑, persists > 2 weeks
Clinical Signs
- Yellow discoloration: sclerae (earliest), skin (face → trunk → extremities), mucous membranes
- Pre-hepatic: mild jaundice, pallor (anemia), splenomegaly
- Hepatic: fatigue, anorexia, hepatomegaly, tender liver, dark urine, possible fever
- Obstructive: deep yellow-green jaundice, pruritus, pale stools, dark urine, no fever (unless cholangitis)
Management
| Type | Management |
|---|---|
| Pre-hepatic | Treat underlying hemolysis; phototherapy/exchange transfusion in neonates |
| Hepatic | Treat underlying cause (antivirals for hepatitis B/C, immunosuppression for AIH, chelation for Wilson's); supportive care |
| Obstructive | Surgical/endoscopic relief of obstruction (Kasai portoenterostomy for biliary atresia; ERCP/stenting; cholecystectomy); ursodeoxycholic acid for cholestasis |
3. Portal Hypertension
Definition
Portal hypertension is defined as portal venous pressure > 12 mmHg (normal: 5–10 mmHg). It results from increased resistance to portal blood flow and/or increased portal blood flow.
Causes — Classified by Level of Obstruction
— Robbins Pathologic Basis of Disease, p. 770
| Level | Causes |
|---|---|
| Pre-hepatic | Portal vein thrombosis, portal vein narrowing/atresia, massive splenomegaly with ↑ splenic flow |
| Intrahepatic | Cirrhosis (most common overall), schistosomiasis, nodular regenerative hyperplasia, primary biliary cholangitis, sarcoidosis, fatty liver, amyloidosis, infiltrative malignancy |
| Post-hepatic | Right-sided heart failure, constrictive pericarditis, Budd-Chiari syndrome (hepatic vein outflow obstruction) |
In children specifically, the most common causes are: extrahepatic portal vein obstruction (EHPVO)/portal vein thrombosis (pre-hepatic, most common in children), biliary atresia with cirrhosis (intrahepatic), and cystic fibrosis-related liver disease.
Pathophysiology
Two mechanisms combine:
- Increased resistance at the sinusoidal level — from fibrosis, parenchymal nodules, myofibroblast contraction, ↓ NO production, ↑ endothelin-1
