Chest pain and MI comparison
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
chest pain differential diagnosis myocardial infarction ECG ST elevation
Here is a comprehensive comparison of Chest Pain as a symptom versus Myocardial Infarction (MI) as a specific diagnosis, drawing from Goldman-Cecil Medicine, Robbins Pathology, and Ganong's Review of Medical Physiology.
Chest Pain vs. Myocardial Infarction — A Clinical Comparison
1. Overview
| Feature | Chest Pain (Symptom) | Myocardial Infarction (Diagnosis) |
|---|---|---|
| Nature | Cardinal symptom — not a diagnosis | Specific disease entity with defined criteria |
| Definition | Discomfort/pain in the thoracic region | Necrosis of myocardium due to ischemia |
| Diagnostic criteria | None — it is a presenting complaint | Abnormal cardiac biomarkers + evidence of acute myocardial ischemia (2018 joint task force) |
| Causes | Broad — cardiac, pulmonary, GI, MSK, vascular | Coronary artery occlusion (≥90% thrombotic) |
2. Causes of Chest Pain (Differential Diagnosis)
Chest pain has a vast differential. Clinicians must rule out life-threatening causes first:
Cardiac (ischemic)
- Acute MI
- Unstable angina / Acute Coronary Syndrome (ACS)
- Stable angina pectoris
Cardiac (non-ischemic)
- Pericarditis — pain may mimic MI; key finding is a pericardial rub; ECG shows diffuse concave ST elevation (vs. localized, convex "tombstone" in STEMI)
- Aortic dissection — sudden, severe pain radiating to the back; hypertension, Marfan syndrome risk factors
Pulmonary
- Pulmonary embolism — pleuritic pain + dyspnea ± hemoptysis
- Pulmonary hypertension — exertional pain + severe dyspnea ± cyanosis
- Pneumonia, pleuritis, pneumothorax
Gastrointestinal
- Esophageal reflux or spasm
- Peptic ulcer disease, cholecystitis
Musculoskeletal
- Chest wall pain (most common in children)
- Precordial catch syndrome (Texidor's twinge)
Women and older individuals may not experience classic anginal chest pain even with advanced coronary disease. — Goldman-Cecil Medicine
3. Myocardial Infarction: Pathogenesis
The typical MI sequence (Robbins Pathology):
- Plaque disruption — atherosclerotic plaque erodes/ruptures due to endothelial injury, mechanical forces, or intraplaque hemorrhage
- Platelet activation — adhesion, aggregation, release of TXA₂, ADP, serotonin → vasospasm
- Coagulation cascade — tissue factor exposure → thrombus growth
- Complete occlusion within minutes → ischemia → necrosis
Angiography within 4 hours of MI onset shows coronary thrombosis in ~90% of cases. By 12–24 hours, evidence drops to 60%, as some thrombi lyse spontaneously. — Robbins & Kumar Basic Pathology
Non-atherosclerotic causes (~10%): vasospasm (Prinzmetal angina), embolism from mural thrombi (e.g., AF), vasculitis, amyloid, sickle cell disease.
4. ACS Spectrum: Distinguishing MI from Other Chest Pain
| Condition | Troponin | ST Changes | Definition |
|---|---|---|---|
| Unstable Angina | ❌ Negative | No ST elevation | Cardiac chest pain at rest/worsening, no necrosis |
| NSTEMI | ✅ Positive | No ST elevation | Cardiac pain + myonecrosis, no ST elevation |
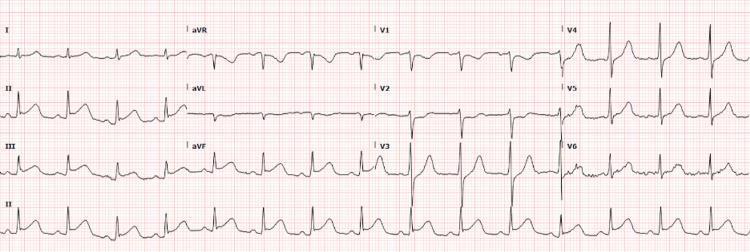
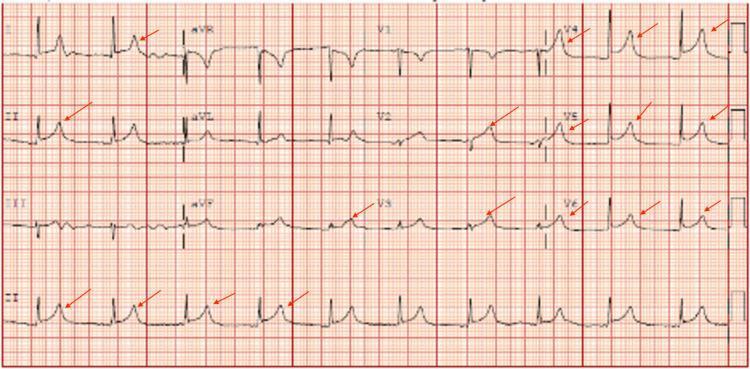
| STEMI | ✅ Positive | Persistent ST elevation (>20 min) | Full-thickness ischemia, acute occlusion |
The chest discomfort of unstable angina is clinically indistinguishable from that of acute MI, except it may be more clearly precipitated by activity and more rapidly responsive to antianginal therapy. — Goldman-Cecil Medicine
5. ECG Changes in MI (Ganong's Physiology)
Three sequential electrical events occur after coronary occlusion:
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization | Out of infarct | ST segment elevation |
| Decreased resting membrane potential | Into infarct | TQ depression → manifest as ST elevation |
| Delayed depolarization | Out of infarct | ST segment elevation |
Evolution over time:
- Acute (hours): ST elevation — the hallmark of STEMI
- Days–weeks: ST normalizes; Q waves develop (electrically silent scar)
- Non-Q-wave infarcts: less severe but higher risk of reinfarction
6. Key Clinical Distinguishing Features
| Feature | Suggests MI/ACS | Suggests Non-Cardiac |
|---|---|---|
| Quality | Pressure, squeezing, heaviness | Sharp, stabbing, pleuritic |
| Radiation | Neck, shoulder, arm, jaw | Localized, no radiation |
| Duration | >20 min (STEMI), variable (UA) | Seconds or reproduces on palpation |
| Triggers | Exertion or rest | Inspiration, movement, food |
| ECG | Localized ST elevation, Q waves | Diffuse ST (pericarditis), normal |
| Biomarkers | Troponin elevated | Normal troponin |
| Response to nitrates | Often improves | Variable |
| Associated symptoms | Diaphoresis, nausea, dyspnea | Fever (pericarditis), dyspnea (PE) |
7. Therapeutic Implications
- STEMI: Early thrombolysis and/or angioplasty (PCI) is highly effective in limiting necrosis — every minute counts
- NSTEMI/UA: Antiplatelet therapy, anticoagulation, risk stratification with serial troponins
- Type 2 MI: Treat the underlying cause (e.g., tachycardia, anemia, hypotension)
- Aortic dissection: Thrombolytics are contraindicated — diagnosis must be excluded first
- Pericarditis: NSAIDs/colchicine; steroids avoided in acute setting
Sources: Goldman-Cecil Medicine (International Ed.) · Robbins & Kumar Basic Pathology · Ganong's Review of Medical Physiology (26th Ed.) · Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.