Roadside accident had injury emergency management and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Based on authoritative surgical and emergency medicine textbooks, here is a comprehensive guide to roadside accident injury emergency management and treatment.
Roadside Accident — Emergency Management & Treatment
Epidemiology
Trauma is a leading cause of death and disability worldwide. Mortality follows a bimodal distribution:
- Immediate deaths — within minutes, from catastrophic CNS injury or major vascular hemorrhage
- Early deaths — within hours, from ongoing hemorrhage and severe injury
- Late deaths — days to weeks later, from organ failure and sepsis (dramatically reduced with modern care)
Phase 1: At the Scene (Bystander / Spontaneous Responder)
Before trained help arrives, even untrained bystanders can save lives.
Scene Safety First
- Assess for ongoing hazards: moving traffic, fire, fuel spills, unstable vehicles
- Do NOT approach until the scene is safe
- Call emergency services immediately
Stop the Bleed (Public First Aid Priority)
- Direct pressure — apply firm, continuous pressure to any bleeding wound
- Wound packing — pack deep wounds with gauze/cloth and maintain pressure
- Tourniquet — for severe limb bleeding that does not stop with pressure:
- Apply 2–3 inches (5–8 cm) proximal to the wound
- Apply on skin, not over clothing or a joint
- Tighten until bleeding stops
- Note the time of application
Tourniquet use in civilian trauma has demonstrated improved survival with no increase in complications.
Phase 2: EMS Arrival — Prehospital Assessment
xABCDE Framework (current PHTLS/ATLS standard)
| Step | Action |
|---|---|
| x | Exsanguinating external hemorrhage control (FIRST priority) |
| A | Airway management + cervical spine protection |
| B | Breathing and ventilation |
| C | Circulation / hemorrhagic shock |
| D | Disability — neurologic status |
| E | Exposure / Environment (examine fully; prevent hypothermia) |
x — Hemorrhage Control
- Direct pressure + wound packing with hemostatic gauze
- Tourniquet for uncontrolled extremity bleeding
- Exsanguinating hemorrhage is the #1 cause of preventable trauma death
A — Airway (with C-spine protection)
- Ask patient their name — a coherent verbal response confirms airway is patent
- Signs of airway compromise: stridor, hoarseness, gurgling, agitation, use of accessory muscles
- Basic maneuvers: chin lift / jaw thrust → manual clearance → oropharyngeal or nasopharyngeal airway (NPA contraindicated if facial trauma present)
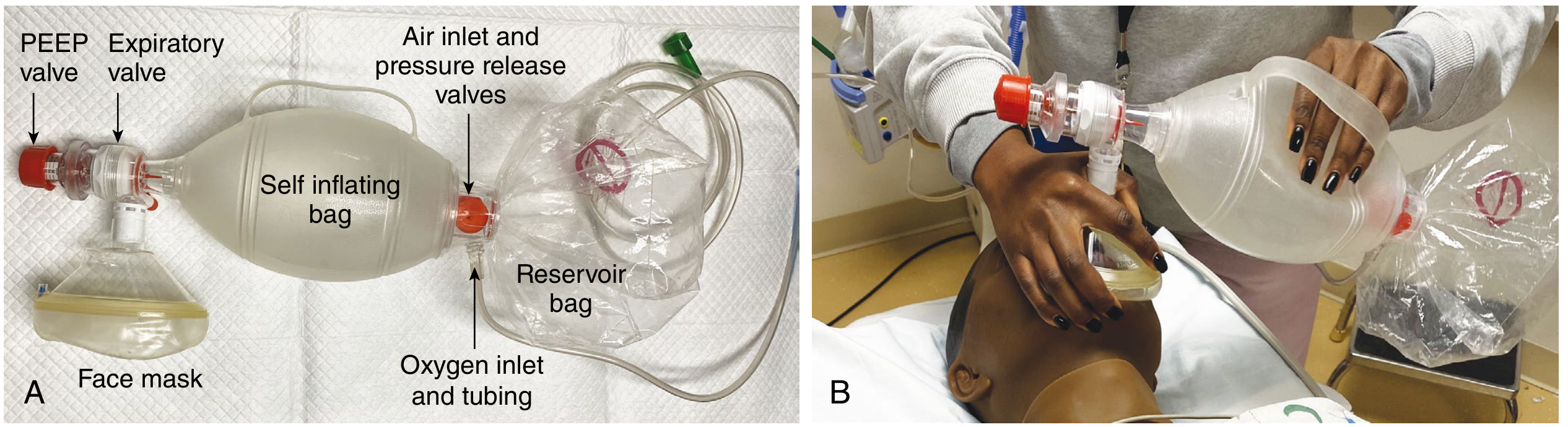
- Bag-valve-mask (BVM) ventilation with supplemental O₂
- Advanced: endotracheal intubation via RSI (Rapid Sequence Induction) if needed
- Surgical airway (cricothyroidotomy) if intubation fails
- For blunt trauma: maintain in-line cervical spine stabilization throughout
B — Breathing
- Auscultate bilateral breath sounds; inspect chest rise
- Absent breath sounds → suspect hemothorax or pneumothorax
- Tension pneumothorax (tracheal deviation, JVD, cyanosis, hemodynamic instability) → immediate needle decompression then chest tube
- Flail chest / large pulmonary contusion → ventilatory support
C — Circulation (Hemorrhagic Shock Recognition)
