Antihistamine in chronic allergy
"antihistamine" AND "chronic allergic"
"H1 antihistamine" AND "allergic rhinitis"
Antihistamines in Chronic Allergy
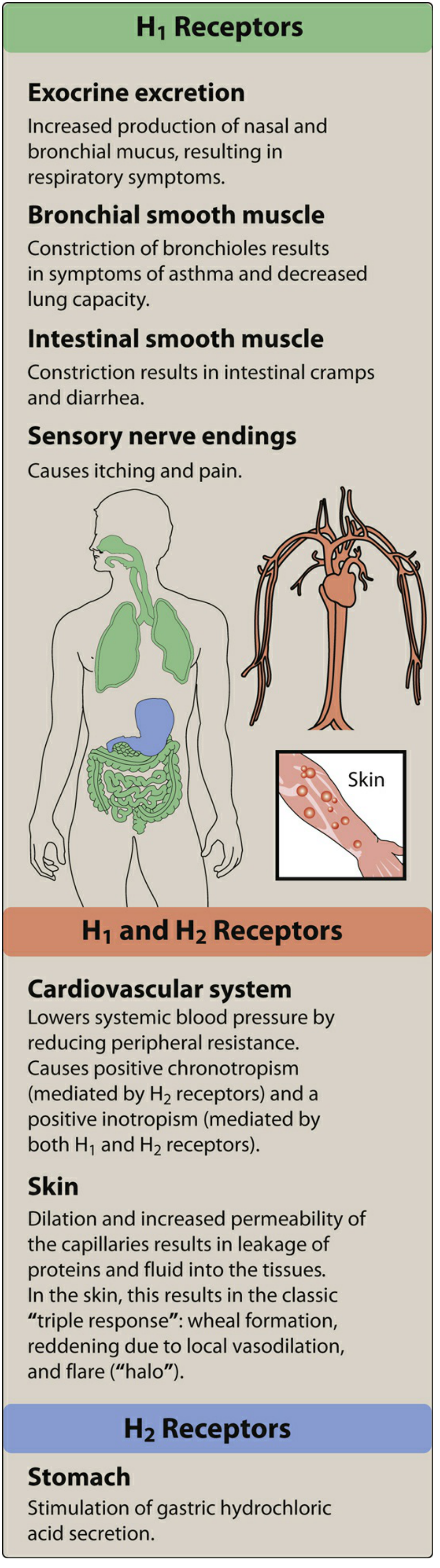
Mechanism of Action
- Increased production of nasal and bronchial mucus (rhinorrhea, congestion)
- Bronchoconstriction (smooth muscle contraction)
- Vasodilation and increased capillary permeability (wheal-and-flare, angioedema)
- Stimulation of sensory nerve endings (pruritus, pain)
Classification
First-Generation (Classic, Sedating)
| Drug | Class | Dose Interval |
|---|---|---|
| Diphenhydramine | Ethanolamine | Every 4-6 hrs |
| Chlorpheniramine | Alkylamine | Every 4-6 hrs |
| Hydroxyzine | Piperazine | Every 6-8 hrs |
| Promethazine | Phenothiazine | Every 6-8 hrs |
| Cyproheptadine | Piperidine | Every 6-8 hrs |
Second-Generation (Non-sedating / Low-sedating)
| Drug | Standard Dose | Key Feature |
|---|---|---|
| Cetirizine | 10 mg once daily | Most potent in skin wheal suppression |
| Levocetirizine | 5 mg once daily | Active enantiomer of cetirizine |
| Loratadine | 10 mg once daily | Extensive hepatic metabolism (CYP3A4) |
| Desloratadine | 5 mg once daily | Active metabolite of loratadine |
| Fexofenadine | 120-180 mg once daily | Minimal hepatic metabolism; safest in hepatic disease |
Role in Specific Chronic Allergic Conditions
1. Chronic Spontaneous Urticaria (CSU)
- Second-generation H1 antihistamines are the first-line treatment. The EAACI/GA2LEN/EDF/WAO consensus guidelines strongly recommend against using sedating (first-generation) H1 antihistamines as monotherapy. - Dermatology 2-Volume Set 5e, p. 474
- All major second-generation agents (cetirizine, loratadine, fexofenadine, desloratadine, levocetirizine) are superior to placebo in double-blind trials.
- If standard doses fail, doses can be up-titrated up to fourfold (e.g., cetirizine 40 mg/day, fexofenadine 720 mg/day). This is an off-label but guideline-recognized step.
