Urine protein creatinine ratio
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Here is a comprehensive overview of the Urine Protein-to-Creatinine Ratio (UPCR / PCR):
Urine Protein-to-Creatinine Ratio (PCR)
What It Is
The PCR is obtained by dividing urinary protein concentration (mg/dL) by urinary creatinine concentration (mg/dL), expressed as mg/mg or mg/g. It is performed on a spot (random) or early morning urine sample and serves as a practical substitute for the 24-hour urine collection.
The underlying principle: because creatinine excretion is relatively constant throughout the day (~1 g/24h in healthy adults), dividing by urinary creatinine corrects for variations in urine concentration/dilution — the resulting ratio approximates grams of protein excreted per day.
Why PCR Instead of 24-Hour Urine?
| Feature | 24-hr urine | Spot PCR |
|---|---|---|
| Patient convenience | Cumbersome | Simple |
| Susceptibility to under/overcollection | Yes | No |
| Effect of hydration/diuresis | Yes | Minimized |
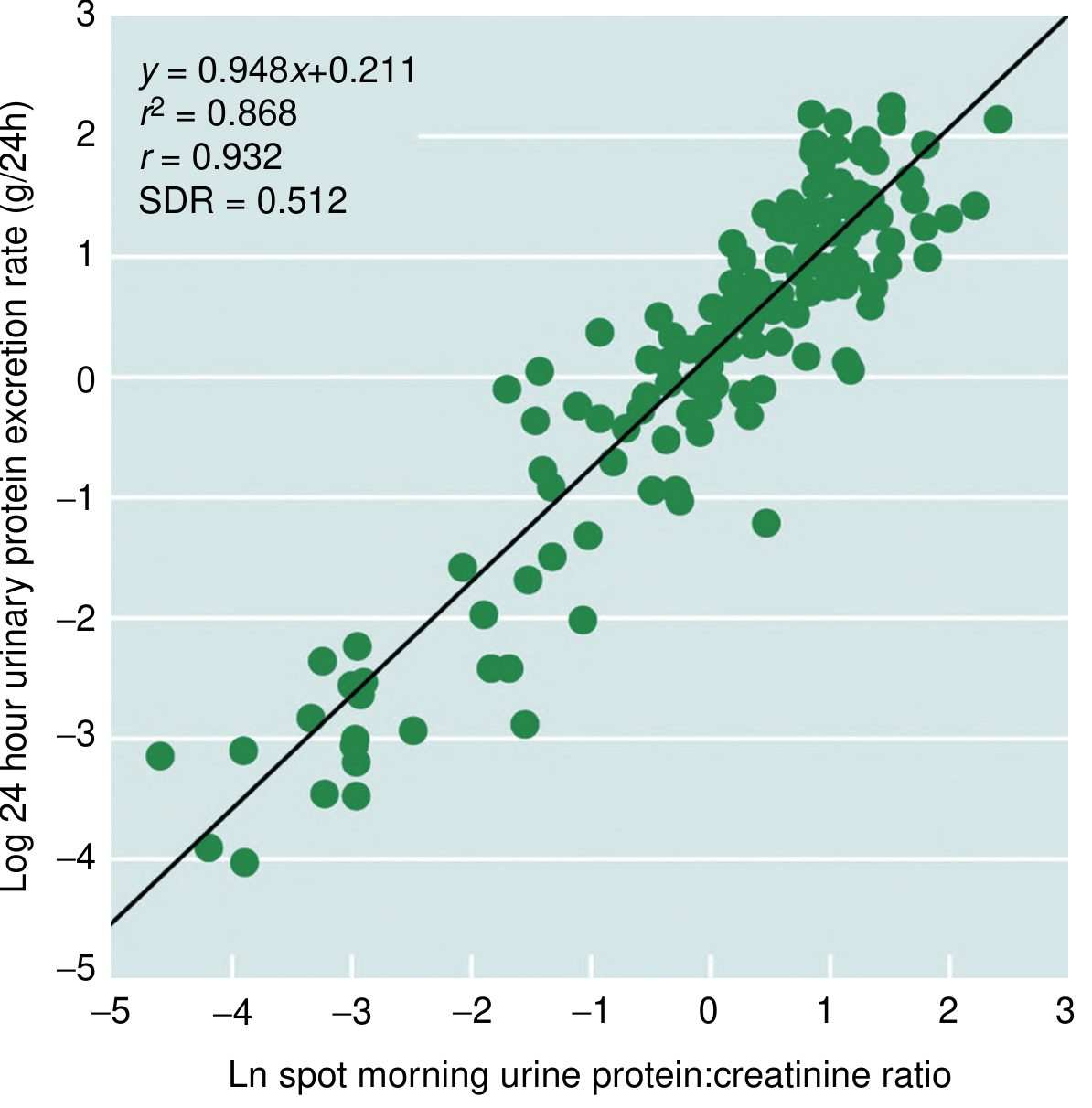
| Accuracy | Reference standard | Close correlation (r = 0.932) |
A strong correlation between spot morning PCR and 24-hour urine protein has been shown across a wide range of patients, including those with glomerulonephritis followed longitudinally during treatment (r² = 0.868). — National Kidney Foundation Primer on Kidney Diseases, 8e, p. 68
Normal Values
| Population | Normal PCR |
|---|---|
| Adults | < 150–200 mg/g (< 0.15–0.2 mg/mg) |
| Children > 2 years | < 0.2 mg/mg |
| Children < 2 years | < 0.5 mg/mg |
| Infants 6–24 months | < 500 mg/g |
Physiological proteinuria does not exceed 150 mg/24h in adults or 140 mg/m²/day in children. — Comprehensive Clinical Nephrology, 7th ed.
Clinical Interpretation Thresholds
| PCR (mg/g) | Interpretation |
|---|---|
| < 200 | Normal (> 2 years of age) |
| 200–500 | Non-nephrotic proteinuria |
| ≥ 3000–3500 | Nephrotic-range proteinuria |
- In lupus nephritis, a biopsy is considered when PCR ≥ 0.5 g/g (though this is not an absolute threshold — overall disease context matters). — Comprehensive Clinical Nephrology, 7th ed.
