I now have comprehensive material from multiple standard textbooks (Campbell-Walsh Urology, Bailey & Love, Hinman's Atlas, The Developing Human, Schwartz's Surgery) plus clinical images. Let me now compile the complete, exam-focused answer:
🔬 HYPOSPADIAS - Complete Exam Guide for Plastic Surgery
Sources: Campbell-Walsh Urology (5th Ed), Bailey & Love's Surgery (28th Ed), Hinman's Atlas of Urologic Surgery, The Developing Human (Moore & Persaud), Schwartz's Principles of Surgery
1. DEMOGRAPHY & EPIDEMIOLOGY
| Parameter | Fact |
|---|
| Incidence | 1 in 125-300 male live births |
| Most common congenital abnormality | Of the urethra (MOST COMMON) |
| Most common type | Glanular hypospadias |
| Distal types | Account for ~70% of all cases |
| Glanular + Penile | ~80% of all cases together |
| Least common / most severe | Perineal hypospadias |
| Perineal type | Only 1% - associated with bifid scrotum + ambiguous genitalia |
| Familial risk | Father affected → 8% risk in son; sibling affected → 14% risk |
| Trend | Incidence increasing in developed countries (possible endocrine disruptor link) |
Exam crux: Hypospadias is the MOST COMMON congenital urethral anomaly. Glanular type = MOST COMMON. Perineal = LEAST COMMON but MOST SEVERE.
2. EMBRYOLOGY & PATHOGENESIS
Normal urethral development:
- Urethral folds fuse in the midline (ventral) under androgen stimulation between weeks 8-16 of gestation
- The spongy (penile) urethra forms by fusion of urethral folds
- The glanular urethra forms separately by canalization of the ectodermal cord
- Complete development depends on testosterone and its conversion to DHT (5-alpha reductase)
What goes wrong in hypospadias:
- Failure of canalization of the ectodermal cord in the glans (→ glanular hypospadias)
- Failure of fusion of the urethral folds (→ penile/proximal hypospadias)
- Both mechanisms together → complete ventral hypoplasia with chordee
(The Developing Human, Moore & Persaud)
3. ETIOLOGY
Genetic Factors
- Polygenic/multifactorial inheritance pattern
- Associated genes: SRD5A2 (5-alpha reductase 2), AR (androgen receptor), ATF3, MAMLD1, FGF8, FGF10, BMP7, MID1, CXorf6
- Monozygotic twins: 18% concordance (not 100% → environmental component)
- Family history present in ~7-10% of cases
Hormonal/Endocrine Factors
- Inadequate androgen production by fetal testes
- Inadequate androgen receptor sensitivity (partial androgen insensitivity)
- 5-alpha reductase deficiency → inability to convert T → DHT
- Maternal progestagen/estrogen exposure during pregnancy
Environmental Factors (Endocrine Disruptors)
- Pesticides (DDT, DDE, vinclozolin) - anti-androgenic
- Phthalates (plastics industry)
- Phytoestrogens (soy-based foods)
- Maternal obesity, preeclampsia, placental insufficiency
- ART (Assisted Reproductive Techniques) - doubles the risk
- Low birth weight / prematurity
Associated Conditions (exam favourite!)
| Condition | Association |
|---|
| Cryptorchidism | 9% of hypospadias cases |
| Inguinal hernia | 9% of cases |
| Disorders of Sex Development (DSD) | Severe hypospadias + cryptorchidism = investigate for DSD |
| CAH | Perineal hypospadias in virilized females |
EXAM KEY: If perineal hypospadias + bilateral cryptorchidism + micropenis → ALWAYS investigate for DSD/intersex
4. CLINICAL FEATURES - THE TRIAD
All three features are pathognomonic:
| Feature | Description |
|---|
| 1. Ectopic meatus | Ventrally placed urethral meatus, proximal to normal position |
| 2. Ventral chordee | Ventral penile curvature due to fibrous tissue replacing spongiosum |
| 3. Dorsal hood / incomplete prepuce | Foreskin present dorsally but absent ventrally (hooded foreskin) |
Note: In mild distal cases, chordee may be absent. The meatus + hooded foreskin may be the only findings.