- If one H1 antihistamine class fails, switching to a different chemical class is recommended before escalating.
- H2 antagonist add-on (e.g., famotidine): since ~15% of skin histamine receptors are H2-type, adding an H2 blocker may help some patients with CSU refractory to H1 blockers alone - though trial evidence is weak and not universally endorsed. - Rosen's Emergency Medicine, p. 779
- For H1-antihistamine-refractory CSU, omalizumab (anti-IgE monoclonal antibody) is the next step.
- Classic antihistamines at night can be added to a second-generation agent if sleep is disturbed by urticaria, with the caveat that next-day impairment (driving, machinery) remains a concern. - Dermatology 2-Volume Set 5e, p. 469
2. Allergic Rhinitis
- Antihistamines effectively control rhinorrhea, sneezing, and nasal itch but are less effective for nasal congestion. - Lippincott Illustrated Reviews: Pharmacology, p. 1313
- Intranasal corticosteroids remain the most effective agents for all rhinitis symptoms including congestion; antihistamines are used as adjuncts or in mild disease.
- Oral second-generation antihistamines (cetirizine, loratadine, fexofenadine) are preferred for long-term use.
- Intranasal antihistamines (azelastine, olopatadine) offer faster onset and are useful in both allergic and non-allergic rhinitis.
3. Atopic Dermatitis
- Evidence is limited. A meta-analysis of 16 studies failed to demonstrate a major benefit for either generation in atopic dermatitis. - Fitzpatrick's Dermatology, p. 3483
- Cetirizine showed a steroid-sparing benefit in children with severe atopic dermatitis (Early Treatment of the Atopic Child study), but no consistent benefit in moderate disease.
- First-generation agents may help with sleep disturbance related to nocturnal pruritus.
4. Allergic Conjunctivitis
- Topical ophthalmic antihistamines - azelastine, olopatadine, ketotifen, bepotastine - are preferred for targeted local delivery.
- Naphazoline-pheniramine (Naphcon-A) combinations are effective but rebound vasodilation can occur with prolonged use. - Textbook of Family Medicine 9e
5. Mastocytosis
- Higher-than-standard doses are often required (e.g., fexofenadine 360 mg in the morning + cetirizine 40 mg at night). - Fitzpatrick's Dermatology, p. 3483
Pharmacokinetics Comparison
| Property | 1st Generation | 2nd Generation |
|---|---|---|
| CNS penetration | High | Minimal |
| Duration of action | 4-6 hours | 12-24 hours (once daily) |
| Dosing | Multiple times/day | Once daily |
| Receptor selectivity | Low (also antimuscarinic, alpha-blocker) | High (H1-selective) |
| Hepatic metabolism | Extensive | Variable (fexofenadine minimal) |
| Tachyphylaxis | No tolerance over 3 months | No tolerance over 3 months |
Adverse Effects
- CNS: sedation, fatigue, dizziness, impaired cognition, paradoxical excitation in children
- Anticholinergic: dry mouth, blurred vision, urinary retention, constipation
- Potentiation of CNS depressants (alcohol, benzodiazepines, opioids)
- Elderly are particularly sensitive
- Most common: headache
- Cetirizine: mild sedation at higher doses (more than other 2nd-gen agents)
- Fexofenadine: least sedating; safest in renal/hepatic disease
- Drug interactions (CYP3A4): mizolastine, loratadine, ebastine - avoid with erythromycin, ketoconazole; fexofenadine, cetirizine, levocetirizine are safer - Dermatology 2-Volume Set 5e, p. 480
Special Populations
- Pregnancy: Loratadine and cetirizine are preferred (previously FDA Category B), especially in the 2nd and 3rd trimesters. Hydroxyzine is contraindicated in breastfeeding (seizure risk in infants). - Dermatology 2-Volume Set 5e, p. 488
- Renal impairment: Dose reduction needed for cetirizine, levocetirizine, fexofenadine (renally excreted unchanged).
- Hepatic impairment: Fexofenadine is the safest (minimal hepatic metabolism). Loratadine dose should be reduced.
- Elderly: Avoid first-generation antihistamines (falls, confusion, urinary retention - on the Beers Criteria list).
- Children: Second-generation agents preferred for long-term use; diphenhydramine causes paradoxical hyperactivity in young children.
