Now I have comprehensive material from the textbooks and images. Let me compile a thorough, well-structured set of notes.
Methods of Examination of Children with Respiratory System Diseases
1. History Taking (Anamnesis)
A structured history in a child with respiratory complaints should cover:
Chief Complaint & Onset
- Duration and onset of symptoms (acute vs. chronic/recurrent)
- Cough: character (dry, productive, barking/croupy, staccato), timing (nocturnal, post-exercise), severity
- Dyspnea: at rest vs. on exertion; positional (orthopnea suggests cardiac/pleural disease)
- Wheeze, stridor, noisy breathing
- Fever, rhinorrhea, sore throat (viral URTI preceding LRT involvement)
- Cyanosis episodes
Birth & Developmental History
- Gestational age, birth weight (prematurity → chronic lung disease of prematurity)
- Neonatal respiratory distress, ventilator use
- Feeding difficulties (aspiration, gastro-oesophageal reflux)
Past Medical & Immunisation History
- Recurrent chest infections, prior hospitalisation/ICU admissions
- Asthma, atopy (eczema, allergic rhinitis)
- Immunisation status (pertussis, measles, Haemophilus influenzae, pneumococcus)
- TB contact or travel history
Family & Environmental History
- Parental asthma, atopy, cystic fibrosis
- Smoking in household (passive smoke)
- Pets, mould, dust mites, recent sick contacts
- Day-care attendance (increased exposure to respiratory viruses)
Feeding & Nutrition — malnutrition impairs respiratory muscle reserve and immune defence.
2. Inspection Techniques
Respiratory Rate Counting
Respiratory rate (RR) is the single most sensitive sign of respiratory compromise in children and must be counted over a full 60 seconds in a quiet, calm child (crying elevates RR).
| Age Group | Normal RR (breaths/min) |
|---|
| Neonate (0–1 month) | 40–60 |
| Infant (1–12 months) | 30–50 |
| Toddler (1–3 years) | 24–40 |
| Preschool (3–5 years) | 22–34 |
| School-age (6–12 years) | 18–30 |
| Adolescent (>12 years) | 12–20 |
Technique: Observe the rise and fall of the chest/abdomen (infants are abdominal breathers) without alerting the child. Using a watch or timer, count for a full minute or count 30 s and multiply ×2.
Chest Shape Assessment
Observe the child undressed from the front, side, and back:
- Normal: Elliptical cross-section; AP:transverse diameter ≈ 1:2 in older children
- Barrel chest (increased AP diameter): air trapping in chronic asthma, bronchiolitis, cystic fibrosis
- Pectus excavatum (funnel chest): depression of lower sternum; can compress lungs
- Pectus carinatum (pigeon chest): protrusion of sternum; seen in chronic respiratory disease
- Harrison's sulcus: transverse groove along the lower costal margin caused by chronic increased work of breathing (rickets, chronic asthma)
- Kyphoscoliosis: reduces lung volume and causes restrictive pattern
- Asymmetry: one side flattened (collapse, fibrosis) or bulging (large effusion, tension pneumothorax)
Also note:
- Breathing pattern: abdominal (normal in infants/toddlers), costal (older children/adults); paradoxical chest movement suggests flail chest or respiratory muscle weakness
- Cyanosis: central (tongue/mucous membranes) vs. peripheral; indicates severe hypoxaemia
3. Types of Pathological Breathing
| Term | Definition | Causes |
|---|
| Tachypnea | RR above age-adjusted upper limit | Pneumonia, asthma, bronchiolitis, fever, metabolic acidosis, sepsis, heart failure |
