Tell about pulmonary embolism
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive content from Rosen's Emergency Medicine, Fuster & Hurst's The Heart, and Braunwald's Heart Disease. I have enough to compose a thorough answer.
Pulmonary Embolism (PE)
Definition & Epidemiology
Pulmonary embolism is the obstruction of one or more pulmonary arteries, most commonly by a thrombus originating in the deep veins of the lower extremities or pelvis. It is the most serious clinical presentation of venous thromboembolism (VTE) — the third most frequent cardiovascular disease, with an overall annual incidence of 75–270 cases per 100,000 inhabitants. The risk of VTE roughly doubles with each decade after age 40. One-month mortality ranges from 9–11%, rising to 17% at 3 months; undiagnosed or late-diagnosed cases drive a substantial portion of these deaths. Approximately one-third of patients die within the first hours of presentation, often before diagnosis is confirmed. — Fuster and Hurst's The Heart, 15th Ed.
Pathophysiology
Thrombosis forms when Virchow's triad converges: venous stasis, endothelial injury, and hypercoagulability. Clot dislodges, travels through the right heart, and lodges in the pulmonary vasculature. The consequences are dual:
Respiratory effects:
- Dead-space ventilation (ventilated but unperfused alveoli) → hypoxemia
- Reflex bronchoconstriction, surfactant loss, atelectasis
- Peripheral PE → pulmonary infarction with pleuritic pain and hemoptysis
Hemodynamic effects:
- Increased pulmonary vascular resistance → acute right ventricular (RV) pressure overload
- RV dilation causes interventricular septal shift toward the left ventricle (LV), reducing LV filling → decreased cardiac output → systemic hypotension
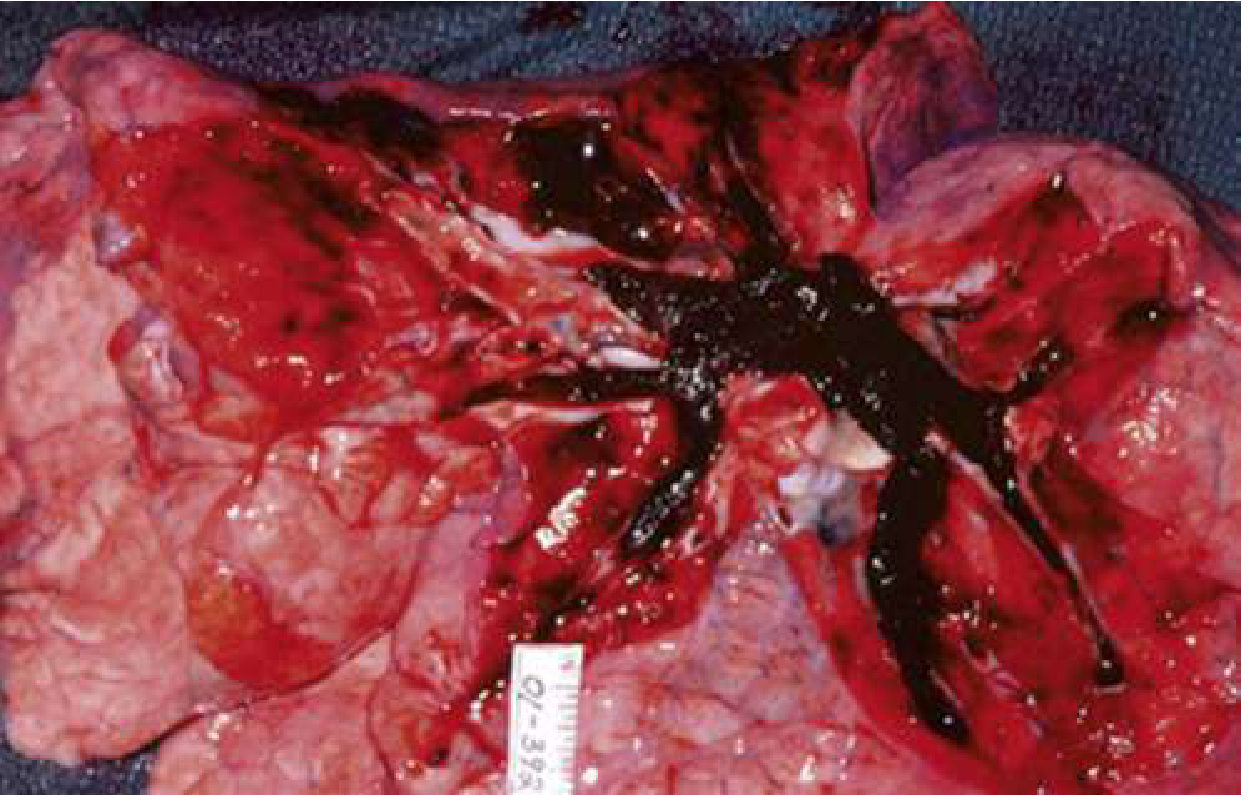
- RV ischemia from increased wall tension + reduced coronary perfusion pressure → RV failure → cardiogenic shock