Additional Features
- Incomplete foreskin (dorsal hood)
- Bifid scrotum (severe cases)
- Penoscrotal transposition (severe cases)
- Urethral dimple / blind pit at normal meatal site
- Downward deflection of urinary stream
- Spraying of urine (40-50%)
- Post-void dribbling (20-40%)
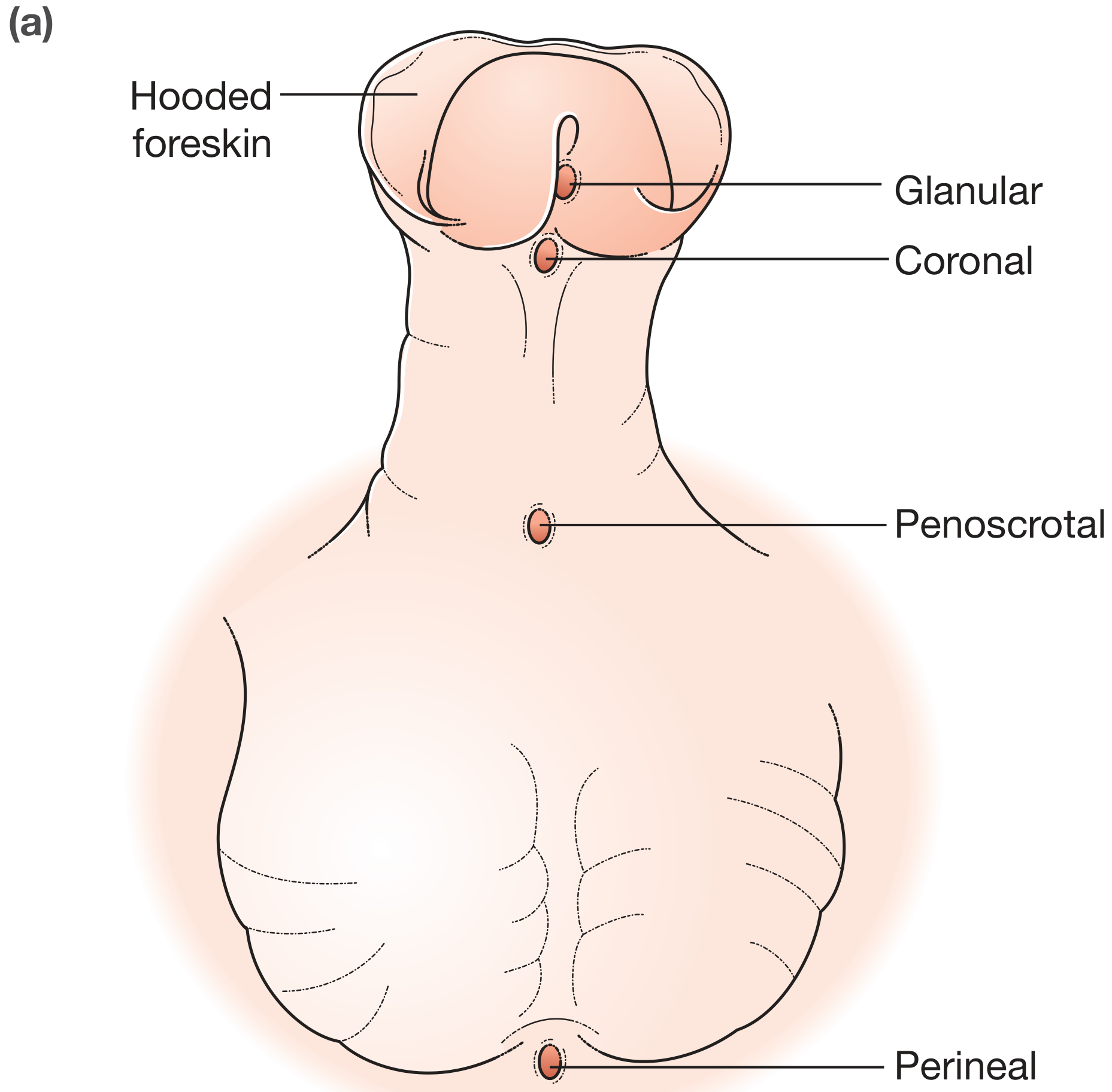
5. CLASSIFICATION
Anatomical / By Meatal Position (Most Used)
Fig: Hypospadias classification diagram (Bailey & Love, 28th Ed)
| Type | Meatal Position | Frequency |
|---|
| Glanular | On glans, proximal to normal site | Most common |
| Coronal | At coronal sulcus | Common |
| Penile (Mid-shaft) | Under penile shaft | Moderate |
| Penoscrotal | At penoscrotal junction | Less common |
| Scrotal | On scrotum (bifid scrotum) | Rare |
| Perineal | Between scrotal halves | Least common |
Simplified Clinical Classification
| Group | Types Included | Surgery |
|---|
| Anterior (Distal) ~70% | Glanular, Coronal, Distal penile | Often single-stage |
| Middle ~10% | Mid-shaft penile | Single-stage possible |
| Posterior (Proximal) ~20% | Penoscrotal, Scrotal, Perineal | Often two-stage |
Barcat Classification (for severity)
| Grade | Position |
|---|
| Grade I | Glanular / Coronal |
| Grade II | Distal penile / Mid-penile |
| Grade III | Proximal penile / Penoscrotal |
| Grade IV | Scrotal / Perineal |
6. CLINICAL PHOTOGRAPHS
Perineal hypospadias - severe type:
Fig: Perineal/severe hypospadias with chordee and bifid scrotum (Bailey & Love)
Glanular hypospadias in infant (arrow = meatal opening):
Fig: Glanular hypospadias - meatus on ventral surface of glans (The Developing Human)
Urethrocutaneous fistula (most common complication):
Fig: Urethrocutaneous fistula after failed hypospadias repair (Bailey & Love)
7. INVESTIGATIONS
When to Investigate?