- PCR < 0.5 in pediatric minimal change disease warrants only ACE inhibitor treatment; nephrotic-range PCR without full nephrotic syndrome guides more aggressive therapy. — Brenner and Rector's The Kidney
PCR vs. Albumin-to-Creatinine Ratio (ACR)
KDIGO recommends ACR preferentially in adults with CKD because albuminuria is a reliable marker of CKD outcomes and glomerular permeability changes.
PCR is preferred over ACR in:
- Children — ACR may miss congenital disorders with non-albumin proteinuria
- Glomerulonephritis — KDIGO recommends PCR
- Tubulointerstitial disease — proteins are mostly tubular, not albumin → ACR gives false-negative
- Monoclonal gammopathies — light chains are not detected by ACR
— Comprehensive Clinical Nephrology, 7th ed.
Limitations and Pitfalls
- Low muscle mass (elderly, female patients, frail individuals): creatinine excretion is reduced → PCR overestimates true protein excretion
- High muscle mass (young athletic males): creatinine excretion > 1 g/day → PCR underestimates protein excretion
- Acute kidney injury / variable tubular secretion: impacts creatinine in the denominator
- Diurnal variation: protein excretion is higher during the day; morning specimens are preferred for reproducibility
- Poor correlation at very high protein levels and possible unreliability in lupus nephritis monitoring in some patients
- Dipstick positivity should always be confirmed with a formal PCR on a first-morning specimen — The Harriet Lane Handbook, 23rd ed.
Collection Technique (Pediatric)
- Child must empty bladder before bed
- If the child wakes at night, bladder should be emptied before returning to sleep
- The first void upon waking is the sample to collect
- Repeat abnormal results within 1–2 weeks (sooner if edema, hypertension, or other concerning features) — The Harriet Lane Handbook, 23rd ed.
Sources: Comprehensive Clinical Nephrology 7th ed. | NKF Primer on Kidney Diseases 8e | The Harriet Lane Handbook 23rd ed. | Brenner and Rector's The Kidney | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.