- Increased portal venous inflow — splanchnic arterial vasodilation (mediated by NO, prostacyclin, TNF-α) → increased venous efflux into the portal system
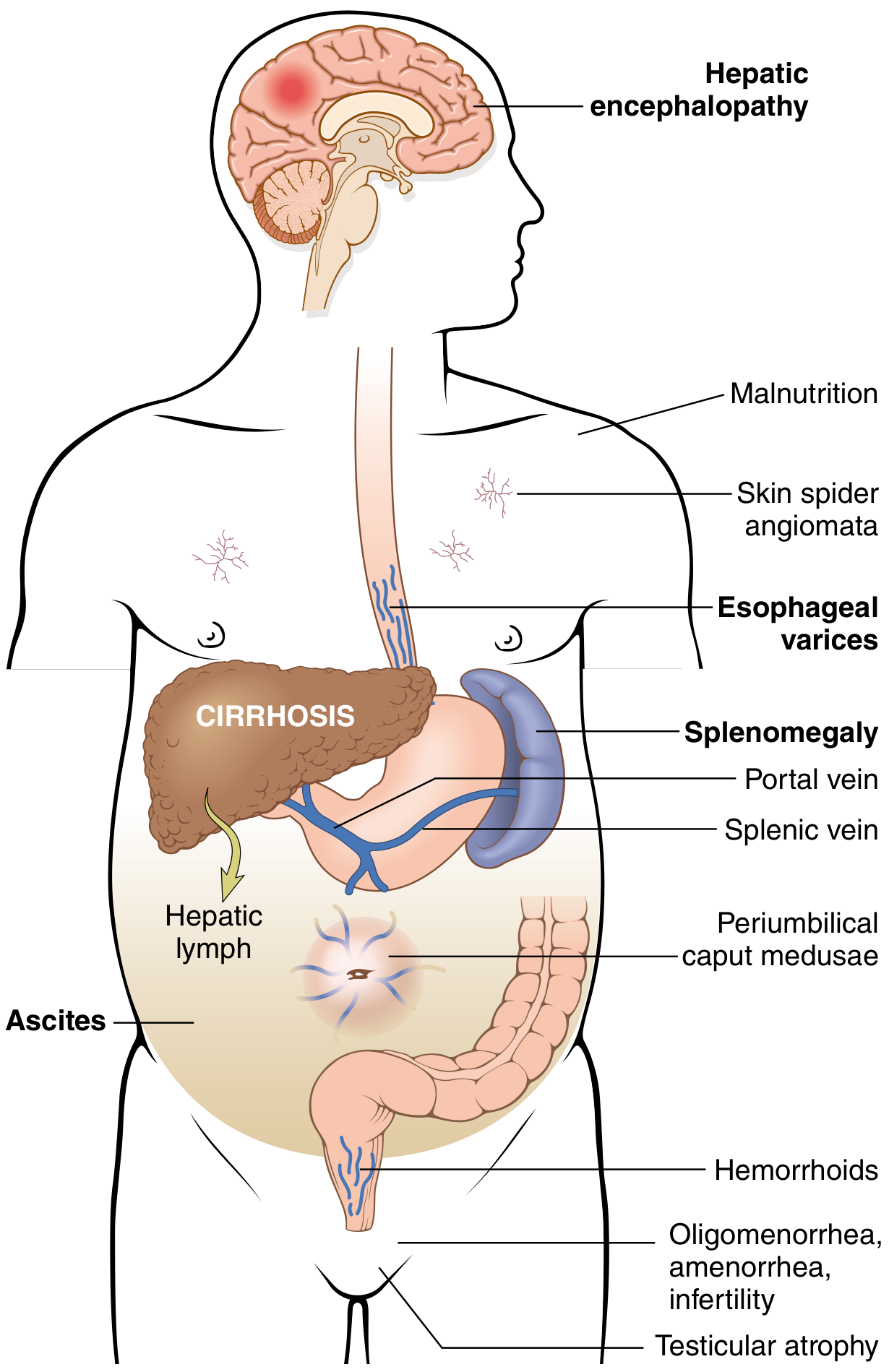
Clinical Signs
- Splenomegaly (most prominent sign in children with pre-hepatic PH)
- Ascites
- Caput medusae (dilated periumbilical veins)
- Hematemesis (esophageal/gastric variceal bleeding)
- Rectal bleeding (hemorrhoids/rectal varices)
- Signs of hypersplenism: thrombocytopenia, leukopenia, anemia
Complications
Four major consequences (Robbins):
- Esophagogastric varices → massive hematemesis; ~40% of patients with advanced cirrhosis; ~30% mortality per bleeding episode
- Ascites → occurs when ≥500 mL accumulates; can lead to spontaneous bacterial peritonitis, hepatorenal syndrome, hepatic hydrothorax
- Portosystemic encephalopathy → impaired ammonia clearance; behavioral changes, confusion, coma
- Congestive splenomegaly → hypersplenism (thrombocytopenia, pancytopenia)
Pulmonary complications:
- Hepatopulmonary syndrome: intrapulmonary vascular dilation → hypoxemia (worse when upright — platypnea/orthodeoxia)
- Portopulmonary hypertension: pulmonary arterial hypertension in the setting of PH
Management
| Problem | Management |
|---|---|
| Variceal bleeding (acute) | IV terlipressin/octreotide (splanchnic vasoconstriction); endoscopic variceal ligation (EVL) or sclerotherapy; Sengstaken-Blakemore tube if uncontrolled; TIPS (transjugular intrahepatic portosystemic shunt) |
| Variceal bleeding (prophylaxis) | Non-selective beta-blockers (propranolol/nadolol); EVL for high-risk varices |
| Ascites | Salt restriction; diuretics (spironolactone ± furosemide); large-volume paracentesis with albumin; TIPS |
| Encephalopathy | Lactulose; rifaximin; dietary protein management |
| Surgical | Portosystemic shunts (Rex shunt preferred in children with EHPVO — mesenterico-left portal bypass); liver transplantation for end-stage disease |
4. Interpretation of Liver Function Tests (LFTs)
— Tietz Textbook of Laboratory Medicine, 7th Ed.
Pattern Recognition Principle
"Patterns of liver test abnormalities denote the predominant type of liver injury."
