What is the initial cause of unconsciousness in lucid interval due to epidural hemorrhage
Reading File
Finding Sources
Searching PubMed
"epidural hematoma" AND "lucid interval" AND pathophysiology
Reading File
Reading File
Here is a clear, textbook-supported answer:
Initial Cause of Unconsciousness in the Lucid Interval of Epidural Hemorrhage
The classic triad of epidural hematoma (EDH) is:
- Initial loss of consciousness (at time of impact)
- Lucid interval (period of regained consciousness)
- Recurrent loss of consciousness with neurological deterioration
The Initial Unconsciousness
The initial loss of consciousness is caused by the concussive force of the traumatic head injury itself - specifically, the sudden mechanical disruption of the reticular activating system (RAS) in the brainstem from the impact. This is a transient concussive effect, not from blood accumulation.
At this stage, there is little or no hematoma yet - the middle meningeal artery has just been lacerated (typically from a temporal bone fracture), and the epidural space has not yet accumulated enough blood to exert significant mass effect.
The Lucid Interval
As the brain "recovers" from the concussive shock and the patient regains consciousness, blood continues to slowly accumulate in the epidural space under arterial pressure from the injured middle meningeal artery. The brain initially compensates through CSF displacement and cerebral venous compression.
The Second Loss of Consciousness
The second, more ominous deterioration is caused by the expanding hematoma compressing the brain, leading to:
- Uncal herniation compressing the ipsilateral midbrain and CN III (fixed, dilated pupil)
- Brainstem compression
- Raised intracranial pressure
As Schwartz's Principles of Surgery states: "The final stages of this sequence are caused by blood accumulation that forces the temporal lobe medially, with resultant compression of the third cranial nerve and eventually the brain stem." - Schwartz's Principles of Surgery, 11th ed.
Summary Table
| Phase | Mechanism | Cause |
|---|---|---|
| Initial unconsciousness | Concussive disruption of RAS | Traumatic impact force |
| Lucid interval | Compensation, concussion resolving | Hematoma still small |
| Second unconsciousness | Hematoma expansion, herniation | Arterial bleeding (MMA) |
The key teaching point: the first loss of consciousness = concussion (traumatic impact); the second = expanding hematoma with herniation. These are two distinct mechanisms.
Explain the cause of contralateral hemiplegia
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a complete, textbook-supported explanation:
Contralateral Hemiplegia in Epidural Hemorrhage
The Anatomical Basis
The corticospinal tract (the main motor pathway) originates in the motor cortex, descends through the internal capsule and cerebral peduncles in the midbrain, then crosses (decussates) at the pyramidal decussation in the lower medulla before continuing down the spinal cord.
Because the crossing happens below the midbrain, any compression of the corticospinal tract at or above the midbrain level will produce weakness on the opposite (contralateral) side of the body.
Step-by-Step Mechanism in EDH
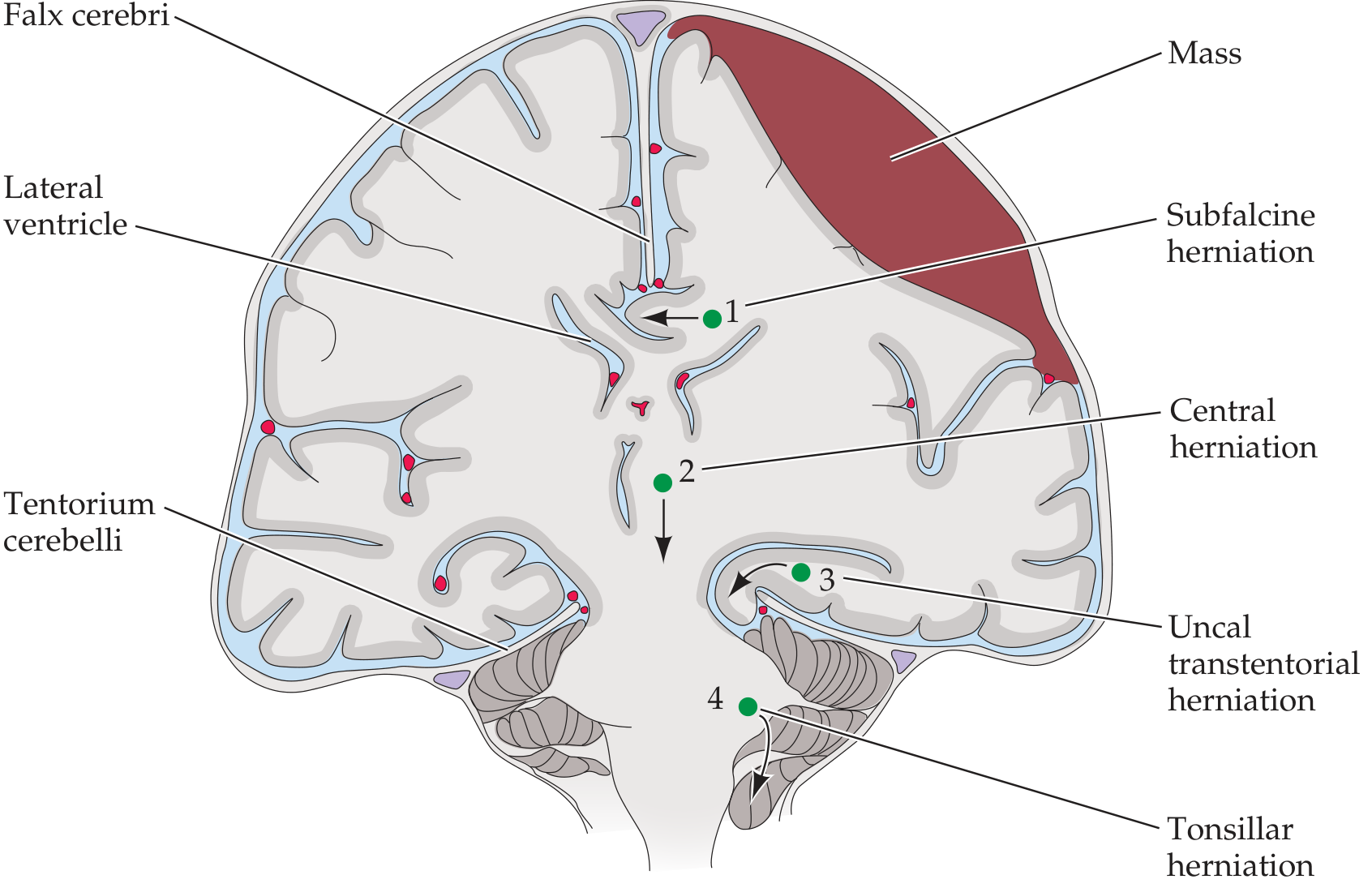
- Hematoma expands in the epidural space (typically temporal/temporoparietal, from middle meningeal artery laceration)
- Rising ICP pushes the medial temporal lobe (uncus) downward through the tentorial notch - this is uncal transtentorial herniation
- The herniating uncus compresses the ipsilateral cerebral peduncle in the midbrain
- The cerebral peduncle contains the corticospinal tract on that same side
- Since the corticospinal tract has not yet crossed at this level, compression here produces weakness on the contralateral side of the body
The Classic Triad of Uncal Herniation
| Sign | Side | Mechanism |
|---|---|---|
| Fixed, dilated pupil | Ipsilateral to hematoma (85%) | CN III compression by herniating uncus |
| Hemiplegia | Contralateral (usually) | Ipsilateral cerebral peduncle compressed; tract not yet crossed |
| Coma | - | Midbrain reticular activating system distortion |
Important Exception - Kernohan's Notch Phenomenon
As the textbook notes, sometimes the midbrain is pushed so far to the opposite side that it is compressed against the contralateral tentorial notch. In this case, the contralateral cerebral peduncle is compressed, producing hemiplegia that is ipsilateral to the lesion - a "false localizing sign" known as Kernohan's notch phenomenon.
"Sometimes in uncal herniation, the midbrain is pushed all the way over until it is compressed by the opposite side of the tentorial notch. In these cases the contralateral corticospinal tract is compressed, producing hemiplegia that is ipsilateral to the lesion." - Neuroanatomy through Clinical Cases, 3rd ed.
Summary
Contralateral hemiplegia (the typical finding) results from the expanding epidural hematoma causing uncal herniation, which compresses the ipsilateral cerebral peduncle (corticospinal tract in the midbrain). Because this is above the pyramidal decussation, the motor deficit manifests on the opposite side of the body from the hematoma.
This is a shared conversation. Sign in to Orris to start your own chat.