Key Takeaway
Why they are insufficient alone in chronic allergy with pnd
Why Antihistamines Are Insufficient Alone in Chronic Allergy with Post-Nasal Drip (PND)
1. The Multi-Mediator Reality of Chronic Allergic Inflammation
Early Phase (0-30 minutes after allergen exposure)
- Histamine - causes sneezing, itch, and some rhinorrhea (antihistamines cover this)
- Prostaglandin D2 (PGD2) - potent vasodilator causing congestion
- Leukotrienes (LTC4, LTD4) - cause mucosal edema, mucus hypersecretion, and sustained congestion
- Tryptase, kininogens - activate kinins (bradykinin) causing glandular secretion and neural sensitization
Late Phase (4-10 hours after exposure)
- Eosinophil influx - releasing major basic protein, eosinophil cationic protein, causing epithelial damage and sustained mucus hypersecretion
- Cytokine surge: IL-1β, TNF-α (early); IL-5, IL-6, IL-8, GM-CSF, soluble ICAM-1 (late)
- Predominantly nasal congestion - the hallmark of the late phase. Antihistamines have virtually no effect on the late-phase response.
2. Nasal Congestion - The Core Problem in PND - Is Histamine-Independent
- Venous sinusoidal engorgement in the submucosal vascular plexus, regulated by sympathetic tone
- Leukotrienes and PGD2 acting on vascular smooth muscle
- Late-phase cellular inflammation (eosinophils, T cells, mast cells)
- Structural mucosal thickening from chronic inflammation
3. Neuropeptide-Driven Mechanisms
- Tachykinins (substance P) - stimulate mucus glands and cause vasodilation
- Calcitonin Gene-Related Peptide (CGRP) - potent vasodilator
- Neurokinin A - smooth muscle constrictor
- Vasoactive Intestinal Peptide (VIP) - from parasympathetic endings, a major driver of watery secretion and rhinorrhea
4. Why PND Specifically Is Poorly Controlled by Antihistamines
- Excess mucus production - from goblet cell hyperplasia and submucosal gland hypersecretion driven by VIP, substance P, and leukotrienes, not histamine
- Impaired mucociliary clearance - from chronic eosinophilic mucosal inflammation
- Postnasal mucus pooling and cough reflex sensitization - driven by C-fiber sensitization (TRPV1, TRPA1 channels) - again unrelated to H1 receptors
- Mucosal edema and nasal obstruction - forcing mucus posterior toward the nasopharynx
- Reduce mucosal edema/congestion
- Suppress eosinophilic infiltration
- Reduce cytokine-driven mucus hypersecretion
- Address goblet cell metaplasia from chronic inflammation
5. Chronic Inflammation Component
- Elevated baseline IL-1β, IL-6, IL-8 in nasal lavages
- Increased IL-4-positive mast cells in biopsy
- Subepithelial fibrosis and thickened basement membrane
6. What Is Needed Alongside Antihistamines
| Problem | Antihistamine covers? | What covers it |
|---|---|---|
| Sneezing, itch, watery rhinorrhea (early phase) | Yes (partial) | H1 antihistamines |
| Nasal congestion | No | Intranasal corticosteroids, decongestants, LTRAs |
| Late-phase mucus hypersecretion | No | Intranasal corticosteroids |
| Eosinophilic mucosal inflammation | No | Intranasal corticosteroids |
| Neuropeptide-driven secretion | No | Ipratropium (anticholinergic) for watery drip |
| Leukotriene-mediated edema | No | Montelukast (LTRA) |
| PND/chronic cough | No (partially at best) | Intranasal corticosteroids (first-line for UACS) |
| Mucosal remodeling/thickening | No | Intranasal corticosteroids |
Clinical Bottom Line
Search for recent clinical guidelines on upper airway cough syndrome (UACS) management
"upper airway cough syndrome" AND management
upper airway cough syndrome UACS clinical guidelines 2024 2025
"chronic cough" AND "postnasal" AND guideline
"chronic cough" AND "allergic rhinitis" AND treatment
"chronic cough" AND guideline
PMID: 34794590
PMID: 41385480
PMID: 37080877
"upper airway cough syndrome" OR "UACS" treatment rhinitis
"allergic rhinitis" AND management AND guideline
CHEST ACCP GOLD ERS chronic cough UACS upper airway cough syndrome guidelines 2023 2024 2025
PMID: 41324154
PMID: 41877472
PMID: 38408152
"cough hypersensitivity" AND "upper airway" AND treatment
PMID: 35000304
PMID: 39722320
PMID: 40544726
Recent Clinical Guidelines on Upper Airway Cough Syndrome (UACS) Management
1. ARIA-EAACI Guidelines 2024-2025 (Most Current - Published 2026)
Part I - Intranasal Treatments
- INAH + INCS (combined intranasal antihistamine + corticosteroid) is suggested over either agent alone - a new recommendation not present in prior ARIA guidelines
- INCS is recommended over intranasal antihistamine alone (stronger evidence)
- This is the first ARIA revision to formally endorse fixed-dose combination sprays (e.g., azelastine + fluticasone) as a preferred first-line option
- Decongestants: short-term use only; not recommended for chronic disease
Part II - Oral and Ocular Treatments
- INCS is recommended over oral antihistamines (OAH) - oral antihistamines are inferior to topical corticosteroids for controlling nasal congestion and PND
- OAH is recommended over leukotriene receptor antagonists (LTRA) - antihistamines preferred over montelukast for AR
- Adding LTRA to OAH is NOT recommended (recommendation against) - no added benefit
- For ocular symptoms: oral antihistamines are suggested over ocular antihistamines for patients with both nasal and ocular symptoms
These two papers together represent the current global standard of care for AR-driven UACS as of 2026.
