Acne vulgaris treatment
Reading File
Finding Sources
Searching PubMed
"acne vulgaris"[MeSH Terms] AND treatment
Searching the Web
acne vulgaris treatment guidelines 2024 2025
Reading File
Finding Sources
Searching Images
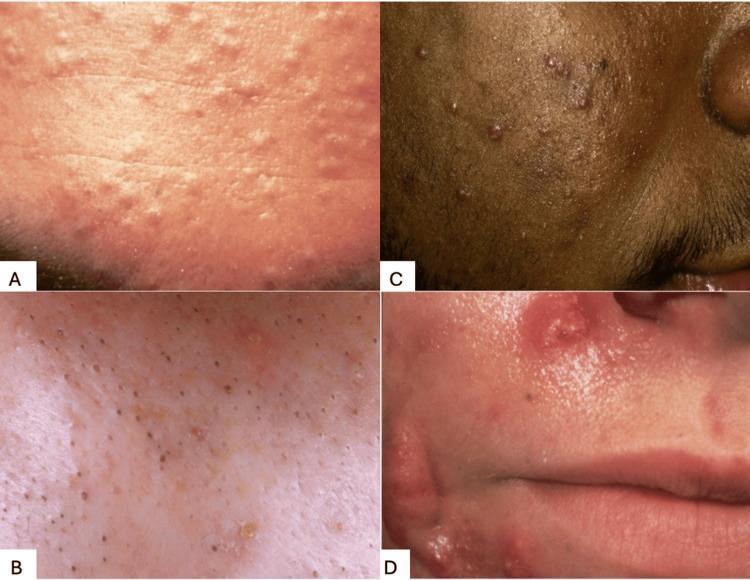
acne vulgaris lesions comedones papules pustules
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile it.
Acne Vulgaris: Treatment
Overview & Pathogenesis
Acne vulgaris is a multifactorial disorder of the pilosebaceous unit, affecting ~85% of adolescents aged 12–24 and persisting into adulthood in 35% of women and 20% of men in their 30s. Four key pathogenic mechanisms drive the disease:
- Increased sebum production — androgen-driven (peaks at puberty)
- Abnormal follicular keratinization — retention of keratin and sebum forms comedones
- Cutibacterium acnes colonization — releases free fatty acids from sebum, triggering inflammation
- Inflammatory cascade — rupture of comedone wall → foreign-body reaction → papules, pustules, nodules
Severity Classification & Treatment Algorithm
Treatment is severity-tiered. The goal is to normalize follicular keratinization, reduce C. acnes, decrease sebum production, and suppress inflammation.
| Severity | Characteristics | First-Line Treatment | Escalation |
|---|---|---|---|
| Mild | Several papules, pustules, and/or comedones; no nodules | Topical retinoid ± BPO ± topical antibiotic | Increase retinoid strength; change to leave-on BPO |
| Moderate | Multiple papules/pustules; few nodules | Topical retinoid + BPO ± oral antibiotic ± hormonal therapy (females) | Add oral antibiotic or hormonal therapy; consider isotretinoin |
| Severe | Numerous papules/pustules + multiple nodules | Topical retinoid + BPO + oral antibiotic ± hormonal therapy (females); OR isotretinoin | Switch to isotretinoin |
| Very severe / Acne fulminans | Numerous nodules with conglobate or hemorrhagic lesions ± systemic symptoms | Prednisone ± low-dose isotretinoin (start low) | Slow isotretinoin dose escalation |
(Dermatology 2-Volume Set 5e, Table 36.4)
Topical Therapies
Retinoids (first-line for all grades)
- Agents: tretinoin, adapalene, tazarotene, trifarotene
- Mechanism: normalize follicular keratinization, prevent comedone formation, enhance penetration of other agents
- Start at lower strength to minimize irritation; titrate up as tolerated
- Apply at night; sun protection is essential
Benzoyl Peroxide (BPO)
- Mechanism: bactericidal against C. acnes; does not induce antibiotic resistance
- Available as washes or leave-on preparations (2.5–10%)
- Should always be combined with topical antibiotics to prevent resistance
Topical Antibiotics
- Clindamycin (most common) and erythromycin
- Must not be used as monotherapy — always combine with BPO to prevent C. acnes resistance
- Limited to acute control phases; avoid long-term monotherapy
Alternative Topicals
| Agent | Notes |
|---|---|
| Azelaic acid (15–20%) | Anti-inflammatory, comedolytic; safe in pregnancy; also treats post-inflammatory hyperpigmentation |
| Dapsone (5–7.5% gel) | Particularly effective in adult female acne |
| Clascoterone (1% cream) | FDA-approved topical androgen receptor blocker; useful when systemic hormonal therapy is not appropriate |
| Salicylic acid | Mild comedolytic; OTC; adjunct only |
Systemic Therapies
Oral Antibiotics
- Doxycycline and minocycline (100 mg twice daily, or low-dose extended-release) — most used
- Anti-inflammatory effects independent of antibacterial activity
- Expect response at 3 months
- Limit duration to reduce resistance; always co-prescribe BPO
- Sarecycline — narrow-spectrum tetracycline (FDA-approved 2018); less GI side effects, reduced resistance potential