In its most extreme form, PE occludes the entire right ventricular outflow system (see autopsy photo below), leading to sudden cardiovascular collapse. Approximately 25% of sudden cardiac deaths are attributed to PE. — Rosen's Emergency Medicine
Risk Factors
| Category | Examples |
|---|---|
| Immobility / stasis | Prolonged travel, hospitalization, paralysis |
| Surgery / trauma | Orthopedic surgery (hip/knee), major abdominal surgery |
| Malignancy | Active cancer (especially mucin-secreting adenocarcinomas) |
| Hypercoagulable states | Factor V Leiden, antiphospholipid syndrome, protein C/S deficiency |
| Hormonal | Oral contraceptives, HRT, pregnancy/postpartum |
| Prior VTE | Single strongest predictor of recurrence |
| Medical illness | Heart failure, COPD, nephrotic syndrome, COVID-19 infection |
Clinical Presentation
The presentation ranges from asymptomatic to sudden cardiac arrest. No single symptom is pathognomonic.
Symptoms (in order of frequency):
- Dyspnea — most common; present in 75–80% of patients. May be vague (fatigue, inability to take a full breath). Absent in ~25%
- Chest pain — second most common; pleuritic (sharp, worse with breathing) in 20%, indicating peripheral infarction. Up to one-third have no chest pain
- Cough / hemoptysis — with pulmonary infarction; fever usually low-grade (>38.6°C suggests infection)
- Leg swelling — unilateral, present in <30% but relatively specific when combined with dyspnea
- Syncope — present in <5% of all syncope, but warrants PE workup especially with risk factors
Signs:
- Tachycardia (most common sign)
- Tachypnea, hypoxia
- Hypotension or shock (high-risk PE)
- Elevated JVP, RV heave, loud P2 (acute cor pulmonale)
- Pleural friction rub (infarction)
— Rosen's Emergency Medicine
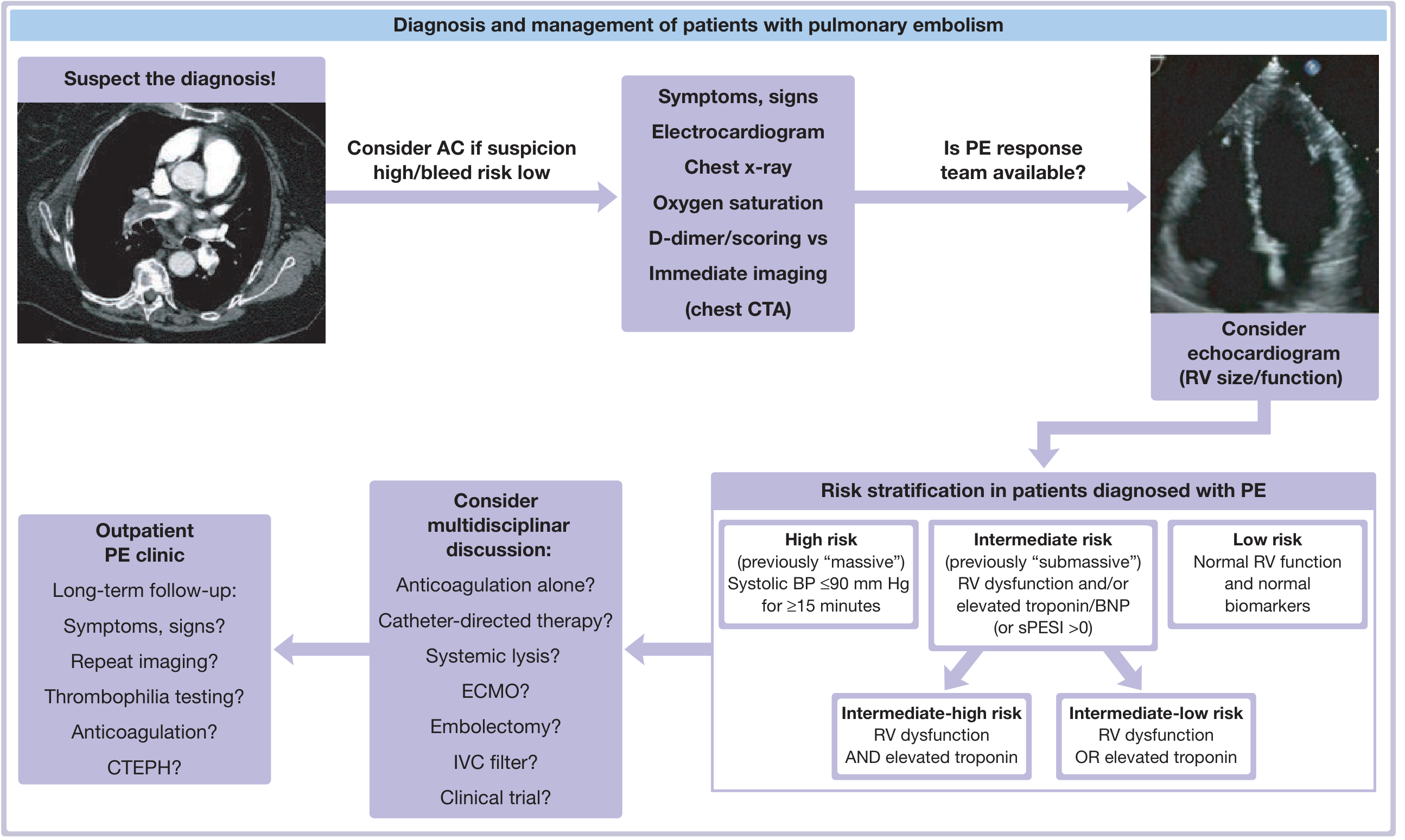
Classification
| Risk Category | Old Term | Criteria |
|---|---|---|
| High-risk | Massive | Hemodynamic instability: systolic BP ≤90 mmHg for ≥15 min |
| Intermediate-high risk | Submassive | RV dysfunction AND elevated troponin |