| Bradypnea | Abnormally slow RR | Central depression (opioids, seizure, CNS injury), severe fatigue/impending arrest |
| Apnea | Cessation of breathing >20 s (or shorter if accompanied by bradycardia/cyanosis) | Prematurity (central apnea), obstructive sleep apnoea, seizures, sepsis in neonates |
| Cheyne-Stokes | Cyclical crescendo–decrescendo respiration with central apnoea | Heart failure, CNS disease, severe anaemia |
| Kussmaul breathing | Deep, laboured, regular breathing | Metabolic acidosis (DKA, renal failure) |
| Biot's breathing | Irregular rate and depth with sudden apnoeic pauses | Meningitis, severe brain injury |
| Agonal breathing | Gasping, irregular | Pre-terminal event |
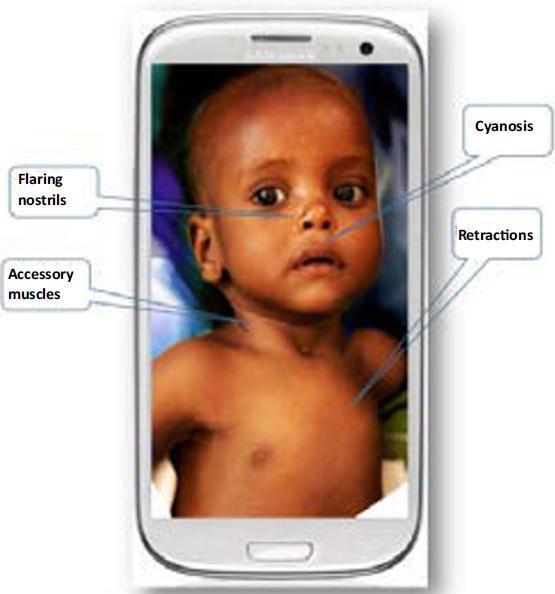
4. Recognition of Respiratory Distress Signs
Increased work of breathing (WOB) in children is visible because the chest wall is highly compliant. The Paediatric Assessment Triangle (PAT) classifies children using Appearance + Work of Breathing + Circulation.
Nasal Flaring
- Rhythmic widening of the nares on inspiration
- Increases the cross-sectional area of the nasal airway, reducing resistance
- Common in infants and young children with pneumonia, bronchiolitis, or upper airway obstruction
Retractions (Indrawing)
Inward movement of soft tissues during inspiration due to high negative intrapleural pressure generated against an obstructed or stiff airway/lung. Locations and their clinical significance:
| Location | Significance |
|---|
| Subcostal | Moderate–severe distress; most common |
| Intercostal | Moderate distress |
| Suprasternal (tracheal tug) | Severe distress; upper airway obstruction |
| Supraclavicular | Severe distress |
| Sternal (substernal) | Infants; high compliance chest wall |
The lower in the chest wall, the more severe the distress. Subcostal and lower sternal retractions ("abdominal indrawing") suggest severe disease.
— ROSEN's Emergency Medicine
Grunting
- Expiratory sound produced by partial closure of the glottis during exhalation
- Acts as auto-PEEP: maintains functional residual capacity (FRC) and prevents alveolar collapse
- Indicates significant lung disease (neonatal RDS, pneumonia, pulmonary oedema, severe bronchiolitis)
- Always a serious sign requiring urgent assessment
Accessory Muscle Use
- Sternocleidomastoid, scalene, and trapezius recruitment on inspiration
- Causes head bobbing in infants (SCM use moves the head with each breath)
Tripod/Sniffing Position
- Child leans forward on outstretched arms (tripod) or juts chin forward (sniffing)
- Optimises airway patency; seen in severe croup, epiglottitis, foreign body
Summary — PAT Work of Breathing Assessment
| Feature | Significance |
|---|
| Audible wheezing | Lower airway obstruction |
| Stridor | Upper airway obstruction |
| Grunting | Alveolar collapse/lung disease |
| Retractions | Increased work of breathing |
| Nasal flaring | Increased WOB (especially infants) |
| Head bobbing | Severe increased WOB (infants) |
5. Palpation
Chest Expansion
Technique: Place both hands symmetrically on the lower chest with thumbs meeting at the midline; ask the child to take a deep breath and observe how far the thumbs separate.
- Normal: equal and full bilateral expansion
- Unilateral reduction: Pneumothorax, consolidation, effusion, atelectasis, endobronchial obstruction on that side
- Bilateral reduction: Generalised hyperinflation (asthma), bilateral disease, neuromuscular weakness
In small infants, expansion is assessed by observation rather than hand placement.