For ROUTINE / DISTAL hypospadias:
- Diagnosis is purely clinical - NO investigations needed routinely
- Physical examination is sufficient
INVESTIGATE when:
| Indication | Investigation | Rationale |
|---|
| Severe hypospadias (penoscrotal/perineal) | Karyotype (chromosomal analysis) | Rule out DSD |
| Perineal hypospadias + bilateral cryptorchidism | Karyotype + pelvic USS | Rule out 46,XX CAH or gonadal dysgenesis |
| Micropenis + severe hypospadias | LH, FSH, testosterone, DHT, 17-OH progesterone | Endocrine workup |
| Any suspicion of DSD | FISH for SRY, estrogen, androgens | Intersex evaluation |
| Recurrent UTI / poor stream | MCUG (voiding cystourethrogram) | Rule out reflux / stricture |
| Pre-operative workup (proximal cases) | RGU (retrograde urethrogram) / MCUG | Assess urethral anatomy |
| Post-operative evaluation | Uroflowmetry | Assess voiding function |
| Failed repair / fistula | RGU + MCU | Assess recurrence, stricture |
Specific Investigations Table
| Investigation | Finding in Hypospadias | When to Do |
|---|
| Clinical Exam | Ventral meatus + hooded foreskin + chordee | ALWAYS first |
| Karyotype | 46,XX → DSD; 46,XY → confirmed male | Perineal/scrotal type |
| Serum 17-OHP | Elevated in CAH | Ambiguous genitalia |
| Testosterone + DHT ratio | >20:1 ratio → 5-alpha reductase deficiency | Small phallus + hypospadias |
| Pelvic USS | Mullerian structures (uterus?) | DSD workup |
| RGU/MCU | Shows urethral anatomy, strictures | Pre/post-op in proximal cases |
| Uroflowmetry | Reduced flow, prolonged void | Post-operative follow-up |
| HCG stimulation test | Assess testosterone response | Micropenis / undescended testes |
When NOT to Investigate
- Distal glanular or coronal hypospadias with no associated anomalies - no workup needed
- Isolated hypospadias without ambiguous genitalia or cryptorchidism - clinical diagnosis only
8. PREOPERATIVE CONSIDERATIONS
Key Rules Before Surgery
- NEVER CIRCUMCISE a child with hypospadias - preputial skin is the most valuable graft material