2. German Respiratory Society (DGP) Cough Guidelines - 4th Edition (2025)
- Multi-specialty guideline (respiratory, allergy, ENT, gastroenterology, speech therapy, physiotherapy)
- Built on modified Delphi process with graded recommendations
- Diagnostic algorithms created for acute, subacute, and chronic cough
- UACS/rhinosinusitis explicitly included as a major chronic cough cause
- Addresses refractory chronic cough (RCC) - when UACS-directed therapy fails, points toward cough hypersensitivity syndrome management (neuromodulators)
- Available as a smartphone app for daily clinical use
3. French Guidelines for Chronic Cough in Adults (2023)
- Defines unexplained/refractory chronic cough (URCC) for patients persisting despite optimal treatment of UACS, GERD, and asthma
- Second-line evaluation framework when initial UACS-directed therapy fails
- For URCC: amitriptyline, pregabalin, gabapentin, or low-dose morphine combined with speech and/or physical therapy
- Introduces P2X3 receptor antagonists (gefapixant class) as an emerging treatment option
4. ACR Appropriateness Criteria - Chronic Cough (2021)
- Evidence-based radiological imaging guideline (RAND/UCLA + GRADE methods)
- UACS is listed as one of the most common causes of chronic cough alongside asthma and GERD
- Chest X-ray is the recommended initial imaging for chronic cough
- CT chest and sinus CT reserved for cases not responding to empirical UACS treatment
- Highlights the multifactorial nature of chronic cough
5. Immunotherapy for Inhalant Allergy - AAO-HNS Guideline (2024)
- Strong recommendation: Offer allergen immunotherapy (AIT) when symptoms are inadequately controlled with medications + allergen avoidance
- Both SCIT (subcutaneous) and SLIT (sublingual) are options - patients should be educated on differences in risk, benefit, convenience, and cost
- Potential disease-modifying benefits: prevention of new sensitizations, reduced risk of asthma development, sustained benefit after stopping therapy
- Minimum 3 years of treatment for patients with good symptomatic control
- Contraindications: pregnancy, uncontrolled asthma, inability to tolerate injectable epinephrine
6. Therapeutic Advances in Chronic Cough - 2025 Review (ACAAI)
- Confirms the "Big 3" triad of chronic cough causes: UACS, GERD/LPR, and asthma/eosinophilic bronchitis (assuming normal CXR and no ACE inhibitor use)
- If cough persists despite full treatment of all three, it is classified as refractory chronic cough (RCC) - thought to arise from cough hypersensitivity syndrome (neuronal dysregulation, peripheral + central)
- Gefapixant (P2X3 antagonist): approved in EU, UK, Switzerland, Japan - not yet approved in USA or Canada (as of 2025)
- Speech therapy (speech language pathology - SLP) is established as part of RCC management
Summary: Current UACS Management Algorithm (Guideline-Based, 2026)
Chronic cough (>8 weeks) with suspected UACS
|
v
Step 1: Empiric treatment (no cause proven yet)
- INCS (fluticasone, mometasone, budesonide) - FIRST LINE
- ± INAH (azelastine) or fixed INAH+INCS combo
- 2nd-gen oral antihistamine if sneezing/rhinorrhea dominant
- Saline nasal irrigation (adjunct)
- Avoid LTRA add-on to OAH (no benefit per ARIA 2025)
|
v
Step 2: If persistent - investigate cause
- Allergy testing → consider AIT if AR confirmed (AAO-HNS 2024)
- Rule out chronic rhinosinusitis (nasal endoscopy, CT sinuses)
- Rule out non-allergic rhinitis → ipratropium for watery drip
- Short-course nasal decongestant (≤3-5 days)
|
v
Step 3: Refractory UACS or co-existing causes
- Assess for GERD (empiric PPI trial) and asthma
- Speech language pathology (SLP/physiotherapy cough suppression)