Vocal (Voice/Tactile) Fremitus
Technique: Place the palm or ulnar border of the hand on the chest wall; ask the child to say "ninety-nine" or "one-one-one" (or cry in an infant) and feel the transmitted vibration.
| Finding | Interpretation |
|---|
| Increased fremitus | Consolidation (solid lung transmits sound better) |
| Decreased/absent fremitus | Pleural effusion (fluid attenuates transmission), pneumothorax (air), large airway obstruction |
- Less reliable in infants/toddlers; tremor and crying complicate assessment
- Confirm with percussion and auscultation
Tracheal Position
- Palpate the trachea in the suprasternal notch
- Deviation toward lesion: Collapse, atelectasis, fibrosis
- Deviation away from lesion: Tension pneumothorax, large pleural effusion
6. Percussion
Technique: Place the middle finger of the non-dominant hand firmly against the chest wall (parallel to ribs); strike its distal interphalangeal joint sharply with the middle finger of the dominant hand. In infants, use a single finger on a single finger (one-finger technique). Percuss symmetrically, comparing sides at each level.
Comparative Percussion
Side-to-side comparison at the same anatomical level; any asymmetry is pathological.
Topographic (Boundary) Percussion
Identifies the borders of lung, liver, heart, and diaphragm.
Normal lung boundaries (children):
- Anterior: 2nd–6th rib
- Lateral: axillary region down to 8th rib
- Posterior upper border: at level of C7 (lung apex)
- Lower border posteriorly: approximately T10 at rest
Diaphragm excursion: Percuss from resonant to dull on expiration vs. full inspiration — normal excursion is 3–5 cm. Reduced in paralysed hemidiaphragm or hyperinflation.
7. Pathological Percussion Sounds
| Percussion Note | Quality | Causes |
|---|
| Normal (resonance) | Medium pitch, hollow | Normal aerated lung |
| Dullness | High pitch, short, "thuddy" | Consolidation (pneumonia), pleural effusion, atelectasis, mass |
| Stony dullness | Extreme dullness, very flat | Large pleural effusion |
| Hyperresonance | Lower pitch than normal, booming | Pneumothorax, severe emphysema/air-trapping (asthma attack), large bulla |
| Tympany | Drum-like, musical | Gastric bubble (below left hemidiaphragm), large pneumothorax, tension pneumothorax |
Clinical correlation:
- Consolidation: dull + increased fremitus + bronchial breathing
- Pleural effusion: stony dull + absent fremitus + absent breath sounds ± pleural rub above effusion
- Pneumothorax: hyperresonant/tympanitic + absent fremitus + absent breath sounds
- Atelectasis: dull + reduced expansion on that side + absent or reduced breath sounds
8. Auscultation Technique and Normal Breath Sounds
Technique:
- Use a paediatric stethoscope with a small diaphragm (or bell for low-pitched sounds)
- Child sitting upright if possible, arms slightly forward (to protract scapulae and expose posterior fields)
- Auscultate systematically: anterior → lateral → posterior, comparing sides at each level
- Ask cooperating children to breathe deeply through an open mouth; in infants, listen during quiet breathing and during crying for bronchovesicular sounds
- Warm the stethoscope chest piece before use
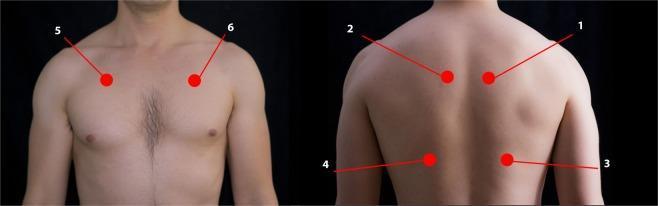
Sequence of auscultation points:
- Anterior: 2nd ICS midclavicular line bilaterally, 4th–5th ICS
- Lateral: mid-axillary line at 4th–6th ICS
- Posterior: above spine of scapula, between scapula and spine (interscapular), below scapula (infrascapular), basal angles
Normal Breath Sounds
| Sound | Location | Character |
|---|
| Vesicular | Most of lung periphery | Soft, low-pitched; inspiration > expiration; no pause between phases |
| Bronchovesicular | Over main bronchi (manubrium anteriorly, between scapulae posteriorly) | Intermediate; inspiration = expiration |
| Bronchial (tracheal) | Over trachea/large bronchi | Loud, high-pitched; expiration > inspiration; pause between phases |
In young infants, breath sounds are louder and more bronchial-sounding throughout the chest due to the thin chest wall — this is normal.