- Correct age: 6-18 months is the optimal window (before toilet training, penile development)
- Most surgeons prefer 6-12 months
- Anesthetic risk is acceptable after 6 months
- Magnification (2.5x-3.5x loupes or operating microscope) is mandatory
- Preoperative testosterone cream/DHT cream (topical) for 4-6 weeks may enlarge a small phallus
- Assess: meatal position, urethral plate quality, degree of chordee, foreskin amount
Hormonal Priming (Preoperative)
- Topical DHT or testosterone applied for 4-6 weeks pre-op
- Used for small phallus or in proximal cases
- Systemic HCG or testosterone for severe micropenis
- A 2024 systematic review (PMID 38739164) confirmed benefit of topical estrogen / hormone priming in hypospadias management
9. SURGICAL PRINCIPLES - GOALS OF REPAIR
The ideal repair achieves:
- Orthotopic meatus - vertical slit at tip of glans
- Straight penis - correction of chordee
- Normal voiding - forward, non-deflected stream
- Cosmetically normal appearance
- Normal sexual function in adulthood
- Low complication rate - fistula rate <5% is the benchmark
10. SURGICAL TECHNIQUES
OVERVIEW: Which technique for which type?
| Type of Hypospadias | Preferred Repair |
|---|
| Glanular (meatal advancement possible) | MAGPI or Urethromeatoplasty |
| Coronal / Distal penile - good urethral plate | TIP (Snodgrass) - GOLD STANDARD |
| Distal - wide plate, no chordee | Thiersch-Duplay (Tubularization) |
| Distal - parameatal skin available | Mathieu (Flip-Flap) |
| Mid/proximal - intact urethral plate | TIP or Onlay Island Flap (OIF) |
| Proximal with chordee - needs plate division | Two-stage Bracka/Byars repair |
| Severe - inadequate local tissue | Buccal mucosa graft (staged) |
| Failed/redo cases | Buccal mucosa graft / staged repair |
A. MAGPI (Meatal Advancement and Glanuloplasty Incorporated)
Duckett, 1981
Indication: Glanular / subcoronal hypospadias with mobile meatus (can advance distally)
Steps:
- Transverse incision distal to meatus (Heineke-Mikulicz principle)
- Close transversely to advance meatus distally
- Dorsal skin bridge excised