- Neuromodulators (gabapentin, pregabalin, amitriptyline) if cough hypersensitivity syndrome
- Gefapixant (P2X3 antagonist) - where approved
Key Guideline Shifts (2024-2026 Updates)
| Area | Old recommendation | New (ARIA 2024-2025) |
|---|---|---|
| Intranasal treatment | INCS alone first-line | INAH+INCS combo suggested over INCS alone |
| Oral antihistamine vs INCS | Both options | INCS recommended over OAH |
| LTRA (montelukast) | Sometimes added to OAH | Recommend against adding LTRA to OAH |
| Immunotherapy | Specialist referral | Offer when meds + avoidance fail (strong rec) |
| Refractory cough | Limited options | P2X3 antagonists (gefapixant) - approved EU/Japan |
Why montelukast against recommend
montelukast allergic rhinitis efficacy antihistamine comparison
montelukast neuropsychiatric adverse effects black box warning
PMID: 41170705
PMID: 37758273
Why ARIA 2024-2025 Recommends Against Adding Montelukast to Oral Antihistamines
Reason 1: Weak and Marginal Added Efficacy
What the evidence shows
- Combination therapy improved daytime symptoms modestly (SMD = 0.25; small effect)
- No significant benefit for nighttime symptoms (SMD = 0.10; CI crossed zero)
- No significant benefit for quality of life (RQLQ scores) (SMD = 0.11; CI crossed zero)
- Only the levocetirizine-montelukast combination showed significant benefit across multiple symptom domains; other combinations (loratadine, desloratadine) showed limited or inconsistent gains
Mechanistic reason montelukast adds little
- Antihistamine handles: sneezing, itch, watery rhinorrhea (histamine-mediated)
- Montelukast handles: congestion, mucus (leukotriene-mediated) - but modestly
- INCS handles all of the above more effectively than either oral agent
Reason 2: FDA Black Box Warning - Neuropsychiatric Events (2020)
"Because of the risk of neuropsychiatric events, the risks may outweigh the benefits in patients with allergic rhinitis. Reserve use for patients with inadequate response or intolerance to alternative therapies."
What neuropsychiatric events were reported?
- Agitation, aggression
- Anxiousness, depression
- Sleep disturbances, abnormal dreams, insomnia
- Suicidal thinking and behavior
- Hallucinations, memory impairment, tremor
What the systematic review found
- No significant association with suicide-related events (6 observational studies)
- No association with ICD-10-coded depression (3 observational studies + RCT review)
- BUT: 4 studies using antidepressant prescriptions as the outcome found significant associations
- Anxiety and sleeping disorders were consistently associated in 2 large observational studies in adults, and confirmed in 9 pharmacovigilance studies
- Older adults appeared particularly susceptible to anxiety and sleeping disorders
- Children did not replicate the anxiety/sleep findings in 2 pediatric observational studies
Reason 3: Risk-Benefit Calculus Tilts Negative for AR Specifically
| Condition | FDA position |
|---|---|
| Asthma | May still be appropriate when other options fail |
| Allergic rhinitis | Risks may outweigh benefits - restrict to inadequate responders |
Summary Table
| Factor | Detail |
|---|---|
| Added efficacy (vs INCS) | INCS superior to OAH alone and OAH+LTRA for all AR symptoms |
| Added efficacy (vs OAH alone) | Only small benefit in daytime symptoms; no significant benefit for nighttime or QoL |
| Neuropsychiatric risk | FDA black box warning (2020): suicidal ideation, anxiety, sleep disturbance |
| Guideline recommendation | ARIA 2024-2025: recommend against adding LTRA to OAH in AR |
| When montelukast IS still used | Asthma + AR comorbidity, aspirin-exacerbated respiratory disease, exercise-induced bronchoconstriction, urticaria (aspirin-sensitive), CRSwNP as adjunct |