Hormonal Therapy (females only)
- Combined oral contraceptives (OCPs): several FDA-approved for acne (norgestimate/ethinyl estradiol; norethindrone acetate/ethinyl estradiol; drospirenone/ethinyl estradiol)
- Spironolactone (50–200 mg/day): anti-androgen; safe, effective, and durable in women; particularly useful for adult female acne
- Not appropriate for males (gynecomastia risk)
Isotretinoin (13-cis-retinoic acid)
- Indications: severe nodulocystic acne; moderate acne unresponsive to conventional therapy; acne causing significant psychosocial distress or scarring
- Mechanism: reduces sebaceous gland size and activity (~90% reduction in sebum); normalizes desquamation; anti-inflammatory
- Dosing: weight-based; cumulative dose approach (~120–150 mg/kg total)
- Monitoring: lipids, liver function, CBC; monthly pregnancy tests in women of childbearing potential
- iPLEDGE program (USA): mandatory enrollment to prevent teratogenicity; two negative pregnancy tests before initiation; monthly negative test before each refill
- Common side effects: dry skin, cheilitis, dry eyes, elevated triglycerides
- Severe/rare: teratogenicity (Category X), potential IBD risk (controversial), mood changes (monitor)
- Results are excellent in appropriately selected patients; often produces long-term remission
Acne Fulminans (Very Severe)
A rare, explosive form with ulcerative nodules, systemic symptoms (fever, arthralgia, leukocytosis). Treatment:
- Oral prednisolone 0.5–1 mg/kg/day to suppress acute inflammation
- Add low-dose isotretinoin once inflammation subsides; slow titration upward
Special Considerations
| Scenario | Approach |
|---|---|
| Pregnancy | Azelaic acid, topical erythromycin, topical clindamycin (avoid systemic tetracyclines and isotretinoin — both contraindicated) |
| Hormonal acne (adult women) | Spironolactone + OCP ± topical retinoid; clascoterone if systemic hormones contraindicated |
| Post-inflammatory hyperpigmentation | Azelaic acid; topical retinoids; photoprotection |
| Acne scars | Isotretinoin first to control active disease; then procedural options (microneedling, chemical peels, laser resurfacing) |
| Drug-induced acne | Identify and remove offending agent (glucocorticoids, lithium, isoniazid, androgenic steroids, phenytoin) |
| PCOS-associated acne | Hormonal therapy is central; treat underlying PCOS |
Practical Pearls
- Overly vigorous scrubbing aggravates acne — gentle cleansing is recommended
- Comedogenic cosmetics and hair products can worsen acne; non-comedogenic formulations preferred
- Maintenance therapy after achieving control (typically retinoid ± BPO) is essential — acne commonly recurs
- Response to oral antibiotics expected at 3 months; if inadequate, reassess adherence or escalate to isotretinoin
- Lack of response should prompt evaluation for endocrine disorders (PCOS, hyperandrogenism, Cushing's) or medication-induced acne
Recent Evidence (2024–2025)
- A 2025 systematic review (PMID 39269130) highlights the cutaneous microbiome's role in acne pathogenesis, suggesting future probiotic/microbiome-modulating treatments may complement standard therapy.
- A 2025 meta-analysis (PMID 39509291) found that combining isotretinoin with laser/light-based treatments does not provide superior outcomes over isotretinoin alone for active acne.
- A 2024 network meta-analysis (PMID 39110247) on acne scarring found microneedling combined with PRP or other adjuncts offers greater improvement in scar appearance than microneedling alone.
Sources: Harrison's Principles of Internal Medicine 22e (2025); Dermatology 2-Volume Set 5e; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.