- Glanular wings approximated to create conical glans
Contraindication: Meatus that cannot be easily advanced; narrow glans; any chordee
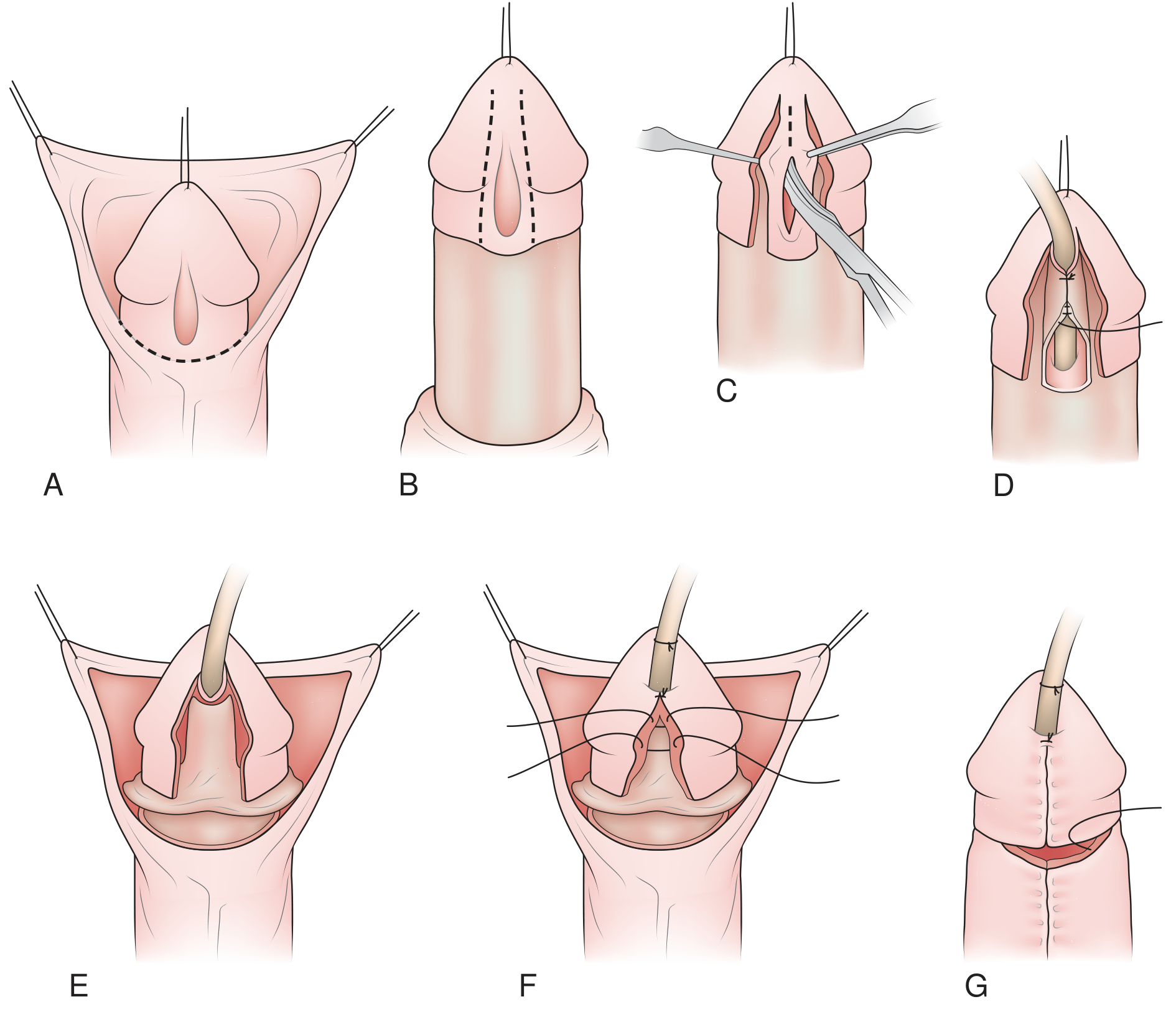
B. TIP REPAIR (Tubularized Incised Plate) - SNODGRASS
Snodgrass, 1994 - Current GOLD STANDARD
Indication: Distal to mid-penile hypospadias with a good urethral plate (90%+ of distal repairs)
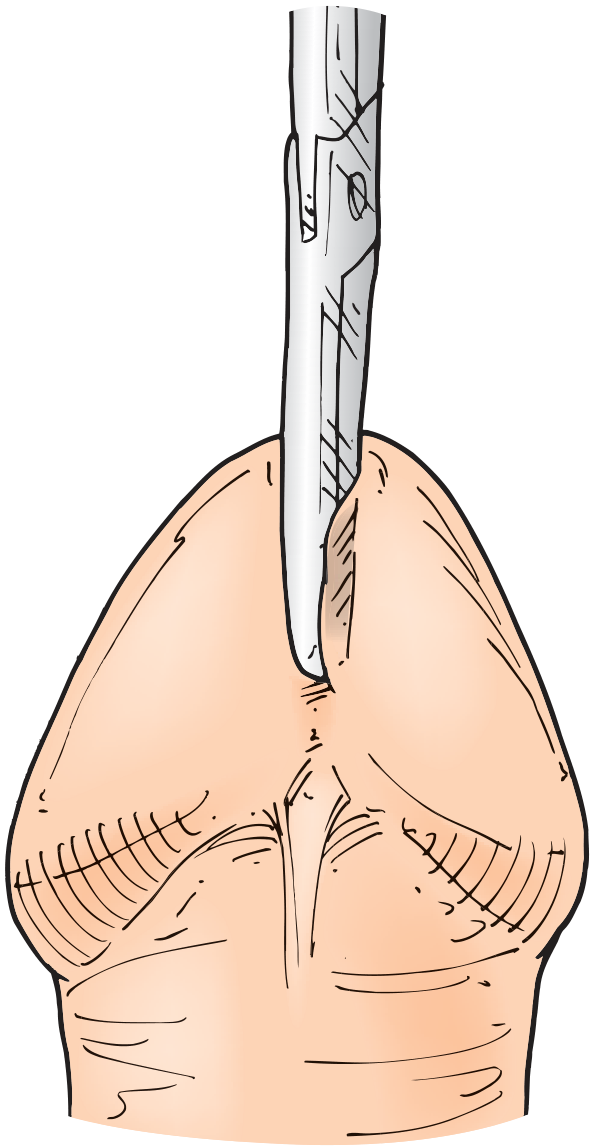
KEY PRINCIPLE: A midline incision in the urethral plate paradoxically WIDENS it (allows tubularization without tension)
Fig: Distal TIP repair steps A-G (Campbell-Walsh Urology)
Surgical Steps (Snodgrass TIP):
- A - Circumscribing skin incision around hypospadiac meatus, preserving urethral plate
- B - Penile degloving - skin retracted proximally, chordee assessed
- C - Deep midline incision of urethral plate to underlying corporal bodies (the KEY step - widens the plate)
- D - Tubularization - plate rolled into tube over catheter using 7-0 PDS running sutures; first stitch ~3mm proximal to meatal end (creates oval opening)
- E - Dartos flap cover - pedicled dartos/subcutaneous flap interposed between neourethra and skin (reduces fistula risk - WATERPROOFING LAYER)
- F - Glansplasty - glans wings approximated over neourethra creating neo-meatus at tip
- G - Skin closure + circumcision or preputioplasty
Fig: Midline incision into the urethral plate - the defining step of TIP repair (Hinman's Atlas)
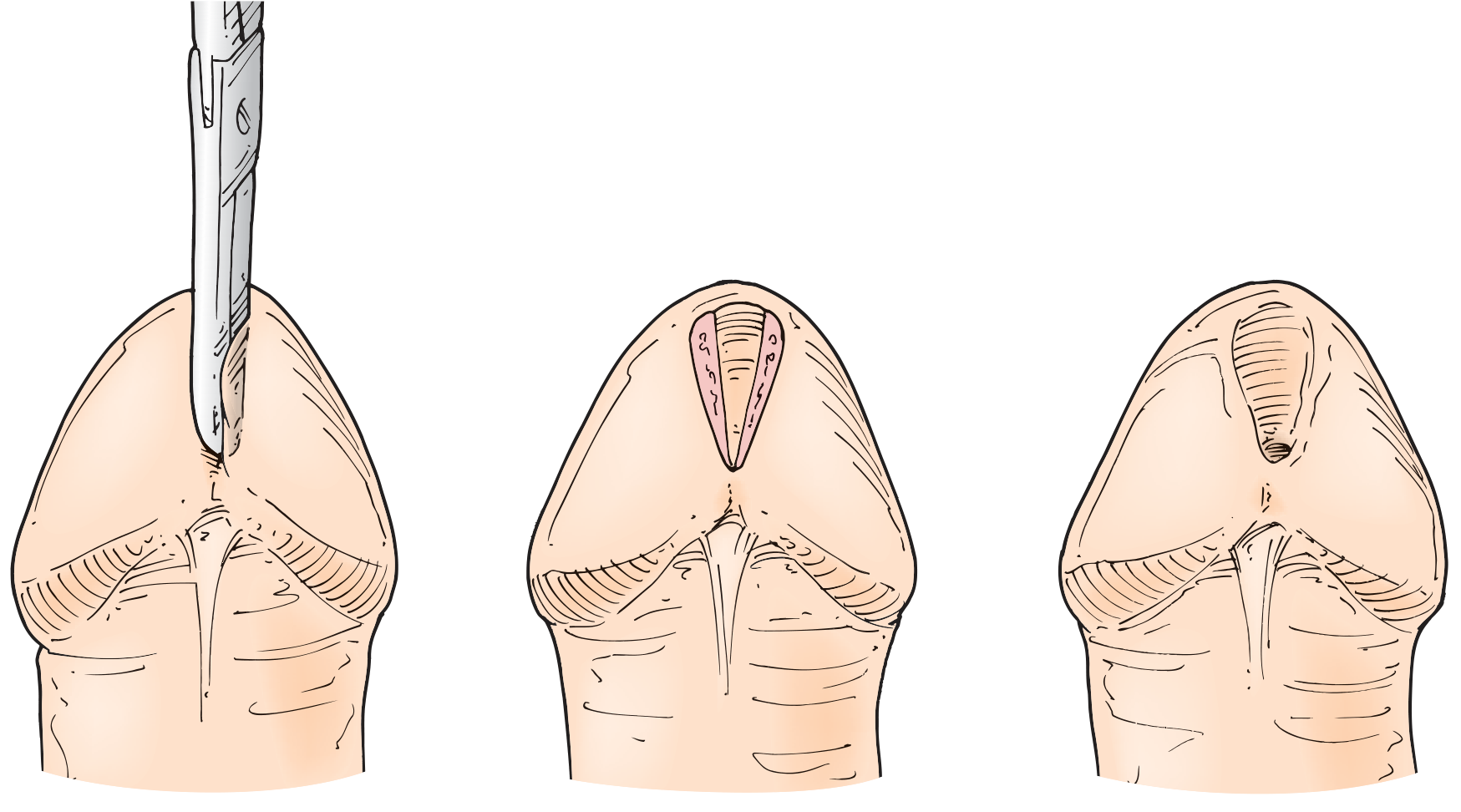
Fig: Sequence showing (L→R): midline incision, widened plate, tubularized/closed neourethra (Hinman's Atlas)
Advantages of TIP:
- Most cosmetically normal meatus (vertical slit)
- Single-stage
- No graft/flap needed in distal cases
- 90%+ used for distal hypospadias in surveys
Limitations of TIP:
- Requires a GOOD, flat, wide urethral plate
- If plate is narrow/stenotic → risk of meatal stenosis
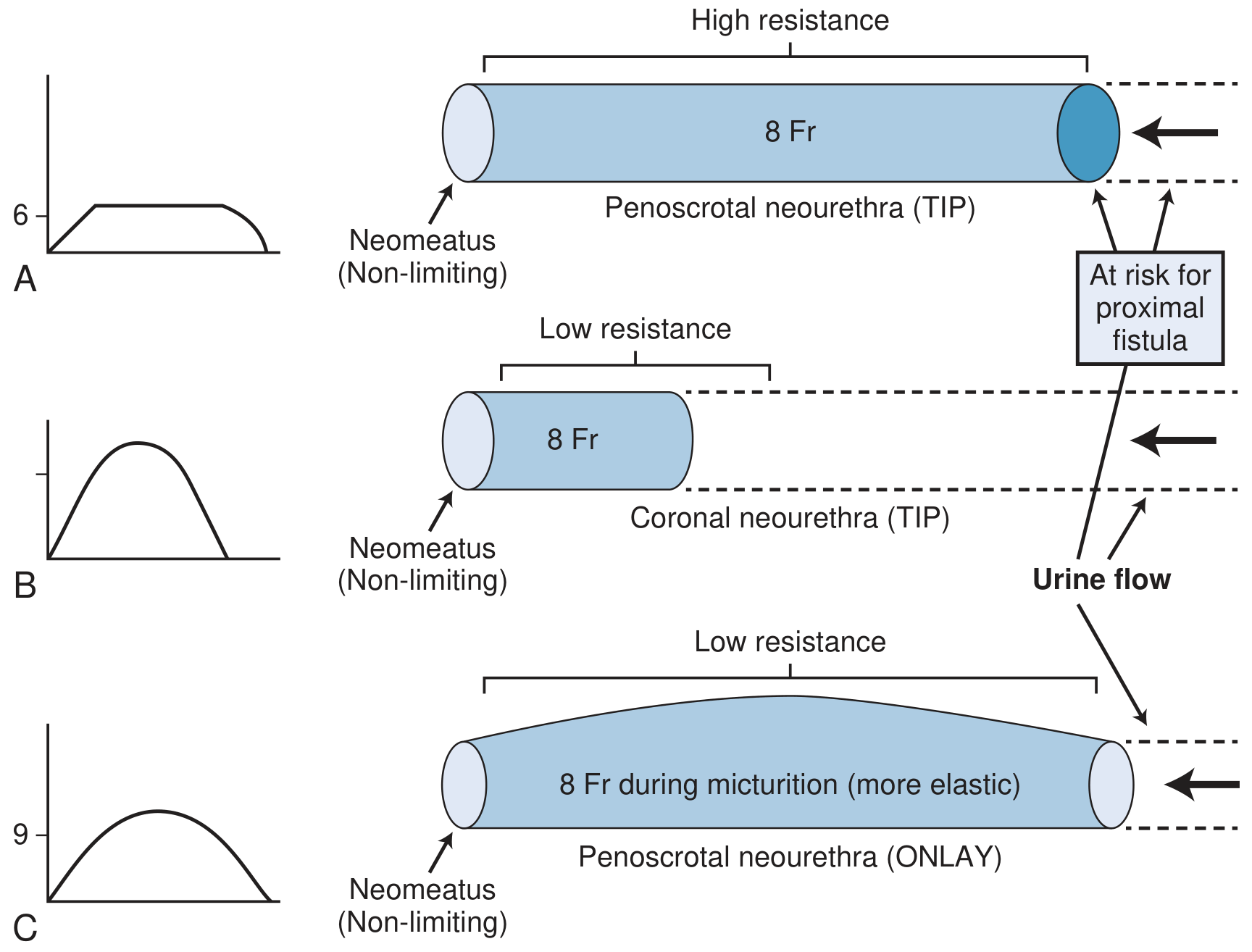
- Long TIP repair (penoscrotal) → HIGH RESISTANCE neourethra → prolonged voiding, poor flow
- Not ideal for proximal hypospadias with severe chordee
Contraindications:
- Severe chordee requiring urethral plate division
- Very narrow or scarred urethral plate
- Redo cases with scarred tissues
C. MATHIEU (FLIP-FLAP) REPAIR
Mathieu, 1932
Indication: Distal/coronal hypospadias with parameatal skin available, wide urethral plate
Steps:
- Parameatal-based proximal flap raised (equal in length to deficient urethra)
- Flap FLIPPED (rotated 180°) onto ventral glans over urethral plate
- Flap and plate edges sutured together distally
- Creates neo-meatus at tip
Advantage: Simple, single-stage, no plate incision needed
Disadvantage: Tendency toward "fish-mouth" meatus appearance; vascular compromise if flap base narrow
D. ONLAY ISLAND FLAP (OIF) / DUCKETT
Indication: Mid-to-proximal hypospadias with good urethral plate that cannot be tubularized alone
Steps:
- Inner preputial skin island flap raised on vascular pedicle (dartos)
- Flap transposed ventrally and sutured as an ONLAY onto the retained urethral plate (augments width)
- Glansplasty performed
Advantage: Elastic tissue → lower resistance (better flow than proximal TIP); less meatal stenosis
Risk: Urethral diverticulum (elasticity of preputial skin), fish-mouth meatus
Fig: TIP (long segment) creates high resistance and prolonged void (A) vs short TIP (B) vs Onlay flap (C) - more elastic, lower resistance, better flow (Campbell-Walsh)
E. TRANSVERSE PREPUTIAL ISLAND FLAP (TPIF) / DUCKETT TUBE
Indication: Proximal hypospadias - one-stage repair when curvature corrected after degloving
Steps:
- Penile degloving + artificial erection to assess curvature
- Transverse preputial inner skin island harvested on dartos pedicle
- Island flap TUBULARIZED into a neourethra
- Anastomosed to native proximal urethra
- Transposed ventrally through buttonhole in pedicle
- Glansplasty completed
Key concern: Fish-mouth meatus; higher diverticulum rate; complication rate higher than OIF
F. TWO-STAGE REPAIR (BRACKA / BYARS)
Indication: Proximal hypospadias with severe chordee requiring urethral plate division; Failed primary repairs; Redo/salvage cases
Stage 1 (Correction):