Signs: tachycardia, hypotension, weak/absent peripheral pulses, cool/pale skin, delayed capillary refill
Shock Index (SI) = Heart Rate ÷ Systolic BP — SI >0.9 is highly suggestive of critical bleeding
| Class | Blood Loss | HR | BP | Mental Status |
|---|---|---|---|---|
| I | <15% | Normal | Normal | Normal |
| II (Mild) | 15–30% | ↑ | Normal | Anxious |
| III (Moderate) | 31–40% | ↑↑ | ↓ | Confused |
| IV (Severe) | >40% | ↑↑ | ↓↓ | Lethargic/obtunded |
Blood pressure alone is NOT an early indicator of hemorrhagic shock — tachycardia appears first.
Management:
- Large-bore IV access (×2) → blood samples
- Balanced resuscitation: packed red cells + plasma + platelets (1:1:1 ratio)
- Massive transfusion protocol (MTP) if severe hemorrhage
- Tranexamic acid (TXA) — give within 3 hours of injury to reduce mortality from hemorrhage
- Avoid excessive crystalloid (worsens coagulopathy)
D — Disability (Neurologic Assessment)
- GCS (Glasgow Coma Scale): Eyes + Verbal + Motor
- Pupil size and reactivity
- Assess for traumatic brain injury (TBI)
- Spinal cord injury: hypotension without tachycardia = neurogenic shock → fluids + vasopressors
E — Exposure / Environment
- Fully expose patient (cut off clothing) to identify all injuries
- Prevent hypothermia — cover with blankets, use warm fluids
- Log roll to examine posterior body
- Check for: burns, penetrating wounds, seat belt sign, flank bruising, pelvic instability
Phase 3: In-Hospital Management
Secondary Survey
- Head-to-toe physical examination after life-threatening conditions are controlled
- Focused FAST ultrasound (eFAST): assess for blood in abdomen, pelvis, pericardium, pleural spaces
- Imaging: CXR, pelvis X-ray, CT (head, c-spine, chest/abdomen/pelvis as indicated)
Differential Diagnosis of Shock in Trauma
| Cause | Key Features | Immediate Action |
|---|---|---|
| Hemorrhagic (chest) | Absent breath sounds, rib fractures | Chest tube / thoracotomy |
| Hemorrhagic (abdomen) | Peritonitis, FAST +ve | Laparotomy / IR embolization |
| Pelvic fracture | Pelvic instability, hematoma | Pelvic binder → IR embolization |
| Cardiac tamponade | Beck's triad (muffled sounds, JVD, hypotension) | Pericardiocentesis / sternotomy |
| Tension pneumothorax | Tracheal deviation, tympanic percussion | Needle decompression |
| Neurogenic shock | Hypotension without tachycardia | IV fluids + vasopressors |
Fracture & Extremity Management
- Splint long bone fractures
- Assess neurovascular status distal to each injury (pulses, sensation, motor)
- Hard signs of vascular injury (pulsatile bleeding, expanding hematoma, absent pulses) → urgent angiogram or surgical repair
Wound Care
- Irrigate and cover open wounds
- Antibiotics for contaminated/open fractures
- Tetanus prophylaxis
Key Mnemonics Summary
| Mnemonic | Stands For |
|---|---|
| xABCDE | Exsanguination → Airway → Breathing → Circulation → Disability → Exposure |
| MARCH | Massive hemorrhage → Airway → Respiration → Circulation → Hypothermia |
| STOP THE BLEED | Public hemorrhage control: Apply pressure / Pack wound / Apply tourniquet |
Sources: Current Surgical Therapy 14e (Qasim; Ho & Alam); Sabiston Textbook of Surgery — Field Assessment & Trauma chapters
This is a shared conversation. Sign in to Orris to start your own chat.