| Intermediate-low risk | Submassive | RV dysfunction OR elevated troponin (not both) |
| Low-risk | — | Normal RV function, normal biomarkers, hemodynamically stable |
The simplified Pulmonary Embolism Severity Index (sPESI) >0 places a patient in at least intermediate risk. — Fuster and Hurst's The Heart, 15th Ed.
Diagnosis
Pre-test Probability Scoring
- Wells score and Geneva score stratify patients into low, intermediate, or high probability before testing
- In low-probability patients, a negative D-dimer effectively excludes PE (high sensitivity, low specificity)
- Age-adjusted D-dimer threshold (age × 10 µg/L in patients >50 years) improves specificity
Key Investigations
| Test | Finding in PE |
|---|---|
| D-dimer | Sensitive but not specific; elevated in many conditions |
| ECG | Sinus tachycardia (most common); S1Q3T3 pattern; RBBB; right axis deviation |
| Chest X-ray | Often normal; may show Hampton's hump (wedge opacity), Westermark sign (oligemia), atelectasis |
| ABG | Hypoxemia, hypocapnia, respiratory alkalosis; A-a gradient elevated |
| Troponin / BNP | Elevated with RV strain; prognostic value |
| CT Pulmonary Angiography (CTPA) | Gold standard; direct visualization of emboli |
| V/Q scan | Useful when CTPA contraindicated (renal failure, allergy, pregnancy) |
| Echocardiography | RV dilation, septal shift, elevated RVSP; confirms RV dysfunction for risk stratification |
| Compression ultrasound | Confirms DVT; supports diagnosis in high-suspicion patients |
CTPA is the imaging modality of choice in most settings. In hemodynamically unstable patients, bedside echo is invaluable. — Braunwald's Heart Disease; Rosen's Emergency Medicine
Management
Anticoagulation (cornerstone of therapy)
Anticoagulation reduces mortality and prevents thrombus propagation and recurrence. It should be started before imaging confirmation if clinical suspicion is high and bleeding risk is acceptable.