- Full penile degloving
- Chordee correction - division of urethral plate + division of fibrous tissue
- Multiple ventral corporotomies if needed (corporal lengthening)
- BRACKA: Buccal mucosa graft (BMG) or inner prepucial graft laid on ventral surface and quilted
- BYARS: Dorsal prepucial skin transposed ventrally as pedicled flaps sutured in midline
- Penis allowed to heal for minimum 6 months
Stage 2 (Tubularization):
- U-shaped (Thiersch-Duplay) incision around neourethral template
- Tubularize the graft/flap into neourethra over catheter
- Multilayer closure with dartos cover
- Glansplasty
Advantages: Best correction of severe curvature; allows corporal lengthening; versatile
Disadvantage: Two operations required 6 months apart; higher overall complication rate
G. THIERSCH-DUPLAY TUBULARIZATION
Indication: Wide, flat urethral plate without plate incision (or second stage of staged repair)
Steps:
- U-incision around urethral plate
- Plate edges rolled into tube over catheter
- Closed in 2 layers with dartos cover
- Glansplasty
H. BUCCAL MUCOSA GRAFT (BMG)
Indication: Scarred/stenotic urethra, redo/salvage repairs, inadequate local tissue, failed TIP
Harvest site: Inner cheek or lower lip
Advantage: Robust epithelium, resistant to infection, wet mucosal environment, low contracture
Steps (staged): BMG spread-quilted onto ventral shaft → second stage tubularization
A 2025 systematic review (PMID 39945907) on post-pubertal outcomes after oral mucosa grafts confirmed generally good long-term results in urethral reconstruction for hypospadias.
11. CHORDEE CORRECTION
Artificial erection test (saline injection): Always done intra-operatively to assess curvature
| Degree of Curvature | Management |
|---|
| < 30° | Dorsal plication (Nesbit/modified) |
| 30-60° | Extensive dorsal plication OR corporotomy |
| > 60° | Multiple ventral corporotomies + graft; plate MUST be divided; two-stage preferred |
Dorsal Plication: Midline sutures on dorsal tunica, opposite point of maximal curvature. Simple but shortens penis slightly.