| Test | What It Reflects | Normal (approximate) | Interpretation |
|---|---|---|---|
| AST (aspartate aminotransferase) | Hepatocellular injury (also cardiac/muscle) | < 40 U/L | Elevated in hepatitis, cirrhosis, ischemic hepatitis, muscle disease; less liver-specific than ALT |
| ALT (alanine aminotransferase) | Hepatocellular injury (liver-specific) | < 35–40 U/L | Elevated primarily in liver parenchymal disease; hallmark of hepatitis |
| Bilirubin (total/direct/indirect) | Cholestasis, hemolysis, hepatocellular dysfunction | Total < 17 µmol/L (1 mg/dL) | ↑ Unconjugated → hemolysis or impaired uptake/conjugation; ↑ Conjugated → intrahepatic or extrahepatic cholestasis |
| ALP (alkaline phosphatase) | Biliary tree injury, cholestasis | Age-dependent (higher in children during growth!) | Predominantly elevated in bile duct injury, cholestasis, cholangitis; must interpret in context of GGT |
| GGT | Biliary/cholestatic (also alcohol) | < 50 U/L | Confirms biliary origin of ↑ ALP; elevated in alcohol use |
| Albumin | Hepatic synthetic function | 35–50 g/L | Low in chronic liver disease = impaired synthesis |
| PT/INR | Hepatic synthetic function (clotting factors) | INR ≈ 1.0 | Prolonged in acute or chronic liver failure; vitamin K–responsive if cholestasis is the cause |
Diagnostic Patterns
| Pattern | Likely Diagnosis |
|---|---|
| AST/ALT ↑↑↑ >> ALP | Acute hepatocellular injury (viral hepatitis, toxic, ischemic) |
| ALP ↑↑ + GGT ↑↑ + conjugated bilirubin ↑ | Cholestasis / biliary obstruction |
| Both AST/ALT and ALP ↑ moderately | Mixed hepatocellular + cholestatic (e.g., primary biliary cholangitis, drug-induced) |
| AST/ALT ratio > 2:1 | Alcoholic hepatitis (De Ritis ratio) |
| Bilirubin ↑ + normal AST/ALT + normal ALP | Isolated hyperbilirubinemia → hemolysis or Gilbert's syndrome |
| Low albumin + prolonged INR | Chronic liver failure (poor synthetic function) |
Pediatric note: ALP is physiologically elevated in children and adolescents due to bone isoenzyme during periods of growth — always interpret with age-specific reference ranges and confirm biliary origin with GGT.
5. Ultrasound Examination of the Gallbladder (Functional Assessment)
Ultrasound is the first-line imaging modality for gallbladder assessment.
Morphological Assessment
- Wall thickness (normal < 3 mm)
- Size: normal gallbladder in children — length 3–7 cm, width 1–3 cm
- Presence of stones, sludge, polyps
- Pericholecystic fluid (sign of cholecystitis)
Functional Assessment (Dynamic / Contraction Study)
Used to assess gallbladder contractility (relevant in biliary dyskinesia):
- Fasting scan: baseline gallbladder volume measured (child fasts 4–6 hours)
- Fatty meal provocation: child given a fatty meal or CCK injection
- Post-prandial scan: gallbladder volume re-measured at 30 and 60 minutes
- Ejection fraction = (Fasting volume − Residual volume) / Fasting volume × 100%
Normal ejection fraction ≥ 35–40%
- EF < 35% → hypokinetic biliary dyskinesia (impaired emptying)
- EF > 75–80% → hyperkinetic dyskinesia
Note: CCK-HIDA scan (cholescintigraphy) is the gold standard for ejection fraction measurement, but dynamic ultrasound is used as a simpler, radiation-free alternative particularly in children.
6. Skin Color Assessment
Jaundice
- Assessment: examine in natural (daylight) lighting
- Earliest sign: yellow discoloration of the sclerae (visible at bilirubin ~34 µmol/L)
- Then: skin of face, trunk, palms/soles (deepest jaundice)
- Color nuances:
- Lemon-yellow: hemolytic jaundice (pre-hepatic)
- Bright orange-yellow: hepatocellular jaundice
- Yellow-green / olive green: obstructive/cholestatic jaundice (prolonged)
- Check oral mucosa, hard palate (especially in dark-skinned children)
Pallor
- Indicates anemia — relevant in hemolytic jaundice
- Assess: conjunctival pallor (most reliable), palmar creases, nail beds, oral mucosa
- In children: conjunctival pallor is the most sensitive site
- Associated with pre-hepatic jaundice, hypersplenism-related anemia (in portal hypertension), or blood loss from varices
7. Palpation of the Abdomen in Children
General Principles
- Child should be supine, relaxed, knees slightly flexed; warm hands
- Younger children: distract with conversation or have parent present; infants may be examined on parent's lap
- Begin with light palpation (to assess tenderness, guarding, superficial masses), then deep palpation
Liver Palpation
- Technique: start from the right iliac fossa, moving upward toward the right costal margin, synchronizing with breathing (feel the liver edge descend on inspiration)
- Normal findings in children:
- Neonates/infants: liver edge palpable 1–2 cm below right costal margin (normal)
- Children < 4 years: up to 2 cm below right costal margin
- Older children/adolescents: normally not palpable or just at costal margin
- Characterize the liver edge: sharp vs. rounded; smooth vs. nodular; tender vs. non-tender; soft vs. firm/hard
Spleen Palpation
- Start from right iliac fossa toward left costal margin (spleen enlarges toward right iliac fossa)
- Splenomegaly: a key sign of portal hypertension in children
Gallbladder Palpation
- Murphy's sign: deep inspiration while examiner presses under right costal margin in mid-clavicular line → sudden arrest of inspiration due to pain = positive (cholecystitis)
- In children: less sensitive; gallbladder rarely palpable unless hydrops or empyema
8. Percussion of Liver Borders — Kurlov's Method
Kurlov's method is a standardized percussion technique for determining liver size.