9. Pathological Breath Sounds
Altered Transmission Sounds
| Finding | Description | Causes |
|---|
| Bronchial breathing (over peripheral lung) | Loud, tubular; expiration ≥ inspiration | Consolidation (sound transmitted through solidified lung), collapse with patent bronchus |
| Diminished/absent breath sounds | Reduced air entry | Pleural effusion, pneumothorax, severe asthma (silent chest), atelectasis, obesity |
| Amphoric breathing | Hollow, echoing | Large cavity (abscess, cavitated TB) |
Added/Adventitious Sounds
Wheezing
- High-pitched musical sound, predominantly expiratory (can be biphasic)
- Generated by turbulent flow through narrowed lower airways
- Causes: asthma (diffuse, bilateral, polyphonic), bronchiolitis, foreign body (focal, monophonic), cardiac failure
- Monophonic wheeze = single airway obstruction (foreign body, mucous plug)
- Polyphonic wheeze = generalised airway narrowing (asthma)
Crackles (Rales)
- Discontinuous, explosive sounds caused by sudden opening of collapsed small airways or by air bubbling through secretions
- Fine crackles (crepitations): High-pitched, late inspiratory; heard in pneumonia (alveolar), pulmonary oedema, fibrosis; do not clear with cough
- Coarse crackles: Low-pitched, early inspiratory and expiratory; secretions in larger airways (bronchiectasis, CF); may partially clear with cough
Stridor
- Harsh, high-pitched sound, predominantly inspiratory
- Generated by partial obstruction at or above the level of the larynx/extrathoracic trachea
- Inspiratory stridor: Supraglottic/glottic obstruction (croup, epiglottitis, foreign body, haemangioma)
- Expiratory stridor: Subglottic/upper tracheal (fixed obstruction)
- Biphasic stridor: Glottic/subglottic obstruction (fixed, critical)
| Type | Likely Level |
|---|
| Inspiratory only | Supraglottic/glottic |
| Expiratory only | Tracheal/subglottic |
| Biphasic | Glottic/subglottic (more severe) |
Ronchi (Rhonchi)
- Low-pitched, snoring/musical sounds generated by secretions in larger airways
- Predominantly expiratory; may clear with coughing
10. Pleural Friction Rub and Crepitus
Pleural Friction Rub
- Character: Creaking, grating, leathery sound — like two pieces of sandpaper rubbed together
- Timing: Heard in both inspiration and expiration, usually at the end of inspiration and beginning of expiration
- Location: Lower lateral chest wall (most common site of pleuritis)
- Mechanism: Inflammation of the parietal and visceral pleura causes loss of normal smooth serosal surface; friction during respiratory movements generates the sound
- Causes: Pleuritis (viral, bacterial pneumonia with pleural involvement), pulmonary embolism with infarction, systemic lupus erythematosus, tuberculosis, malignancy
- Key distinguishing feature: Does NOT change with coughing (unlike crackles); disappears when the patient holds their breath; disappears once effusion accumulates (fluid separates the pleural surfaces)
Subcutaneous Crepitus (Surgical Emphysema)
- Crackling sensation on palpation of the skin (like crushing cornstarch)
- Air in the subcutaneous tissues
- Causes: Pneumothorax with chest wall tracking, after thoracic trauma or procedure, spontaneous in children (after severe vomiting – Hamman's sign for pneumomediastinum)
Summary: Examination Findings in Common Paediatric Respiratory Conditions
| Condition | Inspection | Percussion | Fremitus | Auscultation |
|---|
| Pneumonia (consolidation) | Dull, tachypnoeic | Dull | Increased | Bronchial breathing, fine crackles |
| Pleural effusion | Reduced expansion | Stony dull | Absent | Absent breath sounds ± rub above |
| Pneumothorax | Asymmetric, tracheal shift | Hyperresonant | Absent | Absent breath sounds |
| Asthma attack | Barrel, accessory muscles, retractions | Hyperresonant | Normal/reduced | Polyphonic wheeze (silent chest = critical) |
| Croup | Stridor, retractions | Normal | Normal | Inspiratory stridor, barking cough |
| Bronchiolitis | Hyperinflation, tachypnoea, subcostal retractions | Hyperresonant | Reduced | Fine crackles, wheeze |
| Atelectasis | Reduced expansion ipsilateral | Dull | Absent/reduced | Absent/reduced breath sounds |
Sources: ROSEN's Emergency Medicine — Concepts and Clinical Practice; Tintinalli's Emergency Medicine: A Comprehensive Study; Mulholland and Greenfield's Surgery; Swanson's Family Medicine Review