12. POSTOPERATIVE CARE
| Element | Detail |
|---|
| Catheter | 6-Fr silicone "drip stent" sutured to glans |
| Duration | 7-10 days (distal), 10-14 days (proximal) |
| Dressing | Tegaderm/Op-Site wrapped compressively |
| Antibiotics | Co-trimoxazole prophylaxis during catheterization |
| Diaper | Double-diaper technique (catheter drains into outer diaper) |
| Bathing | Avoided 2-4 days; then sitz baths |
| Follow-up | 3-6 months minimum; uroflowmetry at follow-up |
13. COMPLICATIONS
Most Common Complication: Urethrocutaneous Fistula (~10%)
| Complication | Incidence | Time of Presentation |
|---|
| Urethrocutaneous fistula | ~10% | Weeks-months post-op |
| Meatal/urethral stenosis | 5-10% | Weeks-years post-op |
| Glans dehiscence | 5-10% | Early post-op |
| Urethral stricture | Variable | Months-years |
| Urethral diverticulum | Commoner with OIF/TPIF | Months-years |
| Chordee recurrence | 5-30% (proximal) | At puberty |
| Hair in urethra | If scrotal skin used | Puberty |
| Erectile dysfunction | ~25% in adulthood | Adulthood |
| Ejaculatory dysfunction | ~37% | Adulthood |
Most common complication = Urethrocutaneous Fistula
Most common site of fistula = at original meatal site or coronal margin
Management of fistula: Wait 6 months after primary repair → then fistula closure with layered tissue coverage (local flap advancement)
14. INDICATIONS / CONTRAINDICATIONS / TIMING SUMMARY
Indications for Surgery
- All hypospadias except the most minor glanular type
- Functional: poor urinary stream direction, spraying, incomplete emptying
- Cosmetic: abnormal penile appearance
- Psychological: normal appearance for peer development
- Sexual: to enable normal penetrative intercourse
When NOT to Operate
- Isolated minor glanular hypospadias with normal meatus caliber and no chordee (relative)
- Very small phallus → operate only after hormonal priming
- Active local infection
- Before 6 months of age (anesthetic risk)
- In a major syndromic child where surgery adds undue risk
TIMING - Optimal Window
- 6-18 months is universally accepted optimal window
- Before toilet training (typically before 2 years)
- Before psychological awareness of genital differences (~18 months)
- NEVER circumcise before repair
15. KEY EXAM FLOWCHART - MANAGEMENT OF HYPOSPADIAS
NEWBORN MALE → CLINICAL DIAGNOSIS (Ventral meatus + Hooded foreskin + Chordee)
↓
┌──────────────┴──────────────┐
DISTAL (70%) PROXIMAL (30%)
Glanular/Coronal Penoscrotal/Perineal
│ │
No workup needed INVESTIGATE:
• Karyotype
• Hormone panel
• Pelvic USS
• Rule out DSD
│ │
↓ ↓
AVOID CIRCUMCISION ←──── In ALL cases ────→ AVOID CIRCUMCISION
│ │
↓ ↓
Hormonal priming Hormonal priming
if small phallus MANDATORY
│ │
↓ ↓
OPERATE AT 6-18 months OPERATE AT 6-18 months
│ │
↓ ↓
Good urethral plate? Good urethral plate?
Minimal chordee? Severe chordee?
│ │
↓ ↓
TIP (SNODGRASS) ← GOLD STANDARD Two-Stage Repair
[90% of distal repairs] (Bracka BMG or Byars)
│ │
If OIF needed (proximal Stage 1: Chordee correction
but plate OK): ONLAY FLAP + graft/flap placement
│ (wait 6 months)
↓ │
POST-OP: Stage 2: Tubularization
Catheter 7-10 days + Glansplasty
Antibiotics prophylaxis
Uroflowmetry at follow-up
│
↓
COMPLICATION? (10% fistula, 5-10% stenosis)
│
↓
Wait 6 months → Redo/Fistula closure
(Buccal mucosa graft for major redo)
16. CRISP POINT SUMMARY (Exam Crux)
| # | High-Yield Point |
|---|
| 1 | Hypospadias = MOST COMMON congenital urethral anomaly (1:300 males) |
| 2 | Glanular = most common type; Perineal = least common, most severe |
| 3 | Classic triad: Ventral meatus + Hooded foreskin + Chordee |
| 4 | Etiology: Inadequate androgen (T/DHT) effect on urethral folds/ectoderm |
| 5 | Genes: SRD5A2, AR, MAMLD1 most important |
| 6 | Perineal + bilateral cryptorchidism → DSD workup (karyotype mandatory) |
| 7 | NEVER circumcise - prepuce = future graft material |
| 8 | Optimal surgical age = 6-18 months |
| 9 | TIP (Snodgrass) = Gold standard for distal hypospadias |
| 10 | TIP key step = Midline incision of urethral plate (widens it) |
| 11 | Dartos flap = waterproofing layer over neourethra (reduces fistula) |
| 12 | Most common complication = Urethrocutaneous fistula (~10%) |
| 13 | Proximal + severe chordee → Two-stage repair (Bracka BMG or Byars) |
| 14 | Fistula management: wait 6 months then surgical closure |
| 15 | Buccal mucosa graft = graft of choice for redo/salvage |
| 16 | Artificial erection test done intra-operatively to assess chordee |
| 17 | Chordee > 60° → corporal lengthening + two-stage |
| 18 | Post-op follow-up includes uroflowmetry |
| 19 | ART (IVF) doubles hypospadias risk |
| 20 | Onlay Island Flap → risk of urethral diverticulum (elastic preputial skin) |
Recent Evidence (2024-2026):
- Topical estrogen/hormone priming systematic review 2024 - supports pre-op hormonal priming for small phallus (PMID: 38739164)
- Oral mucosa graft outcomes 2025 - confirms good post-pubertal outcomes for buccal mucosa urethral reconstruction (PMID: 39945907)
- Platelet-rich plasma in hypospadias repair meta-analysis 2026 - emerging adjunct to reduce fistula risk (PMID: 42001334)
- TIP repair: interrupted vs continuous sutures meta-analysis 2026 - interrupted sutures may have lower fistula rate (PMID: 42240839)
Sources: Campbell-Walsh Wein Urology (10th Ed), Bailey & Love's Short Practice of Surgery (28th Ed), Hinman's Atlas of Urologic Surgery, The Developing Human - Moore & Persaud, Schwartz's Principles of Surgery (11th Ed)