- DOACs (preferred): Rivaroxaban or apixaban (no heparin bridge needed); edoxaban/dabigatran require initial parenteral anticoagulation
- LMWH: Preferred in cancer-associated PE; weight-based dosing, predictable pharmacokinetics
- Unfractionated heparin (UFH): Used when thrombolysis or embolectomy is planned; rapid reversibility; titrated by aPTT
- Warfarin: Requires INR monitoring (target 2–3); overlap with heparin for ≥5 days until INR therapeutic
Advanced / Reperfusion Therapy (for high-risk and selected intermediate-high risk PE)
| Modality | When Used |
|---|---|
| Systemic thrombolysis (tPA, streptokinase) | High-risk PE (hemodynamically unstable), no absolute contraindications |
| Catheter-directed thrombolysis (CDT) | Intermediate-high risk; lower bleeding risk than systemic lysis |
| Catheter-directed embolectomy / aspiration | Contraindication to thrombolysis; emerging endovascular options |
| Surgical embolectomy | Thrombolysis failure or contraindicated; requires cardiopulmonary bypass |
| ECMO | Bridge to definitive therapy in refractory cardiac arrest |
| IVC filter | Anticoagulation absolutely contraindicated; recurrent PE despite anticoagulation |
Hemodynamic Support
- Small fluid boluses (250–500 mL) for hypotension; avoid aggressive fluid resuscitation (worsens RV dilation)
- Norepinephrine is first-line vasopressor; dobutamine as adjunct (may worsen hypotension if used alone)
- Avoid intubation if possible — positive pressure ventilation reduces preload and can precipitate cardiac arrest
Low-risk PE: Outpatient Treatment
Carefully selected low-risk patients (negative Hestia criteria or sPESI = 0) can be safely discharged on DOAC therapy. — Rosen's Emergency Medicine; Fuster and Hurst's The Heart, 15th Ed.
Duration of Anticoagulation
| Situation | Duration |
|---|---|
| Provoked PE (surgery, transient risk factor) | 3 months |
| Unprovoked PE (first episode) | ≥3 months; consider extended therapy |
| Recurrent unprovoked PE | Indefinite |
| Active malignancy | Indefinite (LMWH or DOAC) |
| Antiphospholipid syndrome | Indefinite (warfarin preferred) |
Complications & Long-term Sequelae
- Post-PE syndrome: Persistent dyspnea, exercise limitation, reduced quality of life after acute PE
- Chronic Thromboembolic Pulmonary Hypertension (CTEPH): Occurs in ~1–4% of PE survivors; unresolved thrombi organize and occlude pulmonary vessels → progressive pulmonary hypertension. Potentially curable with pulmonary thromboendarterectomy (PTE)
- Recurrent VTE: Risk remains elevated, especially in unprovoked PE
- Paradoxical embolism: Thrombus crossing a patent foramen ovale (PFO) → systemic arterial embolism (stroke, limb ischemia)
Special Populations
- Pregnancy: CTPA or V/Q scan; LMWH preferred (DOACs contraindicated); increased baseline risk due to venous stasis and hypercoagulability
- Cancer: LMWH or DOACs (edoxaban, rivaroxaban) preferred over warfarin; higher recurrence risk
- COVID-19: Significantly elevated risk of VTE and PE; likely multifactorial (endothelial injury, hypercoagulability, immobility)
Key Points Summary
- PE is a clinical emergency with high mortality if unrecognized
- The most common symptom is dyspnea; the most common sign is tachycardia — but either may be absent
- Risk stratify with hemodynamic status + RV function + biomarkers (troponin, BNP)
- CTPA is the gold standard imaging test; D-dimer rules out PE in low-probability patients
- Anticoagulate early — this is the intervention that reduces mortality
- High-risk PE requires systemic thrombolysis or embolectomy in addition to anticoagulation
- Watch for CTEPH in follow-up — persistent dyspnea after 3 months warrants evaluation
Sources: Rosen's Emergency Medicine; Fuster and Hurst's The Heart, 15th Ed.; Braunwald's Heart Disease, 2-Vol Set
This is a shared conversation. Sign in to Orris to start your own chat.