Technique
Three measurements are taken in the right mid-clavicular line, midline (xiphoid line), and left costal arch line:
| Dimension | Line | Upper Border | Lower Border |
|---|---|---|---|
| 1st size | Right mid-clavicular line | Determined by percussion (dullness begins) | Dullness ends (transition to tympany) |
| 2nd size | Midline (xiphoid–umbilicus) | Same upper border as 1st (horizontal projection) | Lower border of liver dullness in midline |
| 3rd size | Left costal arch | From 2nd midline lower border | To end of liver dullness along left costal arch |
Normal Liver Size by Kurlov (in adults):
- 1st size: 9 ± 1 cm
- 2nd size: 8 ± 1 cm
- 3rd size: 7 ± 1 cm (written as 9–8–7 cm)
In children, values are age-dependent and smaller:
| Age | 1st size | 2nd size | 3rd size |
|---|---|---|---|
| < 1 year | 5–6 cm | 4–5 cm | 3–4 cm |
| 1–3 years | 6–7 cm | 5–6 cm | 4–5 cm |
| 3–7 years | 7–8 cm | 6–7 cm | 5–6 cm |
| 7–12 years | 8–9 cm | 7–8 cm | 6–7 cm |
| > 12 years | 9 ± 1 cm | 8 ± 1 cm | 7 ± 1 cm |
Hepatomegaly = any measurement exceeding the upper age-appropriate limit.
9. Pathological Percussion Signs
Ortner-Grekov's Sign (Ortner's Sign)
- Technique: the examiner percusses (taps) the right costal arch with the ulnar edge of the right hand, or taps the medial edge of the right hand placed over the right costal arch
- Positive: pain elicited by this percussion
- Significance: indicates inflammation of the gallbladder or bile ducts — positive in:
- Acute cholecystitis
- Cholelithiasis
- Biliary dyskinesia (sometimes)
- Cholangitis
- Reflects tenderness of the gallbladder/biliary tree through the overlying ribs
Mendel's Sign (Mendel's Abdominal Percussion Sign)
- Technique: the examiner percusses or taps the anterior abdominal wall with a finger (like tapping) in the right hypochondrium (over the gallbladder projection) and epigastrium
- Positive: pain elicited by percussion (unlike deep palpation, uses percussion stimulus)
- Significance: indicates local peritoneal irritation over the gallbladder/bile ducts; positive in:
- Acute cholecystitis
- Peritoneal involvement in biliary disease
- Duodenal ulcer with local peritonitis (also described here)
- More sensitive for detecting localized tenderness than palpation in tense abdominal muscles
Comparison: Both signs detect biliary/hepatic tenderness. Ortner's targets the costal arch (indirect percussion); Mendel's targets the abdominal wall directly over the organ. Both are more relevant in the context of acute/inflammatory biliary disease.
Summary Table: Key Differentials in Pediatric Jaundice by LFT Pattern
| Finding | Pre-hepatic | Hepatocellular | Cholestatic/Obstructive |
|---|---|---|---|
| Bilirubin | Unconjugated ↑ | Both ↑ | Conjugated ↑ |
| AST/ALT | Normal | ↑↑↑ | Normal or ↑ |
| ALP | Normal | ↑ or normal | ↑↑↑ |
| GGT | Normal | ↑ | ↑↑↑ |
| Urine color | Normal | Dark | Dark |
| Stool color | Dark | Normal/pale | Pale/clay |
| Albumin/PT | Normal | Abnormal (acute failure) | Normal (early) |
Key References:
- Sabiston Textbook of Surgery, 21st Ed. — Biliary Dyskinesia, p. 1835
- Robbins & Cotran Pathologic Basis of Disease — Portal Hypertension, p. 770–771
- Tietz Textbook of Laboratory Medicine, 7th Ed. — Liver Function Test Abnormalities, p. 2022
This is a shared conversation. Sign in to Orris to start your own chat.